
Quality Improvement Case Series
Peri-Implant Fracture After Distal Femur Percutaneous Epiphysiodesis Using Transphyseal Screws
1University of Colorado School of Medicine, Department of Orthopedics, Aurora, CO; 2Children’s Hospital Colorado, Orthopedics Institute, Aurora, CO
Correspondence: Julia S. Sanders, MD, Children’s Hospital Colorado, Department of Orthopedics, 13123 E. 16th Ave., Box 060, Aurora, CO 80045. E-mail: [email protected]
Received: March 6, 2023; Accepted: March 29, 2023; Published: May 1, 2023
Volume 5, Number 2, May 2023
Abstract
Percutaneous epiphysiodesis using transphyseal screws (PETS) is a commonly used technique for guided growth. Technical challenges specific to the distal femur include difficulty obtaining a start point, accurately predicting trajectory across the physis, and achieving adequate thread purchase in the epiphysis. A previously unreported complication is peri-implant fracture. We present a case of peri-implant fracture after epiphysiodesis for leg length discrepancy, ultimately treated with retrograde intramedullary nail fixation. We recommend a modified PETS technique and close attention to orthopaedic principles to avoid this unfortunate complication.
Key Concepts
- Stress riser fractures can occur due to low bone strength and high mechanical stress, cortical defects, changes in stiffness at the ends of a construct, and changes in cross-sectional area of the bone.
- Percutaneous epiphysiodesis using cannulated screws (PETS) may be safely used for guided growth of the distal femur when the surgeon can utilize a single start point, with trajectory through the physis at the junction of the lateral and middle thirds, to allow adequate purchase in the epiphysis, and to avoid stress riser creation.
- A modified technique utilizing retrograde guidewire placement with antegrade screw placement may help mitigate technical challenges and avoid complication.
Introduction
There are numerous techniques for performing guided growth in pediatric patients with a multitude of lower extremity deformities. Common indications for epiphysiodesis and hemi-epiphysiodesis include leg length discrepancies (LLD), fixed knee flexion contracture, upper limb deformities, and progressive angular deformities of the lower extremities of variable etiologies from congenital to posttraumatic.1 These deformities can result in gait disturbances, pain, compensatory changes in other parts of the skeleton, and overall diminished function or quality of life. Epiphysiodesis alone is effective in certain patient populations with LLDs or deformities that are significant enough to cause functional impairment but not so severe that they require more invasive procedures such as lengthening or osteotomies. This typically includes patients with a predicted leg length discrepancy at maturity of 2-5 cm as well as sufficient remaining growth to allow for adequate angular correction.2
The physiology of epiphysiodesis involves growth arrest through the process of inducing a bone bridge at the indicated physis. Historically, this was done through an open excision of the physis and replacement of a bone block.3 This has since been replaced with a variety of percutaneous techniques including drilling of the physis itself, physeal spanning plates, and isolated screws. Percutaneous epiphysiodesis using transphyseal screws (PETS) is now one of the most common of these techniques and utilizes the compressive forces of cannulated screws to inhibit activity at growth plate.4 Common complications with this technique include technical challenges with placement of the screws, difficulty with hardware removal, under/overcorrection, asymmetric physeal suppression secondary to screw migration, and hardware failure with screw breakage.5 While the concept of peri-implant fracture is well known in orthopaedics, to our knowledge, it has not been well-documented as a possible complication of PETS. Peri-implant fracture is defined as a stress riser fracture around an implant that can be a prosthesis, plate, nail screw, pin, etc.6 We present a case of PETS of the distal femur complicated by peri-implant fracture requiring surgical intervention.
Case Report
A 14 + 8-year-old male with a history of Perthes disease of the right hip and leg length discrepancy who presented to clinic for evaluation. Imaging at the initial visit showed a bone age of 14 years and a leg length discrepancy of 3.3 cm (left: 88.7 cm, right: 85.4 cm). Femur length specifically was found to be 48.1 cm on the left and 44.9 cm on the right (Figure 1).
Figure 1. Standing lower extremity films demonstrating leg length discrepancy, left greater than right, of 3.3 cm.

The decision was made to proceed with left distal femur epiphysiodesis to mitigate leg length discrepancy at skeletal maturity. We proceeded with left distal femur PETS. Intraoperatively, guidewires were placed percutaneously in an antegrade fashion. Several attempts were made on the medial cortex in an attempt to achieve optimal screw trajectory through the physis. Otherwise, the procedure was uncomplicated (Figure 2).
Figure 2. Intraoperative fluoroscopy demonstrating antegrade placement of two fully threaded 6.5 mm cannulated stainless-steel screws.

The patient recovered without any acute complications at his postoperative visits until he was 2 months out from surgery. During box jumps at a supervised physical therapy session, he felt a snap and had immediate pain and inability to bear weight. He was found to have a complete, displaced, peri-implant femur fracture at the proximal level of the transphyseal screws (Figure 3).
Figure 3. Plain radiographs demonstrating left distal femoral peri-implant fracture.

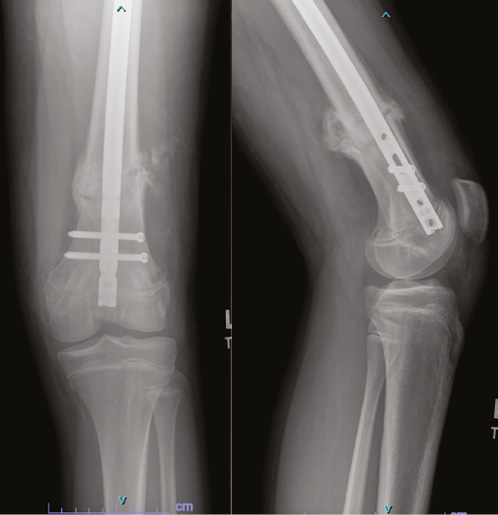
The patient underwent hardware removal of transphyseal screws and rigid intramedullary nail fixation at an outside hospital close to his home. He was seen in our clinic 4 months postoperatively from his initial surgery and 2 months postoperatively from his fracture fixation and was overall doing well without pain (Figure 4).
Figure 4. Two months following screw removal and retrograde intramedullary nail fixation.
At his most recent visit (10 months status-post epiphysiodesis) his leg length discrepancy was 2.4 cm (Figure 5).
Figure 5. Most recent follow-up demonstrating 2.4 cm LLD.

Further intervention to address residual discrepancy was declined by the family due to his prior complication. He is currently doing well with a shoe insert and is back to competitive sports. His right hip is currently asymptomatic and is being monitored by our Hip Preservation team.
Discussion
PETS is a common technique to perform permanent epiphysiodesis in pediatric patients with mild, yet clinically significant, leg length discrepancies. This method is preferred for its minimally invasive nature, minimal postoperative pain, and low complication rate. When complications do occur in these cases, they tend to involve issues with the final correction (overcorrection, undercorrection, coronal malalignment) or hardware (symptomatic hardware, screw migration, difficulty with hardware removal, screw breakage).5 In this case, we present a patient who underwent distal femur PETS complicated by peri-implant femur fracture.
While a case report exists describing a distal femur stress fracture at the site of a tension band plate (TBP) used for epiphysiodesis, a peri-implant fracture after cannulated screw placement for guided growth in the distal femur has not been described.7 Epiphysiodesis with TBP and PETS have been shown to have similar efficacy for managing LLD, but studies have shown that TBP tends to have similar to significantly increased complication rates, again, most commonly involving deformity, wound complications, and knee pain rather than fracture.8 While there is particular concern for under-correction if not placed correctly with sufficient threads crossing the physis, PETS has been shown to be an overall effective and low-risk procedure, with only 3.7% requiring revision procedure for broken implant or angular deformity.9
While there is minimal literature regarding the relationship between strain and stress riser fractures at the distal femur, there is significantly more knowledge about the proximal femur. The subtrochanteric region of the femur has been shown to be subject to high strain, and as such fixation anchored in this region has an increased risk for peri-implant fracture as a result of increased stress concentration.10 Example of this can be seen in constructs such as femoral neck fixation with cannulated screws that have start points distal to the lesser trochanter, short antegrade cephalo-medullary nails, and femoral shaft retrograde intramedullary nails that end in the subtrochanteric region.10 The high-strain environment of the subtrochanteric region of the proximal femur is attributed to multiple biomechanical factors, including tensile and compressive stresses produced by weight-bearing and muscle action as well as trajectories and patterns of trabecular and cortical bone.11 Cortical bone is stiffer with a higher resistance to stress, whereas trabecular bone is porous with a high resistance to strain.12 The metaphyseal-diaphyseal (MD) junction of the distal femur is anatomically similar to the subtrochanteric region of the proximal femur in that it is a transition point in the bone in terms of thickness of cortical bone and trabecular bone width. Implant placement in this transition zone leads to an abrupt change in stiffness that increases the stress concentration at the end of the construct.
We believe that the peri-implant fracture, in this case, occurred from the MD junctional positioning of the cannulated screw heads creating a stress riser at the proximal end of the construct. Stress riser fractures occur because of low bone strength and high mechanical stress as well as cortical defects, changes in stiffness at the ends of a construct, changes in cross-sectional area of the bone, and non-displaced fracture lines. Areas of stress concentration, such as empty screw hole or end of a stiff construct, tend to fracture when they experience torsional or tension forces.6 It has been shown that cortical perforations, such as a hole from prior screw or pin tract, pose the biggest risk for stress-riser fracture.13
In this case, our patient had multiple factors for local increase in stress intensity, including change in material stiffness from metal screw to bone, multiple guide pin passes leading to a pin tract immediately proximal to the screw creating a hole, and the change in cross-sectional area at the metaphyseal-diaphyseal (MD) junction. Also notably, the two screw heads were nearly at the same level on opposite cortices just distal to the lateral cortical hole, increasing the stiffness at the end of the construct and further increasing the stress at that location. Another consideration is screw material. Stainless steel implants are significantly stiffer than bone, while titanium implants more closely match the modulus of elasticity of bone. The use of titanium alloy implants has been postulated to decrease stress riser production and therefore lower complication rates in certain fracture constructs,14 although no literature exists regarding the use of stainless steel versus titanium implants for guided growth in the pediatric population.
Potential reasons for complication, in this case, include screw head positioning at the MD junction as well as multiple passes for guide pin placement leading to cortical holes. Both of these issues can be avoided with an alternative technique utilizing retrograde guide pin placement through the epiphysis, guide pin advancement, followed by antegrade screw placement (please refer to additional links for a video demonstrating this technique). With an epiphyseal start point, the surgeon can create tracts as needed to ensure appropriate placement of the guide pin, and subsequently the cannulated screw, through the physis and into the metaphysis without creating multiple proximal cortical holes. This avoids creating a stress riser in the diaphysis or MD junction of the femur that have lower cross-sectional areas than the more distal regions. This also prevents repeated skiving at the MD junction, which can weaken the cortex and increase the risk of fracture.
While PETS is a common and relatively low-risk technique for epiphysiodesis in the pediatric population, this case highlights a previously unreported complication of peri-implant fracture. It is well known that these screws need to be appropriately positioned in the physis to avoid angulation deformity or inadequate growth arrest; however, this case shows that it is also essential to ensure appropriate positioning at the cortical entry point to avoid the creation of a stress riser, which in turn puts the patient at risk for complication.
Additional Links
- JPOSNA® May 2023, Commentary on Peri-Implant Fracture After Distal Femur Percutaneous Epiphysiodesis Using Transphyseal Screws
- American Academy of Orthopaedic Surgeons (AAOS) Orthopaedic Video Theatre, Distal Femur Guided Growth: Modified Surgical Technique with Retrograde Guide Pin and Antegrade Screw
- POSNA Study Guide, Epiphyseodesis Prediction and Technique
Disclaimer
No funding was received. The authors have no conflicts of interest to report related to this manuscript.
References
- Ghanem I, Karam JA, Widmann RF. Surgical epiphysiodesis indications and techniques: update. Curr Opin Pediatr. 2011;23(1):53-59.
- Vitale MA, Choe JC, Sesko AM, et al. The effect of limb length discrepancy on health-related quality of life: is the ‘2 cm rule’ appropriate? J Pediatr Orthop B. 2006;15(1):1-5.
- Phemister D. Operative arrestment of longitudinal growth of bones in the treatment of deformities. J Bone Joint Surg Am. 1933;15:1-15.
- Monier BC, Aronsson DD, Sun M. Percutaneous epiphysiodesis using transphyseal screws for limb-length discrepancies: high variability among growth predictor models. J Child Orthop. 2015;9(5):403-410.
- Song MH, Choi ES, Park MS, et al. Percutaneous epiphysiodesis using transphyseal screws in the management of leg length discrepancy: optimal operation timing and techniques to avoid complications. J Pediatr Orthop. 2015;35(1):89-93.
- Yoo J, Ma X, Lee J, et al. Research update on stress riser fractures. Indian J Orthop. 2020;55(3):560-570.
- Al-Aubaidi Z, Engell V, Lundgaard B. Stressfraktur efter epifysiodese i femur [Stress fracture following femoral epiphysiodesis]. Ugeskr Laeger. 2010;172(41):2847-2848.
- Cheng YH, Lee WC, Tsai YF, et al. Tension band plates have greater risks of complications in temporary epiphysiodesis. J Child Orthop. 2021;15(2):106-113.
- Dodwell ER, Garner MR, Bixby E, et al. Percutaneous epiphysiodesis using transphyseal screws: a case series demonstrating high efficacy. HSS J. 2017;13(3):255-262.
- Hak DJ, Neiman R, Hazelwood S. Biomechanical strain analysis of the proximal femur following retrograde intramedullary nailing. Curr Orthop Pract. 2010;21(4):385-389.
- Solórzano W, Ojeda C, Diaz Lantada A. Biomechanical study of proximal femur for designing stems for total hip replacement. Appl Sci. 2020;10(12):4208.
- Hart NH, Nimphius S, Rantalainen T, et al. Mechanical basis of bone strength: influence of bone material, bone structure and muscle action. J Musculoskelet Neuronal Interact. 2017;17(3):114-139.
- Zhou S, Jung S, Hwang J. Mechanical analysis of femoral stress-riser fractures. Clin Biomech (Bristol, Avon). 2019;63:10-15.
- Barber CC, Burnham M, Ojameruaye O, et al. A systematic review of the use of titanium versus stainless steel implants for fracture fixation. OTA Int. 2021;4(3):e138.