
Original Research
An Effective and Safe Surgical Technique for Salvage of Postoperative Proximal Junctional Failure in Pediatric Patients–A Case Series
1KU School of Medicine, Kansas City, KS; 2Department of Orthopaedic Surgery and Musculoskeletal Sciences, Children’s Mercy Hospital, Kansas City, MO
Correspondence: Mason A. Fawcett, BA, 610 West 58th Terrace, Kansas City, MO 64113. E-mail: [email protected]
Received: August 16, 2022; Accepted: May 9, 2023; Published: August 1, 2023
Volume 5, Number 3, August 2023
Abstract
Background: Proximal junctional failure (PJF) is a known complication following posterior spinal instrumentation surgery and can be defined simply as proximal junctional kyphosis that requires surgical revision of the proximal instrumentation. PJF can be associated with pain, decreased neurologic function, infection, and increased morbidity. There is little literature on this topic in children and especially on specific surgical techniques for revision surgery.
Methods: The revision technique involves extending the spine instrumentation proximally with paired sets of sublaminar bands used as anchors. Posterior osteotomies are typically required at the level of the kyphosis. The bands are gradually and sequentially tightened, bringing the spine into a corrected sagittal position. Patients who underwent this procedure and had at least 1 year of follow-up were identified. Demographic and clinical data, as well as plain radiographic and CT sagittal spine parameters, were analyzed before the surgery and at the most recent follow-up.
Results: Eight children, average age 14 years, 10 months, were included in the study with an average follow-up time of 31 months. Revision surgery occurred approximately 3 years following the initial surgery. There was 20 degrees (ranging from an increase of 18 degrees to a decrease of 46 degrees) mean kyphotic angle correction at the site of the failure and 16 degrees (ranging from an increase of 24 degrees to a decrease of 78 degrees) mean cervical lordosis correction, using an average of six sublaminar bands. Before revision, all patients reported neck/upper back pain, with upper rod prominence. At the most recent post-revision visit, pain was markedly reduced, and rod prominence had resolved. One patient reported increased satisfaction with appearance, and another noted that maintaining horizontal gaze was easier.
Conclusion: Children who received this surgical technique for PJF experienced resolution of pain and upper rod prominence and improved cervical spine sagittal radiographic parameters that were maintained at least 1 year after revision surgery.
Levels of Evidence: IV
Key Concepts
- PJF is a known complication following posterior spine instrumentation surgery.
- PJF is associated with numerous comorbidities.
- Scarce literature currently exists on how to revise PJF once it occurs.
- Proximal extension of spine instrumentation using paired sublaminar bands was an effective and safe surgical technique to revise PJF for eight children in this study.
Introduction
Proximal junctional kyphosis (PJK) and proximal junctional failure (PJF), also described as “topping off syndrome” or “proximal junctional fracture,” are complications that can occur following posterior spinal fusion surgery.1 PJK and PJF are often thought of as two conditions on the same spectrum, with PJF being the more severe version of PJK, frequently resulting in revision surgery.2 Substantial information exists on these complications in adult populations, yet much less information is available for pediatric patients. Authors often disagree on the definitions of PJF and PJK. PJK is most often defined as a proximal junctional Cobb angle of ≥10 degrees that is at least 10 degrees greater than the preoperative proximal junctional Cobb angle, although other definitions exist in the literature.3 As with PJK, definitions of PJF also vary in the literature, with some authors claiming that PJF is present if there has been structural failure of a vertebral body and/or the posterior ligament complex.2,3 Similar to other authors, we chose to define PJF as PJK severe enough for surgical revision of the proximal instrumentation of the spine to be indicated.4,5
PJF is associated with many comorbidities, including pain, decreased neurologic function, infection, and physical deformity.2 Surprisingly, very little literature exists on management of PJF, especially in children, and surgical techniques for revision have yet to be studied. The purpose of this case series is to introduce a safe and effective surgical technique for load-sharing correction of both the posterior tension band and the anterior column support for symptomatic PJF for pediatric spinal deformity patients.
Materials and Methods
Study Design
This case series review was performed at a single institution after receiving institutional review board approval. A REDCap surgical database was used to identify pediatric patients who had undergone revision surgery performed by a single surgeon for their PJF. Patients were included in the study only if they had received this surgical technique for revision of their PJF. Their medical records were reviewed for demographic information and for the presence and severity of signs and symptoms of PJF both before and after revision surgery. Several spine parameters were measured using radiographic and CT imaging taken before revision surgery as well as at the most recent follow-up after surgery. All spine radiographic measurements were made in accordance with the Radiographic Measurement Manual produced by the Spinal Deformity Study Group.6 These pre- and post-revision parameters were then compared to determine the amount of change for each patient. Surgical documentation was analyzed for each patient to gather key information regarding the specifics of the surgical technique.
Surgical Technique
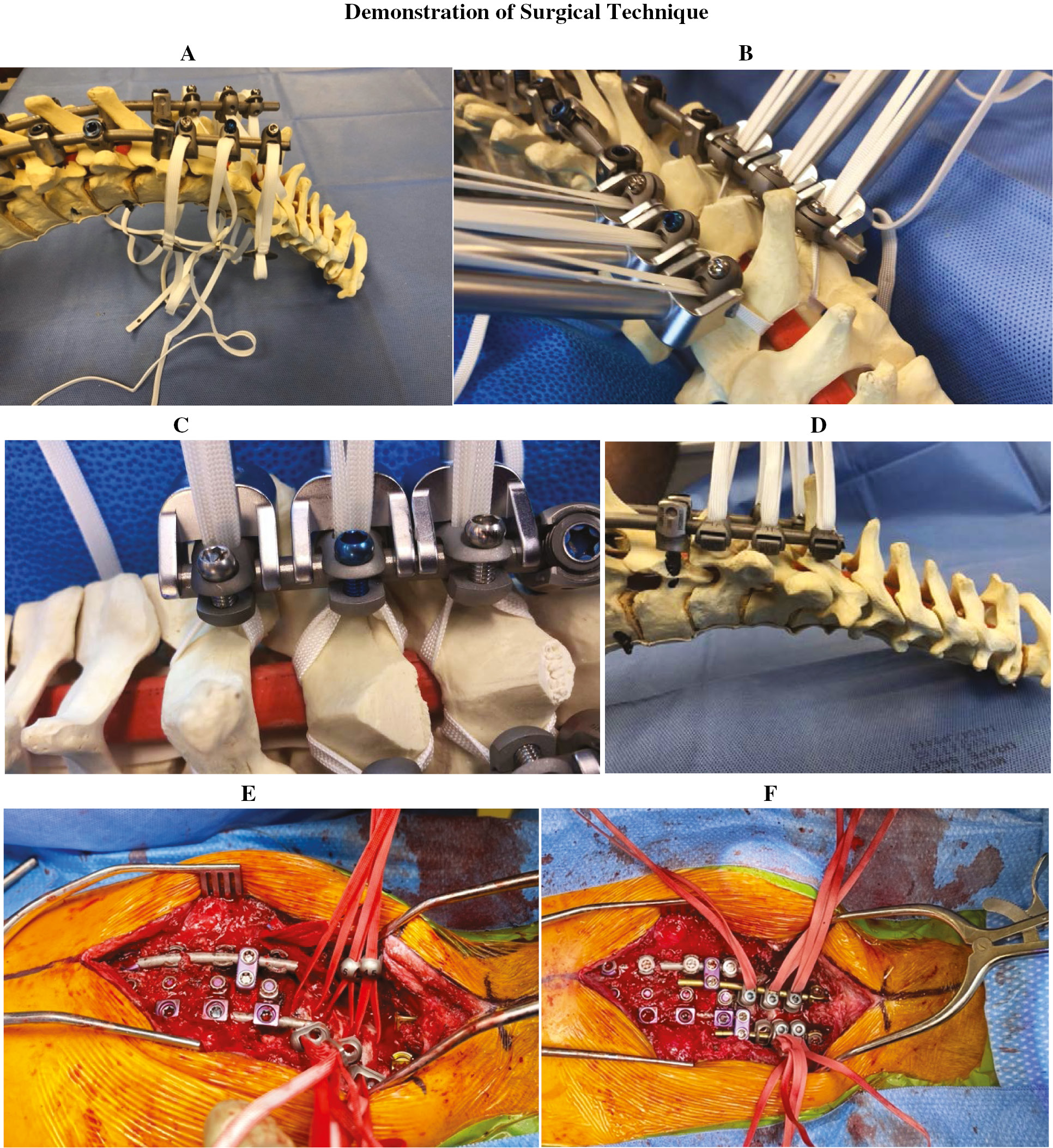
While the specifics of the surgical technique varied for each patient, the general principles remained the same. All patients were positioned prone on a 4-post spine table with Gardner-Wells tongs providing 10-15 lbs of traction at a 45-degree angle to offload the face, while providing some longitudinal traction. Soft tissue dissection was performed, and the spine was exposed to provide adequate visualization of the suspected pathology, and implants were assessed for stability and were removed as needed. Smith-Peterson or Ponte osteotomies were performed in areas of fixed bony deformity. The ligamentum flavum and facets were resected in kyphotic regions of the spine that were mobile. Several levels of paired sublaminar bands (Zimmer Biomet Company, Warsaw, IN) were then passed proximal to the point of kyphotic failure, typically to the sagitally neutral segment. New rods of the same diameter were measured and appropriately contoured, and once the rods were anchored to distal pedicle screws, the sublaminar bands were then attached to the rods. The bands were then sequentially tightened, slowly bringing the spine to the rods into a corrected sagittal position. Operative images of the procedure are shown in Figure 1. A link to the POSNAcademy video demonstrating this technique can be found under the “Additional Links” section.
Figure 1. A demonstration of PJF deformity before and after sublaminar band tightening using a spine model (A-D). Image A demonstrates what PJF may look like before band tightening. Images B and C show band positioning and the process of tightening. Image D shows PJF angle correction following band tightening. Intraoperative images showing sublaminar bands before and after tightening are shown in E and F.
Results
Six male and two female patients received this surgical technique for revision of their PJF. The mean age of the patients at the time of their initial posterior fusion was 14 years, 10 months, and revision surgery occurred at a mean of 33 months later. Follow-up occurred at a mean of 31 months after the revision surgery. Patient demographics are shown in Table 1.
Table 1. Patient Demographics
| Patient | Sex | Scoliosis Type | Age at Initial Surgery | Time Between Initial and Revision Surgery | Length of Follow-Up | Previous UIV | UIV After Salvage |
|---|---|---|---|---|---|---|---|
| 1 | M | Double major atypical adolescent idiopathic scoliosis | 16 years, 9 months | 22 months | 21 months | T3 | T1 |
| 2 | M | Neuromuscular kyphoscoliosis | 13 years, 11 months | 3 months | 60 months | T3 | C7 |
| 3 | F | Juvenile idiopathic scoliosis | 11 years, 6 months | 66 months | 33 months | T4 | T1 |
| 4 | M | Neuromuscular scoliosis | 15 years, 7 months | 19 months | 30 months | T3 | C6 |
| 5 | F | Adolescent idiopathic scoliosis | 11 years, 2 months | 19 months | 12 months | T3 | T1 |
| 6 | M | Kyphoscoliosis | 14 years, 5 months | 31 months | 14 months | T3 | C6 |
| 7 | M | Neuromuscular kyphoscoliosis | 19 years, 2 months | 32 months | 51 months | T1 | C5 |
| 8 | M | Scheuermann thoracic kyphosis | 16 years | 69 months | 24 months | T2 | T1 |
| Mean | ; | 14 years, 10 months | 33 months | 31 months |
Demographics of patients included in the study. Follow-up time was the total time between revision surgery and the most recent documented clinical encounter. UIV = upper instrumented vertebrae.
A mean of six (range 4-8) sublaminar bands (three vertebral levels proximally) were used during surgical revision. There was 20 degrees (ranging from an increase of 18 degrees to a decrease of 46 degrees) mean kyphotic angle reduction at the site of the failure, 16 degrees (ranging from an increase of 24 degrees to a decrease of 78 degrees) mean cervical lordosis reduction, and 19 degrees (ranging from an increase of 22 degrees to a decrease of 11 degrees) C2 slope increase. There was no change in intraoperative neurophysiological monitoring, no transfusion requirement, and no postoperative infections or neurological events. A summary of the changes in spine parameters for each patient is shown in Table 2.
Table 2. Changes in Spine and Pelvic Parameters
| Patient | T1-T12 Kyphosis | PJF Angle | Lumbar Lordosis | Cervical Lordosis | C2 SVA | C2 Slope | Pelvic Incidence | Pelvic Tilt | Sacral Slope | Proximal Extension | Bands Used |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 19° | 18° | 2° | 24° | 0.4 cm | −3° | −4° | −7° | 1° | 2 vertebrae | 7 bands |
| 2 | −43° | −36° | −3° | −16° | 4.1 cm | 0° | −4° | −17° | 11° | 3 vertebrae | 8 bands |
| 3 | 1° | −10° | 14° | −7° | −1.4 cm | −11° | −1° | 15° | −11° | 3 vertebrae | 6 bands |
| 4 | −35° | −46° | −17° | −78° | 2.6 cm | 19° | −1° | 30° | 19° | 4 vertebrae | 6 bands |
| 5 | 5° | 1° | −1° | 8° | 0.7 cm | −1° | 0° | −3° | 5° | 2 vertebrae | 4 bands |
| 6 | −2° | −39° | −17° | −1° | 2.2 cm | −10° | −5° | −7° | 0° | 4 vertebrae | 4 bands |
| 7 | 27° | −22° | −27° | −52° | 3.8 cm | 22° | 13° | 35° | −22° | 3 vertebrae | 6 bands |
| 8 | −2° | −27° | 16° | −6° | 0.7 cm | 3° | −3° | 4° | −2° | 1 vertebrae | 4 bands |
| Mean | −4° | −20° | −4° | −16° | 1.6 cm | 19° | −5° | 6° | 1° | 3 vertebrae | 6 bands |
Data table depicting the change in spinal parameters after revision as compared to before revision. Negative values indicate that the parameter was reduced as compared to the pre-revision value, and positive values indicate that the parameter was increased.
The proximal extension and changes in sagittal spine alignment are evident when pre- and post-revision lateral radiographs are compared (Table 3).
Table 3. Radiographic Images Pre- and Post-Revision
| Patient 1 | Patient 2 | Patient 3 | |||
|---|---|---|---|---|---|
| Pre-Revision | Post-Revision | Pre-Revision | Post-Revision | Pre-Revision | Post-Revision |
 |
 |
 |
 |
 |
 |
| Patient 4 | Patient 5 | Patient 6 | |||
| Pre-Revision | Post-Revision | Pre-Revision | Post-Revision | Pre-Revision | Post-Revision |
 |
 |
 |
 |
 |
 |
| Patient 7 | Patient 8 | ||||
| Pre-Revision | Post-Revision | Pre-Revision | Post-Revision | ||
 |
 |
 |
 |
||
Radiographic images demonstrating changes in sagittal spine alignment in each of the 8 patients.
At the most recent follow-up visit, rod prominence and pain were reduced for all patients. Rod prominence and pain levels were gathered from detailed clinical notes taken from visits before surgery and at the most recent follow-up. These reports were compared to the original clinical notes prior to revision surgery at the time when the patients had symptomatic PJF. Patient 7 reported improvement with horizontal gaze, and patient 3 reported increased satisfaction with physical appearance.
Discussion
This study describes clinical and radiographic outcomes for eight patients receiving a unique PJF revision surgery. While superiority or inferiority cannot be determined from such a small case series, this study demonstrates that patients who received this surgery experienced improvement both clinically and radiographically. On average, patients experienced a reduction in PJF angle of 20 degrees, a reduction in cervical lordosis of 16 degrees, and an increase in C2 slope of 19 degrees.
Not all patients experienced the same degrees of correction in PJF angle, cervical lordosis and C2 slope, and there are several possible explanations for these varied results. One explanation could be due to differences in patient posture during imaging as not all patients were capable of standing due to their functional status. Sagittal balance in patients who sit is different from that of patients who stand, which also impacts the degree of correction required during a revision surgery in order to restore them to their normal functional status. Not all patients had the same level of severity of PJF, and it is possible that those with more severe PJF experienced greater improvement. Spine stiffness was also not uniform among all patients due to differences in skeletal maturity and time since initial surgery. Finally, several different scoliosis subtypes were represented in this study, and it is possible that differences in disease pathophysiology could explain why some patients experienced greater correction than others.
We do recognize that pedicle screw failure/pullout can be a consequence of PJF and that PJF/PJK itself is caused by numerous factors, such as failure to achieve an appropriate sagittal balance, improper rod contouring, and incorrect level selection. The scope of our paper is merely the treatment of PJF and not the prevention of it. We recommend the use of sublaminar bands during salvage, specifically, because salvage will typically require more proximal instrumentation of smaller, potentially damaged proximal vertebrae. Using bands in this situation allows adequate kyphotic correction utilizing the relatively strong lamina in osteopenic bone while simultaneously eliminating the need to place pedicle screws in the upper thoracic and lower cervical spine. The transverse pedicle axis at T1 is consistently 30 degrees, so there is the theoretical danger of screws pulling into the spinal canal with large posterior corrective forces, a risk that sublaminar bands avoid. We have never seen lamina fractures with this technique. An upper down-going hook may be used at the UIV, or alternatively, the midline ligaments can be preserved, and a small bur can be used to create an opening between the lamina, which is possible since these segments are separated due to the kyphosis.
PJF is a well-described complication known to occur in adults with a prevalence between 1.4% and 35%.1,4,7,8 Several different definitions of PJF exist in the literature, with some of the most used definitions shown in Table 4.
Table 4. PJF Definitions
| Author | Publication Year | Definition |
|---|---|---|
| Hart et al.9 | 2013 | A change of more than 10 degrees of kyphosis between the UIV and the vertebra two levels above the UIV (UIV +2) along with one or more of the following: fracture of the vertebral body of UIV or UIV +1, posterior osseous-ligamentous disruption, or pullout of instrumentation at the UIV |
| Hostin et al.7 | 2013 | A 15-degree postop increase in PJK, fracture of UIV or UIV +1, failure of UIV fixation, or a need for proximal extension of fusion within 6 months |
| Ha et al.10 | 2019 | A 10-degree postop increase in kyphosis between UIV and UIV +2 along with one or more: fracture of UIV or UIV +1, posterior osseous-ligamentous disruption, pullout of instrumentation at UIV |
| Hart et al.11 | 2018 | A fracture at UIV or UIV +1, junctional subluxation, and failure of UIV fixation. Junctional subluxation was defined as listhesis of UIV +1 on UIV with or without UIV and/or UIV +1 fracture |
| Yagi et al.4 | 2014 | Symptomatic PJK requiring surgery |
| Yang et al.5 | 2019 | Symptomatic PJK requiring surgery |
Differing definitions of PJF across the literature.
Similar to Yagi et al. and Yang et al., we have chosen to define PJF as any adverse event indicating a need for surgical revision of the proximal spine instrumentation.4,5 Other authors have further categorized PJF by severity and by subtypes. Hart and colleagues have created a PJF severity scale, called the Hart-ISSG PJF Severity Scale, while Ha et al. have designated four distinct types of PJF.10,11 Not all patients diagnosed with PJF will undergo revision surgery, depending on the family’s decision to have this surgery for their child. The percentage of patients with PJF who undergo revision surgery ranges in the literature from 40 to 53%.7,8,12 A review of the indications for revision surgery identified traumatic PJF, severity of PJK angle, high sagittal vertical axis, and female sex as factors surgeons listed for deciding to revise.12
Several hypotheses exist that may explain the development and progression of PJF. Severity of preoperative deformity, total amount of sagittal plane correction, combined anterior and posterior approach for spinal fusion, low bone mineral density, and fusion of lower lumbar vertebrae have all been associated with development of PJF.5,13 Hart et al. also noted that patients undergoing the greatest sagittal correction, and those with a mismatch between pelvic incidence and lumbar lordosis, were at the highest risk for developing PJF in the future.9 When PJF does occur, the mechanism of failure has been shown to fall into different categories. Nguyen et al. identified several mechanisms of structural failure that occur in PJF, including vertebral body fracture, implant pullout/breakage, or disruption of the posterior osseous-ligamentous complex.1
PJF can have severe consequences and has been associated with several negative clinical symptoms. Lau and colleagues reported PJF to be associated with pain, neurologic deficits, difficulties with mobility, issues maintaining horizontal gaze, and a negative emotional disposition.2 Furthermore, a 2013 study estimated the cost of PJF revision surgery to be $77,432, which likely has continued to increase.9 PJF has been described as a “devastating” complication that surgeons must address.4
Given the severity of the consequences of PJF, some authors have identified methods, reported for adults, to prevent the development of this complication. Lau et al. found that cement augmentation of the upper instrumented vertebrae along with the use of spinal hooks for the proximal instrumentation can reduce risk of development of PJF.2 Hyun et al. reported that preservation of soft tissue structures, such as interspinous/supraspinous ligaments along with prophylactic rib fixation and vertebral cement augmentation, reduced PJF.14 Age-appropriate alignment goals are essential to reduce the risk of PJF.8
Several different spine parameters were chosen for analysis in this patient population. Sagittal vertical alignment (SVA) and C2 slope were chosen for evaluation due to their associations with health-related quality of life.15 Pelvic parameters were chosen due to the implications that pelvic positioning can have on the cervical spine.15 Since the goal of surgery is to restore cervical sagittal alignment, it was important to gather data regarding changes in parameters such as C2-C7 lordosis and C2 slope, both of which are commonly used measures of cervical spine alignment.16
Very little literature exists regarding specific surgical techniques for managing PJF. Current advice is to extend the spine instrumentation proximally and to use osteotomies if rigid deformity is present.17,18 The surgical technique described in our report incorporates the use of sublaminar bands. The use of sublaminar bands in adolescent idiopathic scoliosis in a hybrid construct with proximal hook claws and distal pedicle screws was evaluated in a prospective case series. Sale et al. concluded that the bands with a universal clamp were effective and safe methods for coronal plane and kyphosis correction.19 In pediatric patients with a kyphotic spinal deformity, some authors advocate the use of sublaminar bands in a hybrid model that includes pedicle screws and hooks. Battista et al. reported that the use of sublaminar bands for kyphotic deformities in children resulted in lower rates of PJK.20 It is hypothesized that the large surface area of the band creates a mechanical advantage for correction. The use of bands in the hybrid construct eliminates some of the adverse events associated with pedicle screw use such as screw pullout.20 Safety of using sublaminar bands has also been studied. Neuromuscular monitoring alerts were reviewed for a total of 378 spine surgeries, and use of bands was found to be equally safe in comparison to pedicle screws and hooks.21
The greatest limitations of this study are the small patient sample and retrospective design with no control group. Conclusions about superiority of this technique to others cannot be determined due to the lack of a control group. An additional challenge of this study was ensuring the consistency with which the spine parameters were measured. Patient positioning was not always consistent for imaging, with some patients sitting and some standing and the time at which imaging was performed in relation to the initial and revision procedures was also not always consistent.
In conclusion, we describe a reliable, effective, and safe technique for salvage of PJF in children that uses posterior osteotomies when needed and proximal extension of the instrumentation using an average of three vertebral levels with six sublaminar bands, resulting in gradual load-sharing correction to restore sagittal balance.
Acknowledgements
The authors express their gratitude to the Children’s Mercy Medical Writing Center for their assistance in editing this manuscript.
Additional Links
- POSNAcademy: Posterior Spinal Instrumentation and Fusion for Treatment of Adolescent Idiopathic Scoliosis
- POSNAcademy: Ponte Osteotomies
- American Academy of Orthopaedic Surgeons (AAOS) Orthopaedic Video Theatre: The Restoration of Proper Sagittal Balance
- JPOSNA®: Proximal Extension of Instrumentation Using Sublaminar Bands for Salvage of Postoperative Proximal Junctional Failure in Pediatric Patients
Disclaimer
No funding was received. The authors report no conflicts of interest related to this manuscript.
References
- Nguyen NL, Kong CY, Hart RA. Proximal junctional kyphosis and failure-diagnosis, prevention, and treatment. Curr Rev Musculoskelet Med. 2016;9(3):299-308.
- Lau D, Clark AJ, Scheer JK, et al. Proximal junctional kyphosis and failure after spinal deformity surgery: a systematic review of the literature as a background to classification development. Spine (Phila Pa 1976). 2014;39(25):2093-2102.
- Kim HJ, Yang JH, Chang DG, et al. Proximal junctional kyphosis in adult spinal deformity: definition, classification, risk factors, and prevention strategies. Asian Spine J. 2022;16(3):440-450.
- Yagi M, Rahm M, Gaines R, et al. Characterization and surgical outcomes of proximal junctional failure in surgically treated patients with adult spinal deformity. Spine (Phila Pa 1976). 2014;39(10):E607-E614.
- Yang J, Khalifé M, Lafage R, et al. What factors predict the risk of proximal junctional failure in the long term, demographic, surgical, or radiographic? Results from a time-dependent roc curve. Spine (Phila Pa 1976). 2019;44(11):777-784.
- O’Brien MF, Kuklo TR, Blanke KM, et al. Radiographic Measurement Manual. Medtronic Sofamor Danek USA, Inc.; 2008.
- Hostin R, McCarthy I, O’Brien M, et al. Incidence, mode, and location of acute proximal junctional failures after surgical treatment of adult spinal deformity. Spine (Phila Pa 1976). 2013;38(12):1008-1015.
- Line BG, Bess S, Lafage R, et al. Effective prevention of proximal junctional failure in adult spinal deformity surgery requires a combination of surgical implant prophylaxis and avoidance of sagittal alignment overcorrection. Spine (Phila Pa 1976). 2020;45(4):258-267.
- Hart RA, McCarthy I, Ames CP, et al. Proximal junctional kyphosis and proximal junctional failure. Neurosurg Clin N Am. 2013;24(2):213-218.
- Ha KY, Kim YH, Oh IS, et al. Clinical and radiographic features of subtypes of acute proximal junctional failures following correction surgery for degenerative sagittal imbalance. World Neurosurg. 2019;125:e304-e312.
- Hart RA, Rastegar F, Contag A, et al. Inter- and intra-rater reliability of the Hart-ISSG Proximal Junctional Failure Severity Scale. Spine (Phila Pa 1976). 2018;43(8):E461-E467.
- Hart R, McCarthy I, O’brien M, et al. Identification of decision criteria for revision surgery among patients with proximal junctional failure after surgical treatment of spinal deformity. Spine (Phila Pa 1976). 2013;38(19):E1223-E1227.
- Yagi M, Fujita N, Tsuji O, et al. Low bone-mineral density is a significant risk for proximal junctional failure after surgical correction of adult spinal deformity: a propensity score-matched analysis. Spine (Phila Pa 1976). 2018;43(7):485-491.
- Hyun SJ, Lee BH, Park JH, et al. Proximal junctional kyphosis and proximal junctional failure following adult spinal deformity surgery. Korean J Spine. 2017;14(4):126-132.
- Ling FP, Chevillotte T, Leglise A, et al. Which parameters are relevant in sagittal balance analysis of the cervical spine? A literature review. Eur Spine J. 2018;27(Suppl 1):8-15.
- Scheer JK, Tang JA, Smith JS, et al. Cervical spine alignment, sagittal deformity, and clinical implications: a review. J Neurosurg Spine. 2013;19(2):141-159.
- Lee J, Park YS. Proximal junctional kyphosis: diagnosis, pathogenesis, and treatment. Asian Spine J. 2016;10(3):593-600.
- Cerpa M, Sardar Z, Lenke L. Revision surgery in proximal junctional kyphosis. Eur Spine J. 2020;29(Suppl 1):78-85.
- Sale de Gauzy J, Jouve JL, Accadbled F, et al. Use of the universal clamp in adolescent idiopathic scoliosis for deformity correction and as an adjunct to fusion: 2-year follow-up. J Child Orthop. 2011;5(4):273-282.
- Battista C, Wild C, Kreul S, et al. Prevention of proximal junctional kyphosis & failure using sublaminar bands in a hybrid construct in pediatric kyphosis deformity. Int J Spine Surg. 2018;12(6):644-649.
- Polirsztok E, Gavaret M, Gsell T, et al. Sublaminar bands: are they safe? Eur Spine J. 2014;24(7):3594.