
JPOSNA® Special Edition
Advances in Pediatric Orthopaedic Education and Technical Training
Simulation Training in Pedicle Preparation and Screw Insertion in Pediatric Spinal Deformity
Department of Orthopaedics, Cedars-Sinai Medical Center, Los Angeles, CA
Correspondence: Kenneth David Illingworth, MD, Cedars-Sinai Spine Center, 444 S. San Vicente Blvd., Suite 901, Los Angeles, CA 90048. E-mail: [email protected]
Received: May 10, 2022; Accepted: June 5, 2022; Published: August 15, 2022
DOI: 10.55275/JPOSNA-2022-0059
Volume 4, Number S1, August 2022
Introduction
Pedicle screw segmental instrumentation has become the gold standard for spinal deformity correction for both the pediatric and adult populations. The thought of placing screws through tiny boney channels in the spinal column can be a daunting task for trainees. The goal in spine surgery instrumentation is similar to other orthopaedic subspecialities—safe passage of screws through the bone. Yet, the potential consequences of pedicle breaches and malpositioned instruments/screws are what give pedicle preparation and screw insertion an appropriately heightened sense of care and apprehension. Important anatomical structures lie around the pedicles of the spine, with the spinal cord, nerve roots, epidural veins, lungs, kidneys, and major vessels being just some of the structures that lurk outside of the spine’s osseous anatomy.
In 2007, we implemented power pedicle screw preparation and screw insertion to improve safety for both the surgeon and patient. A recent multicenter study of early adopters demonstrated the safety of this technique in 22,209 screws across six institutions.1 As we have taught this technique to fellow surgeons throughout the world, inevitably the question would always arise, “Do you let your residents do that?”. The answer was always an emphatic, YES. However, we began to explore ways in which we could improve our trainees’ education on pedicle screw insertion, both manual and power, given the complexity of the osseous anatomy in pediatric spinal deformity cases.
In 2019, we introduced an informal training session before a resident or fellow’s first time in our pediatric spine cases. The informal process involved a lumbar sawbones model (no deformity), Home Depot-style drills, drills/reamers, a various assortment of pedicle screws, and an office. We wanted the trainees to familiarize themselves with the technique and the equipment outside of the operating room. The Simulation Center for Advanced Clinical Skills at Cedars-Sinai Medical Center has allowed us to formalize this training/simulation program in a realistic operating room environment. This program was implemented in November 2021.
Simulation
Simulation models were created (SurgiSTUD™, Tempe, AZ). The patient model was selected for the severe nature of the curve (>100 degrees) and the significant amount of axial rotational change from the lumbar spine through the thoracic spine. This demonstrated extremes of pedicle trajectory changes throughout the spine. Two models were created: A static/interactive model with ideal pedicle trajectories from T1-S1 and a dynamic model with a soft tissue envelope (Figure 1).
Figure 1. Dynamic model on the left and static model on the right. Interactive red dowels represent the ideal starting point and trajectories for all pedicle screws from T1-S1.

Static Model
A solid T1-Sacrum model was segmented utilizing a thoracic/lumbar/sacral computed tomography scan. Prior to 3D printing, 3 mm virtual cylinders were created and virtually inserted into each of the pedicles from T1-S1. Ideal pedicle trajectories were chosen by the senior author (KDI) and were placed parallel to the endplate in the straightforward position (Figure 2). The static model was printed in one solid material with the ideal pedicle trajectory created at each level during segmentation. Plastic dowels were 3D printed for each pedicle with approximately 3 cm of dowel outside of the pedicle starting point, providing an interactive guide for both pedicle starting point and trajectory (Figure 3).
Figure 2. CT segmentation with virtual 3 mm pedicle trajectories.
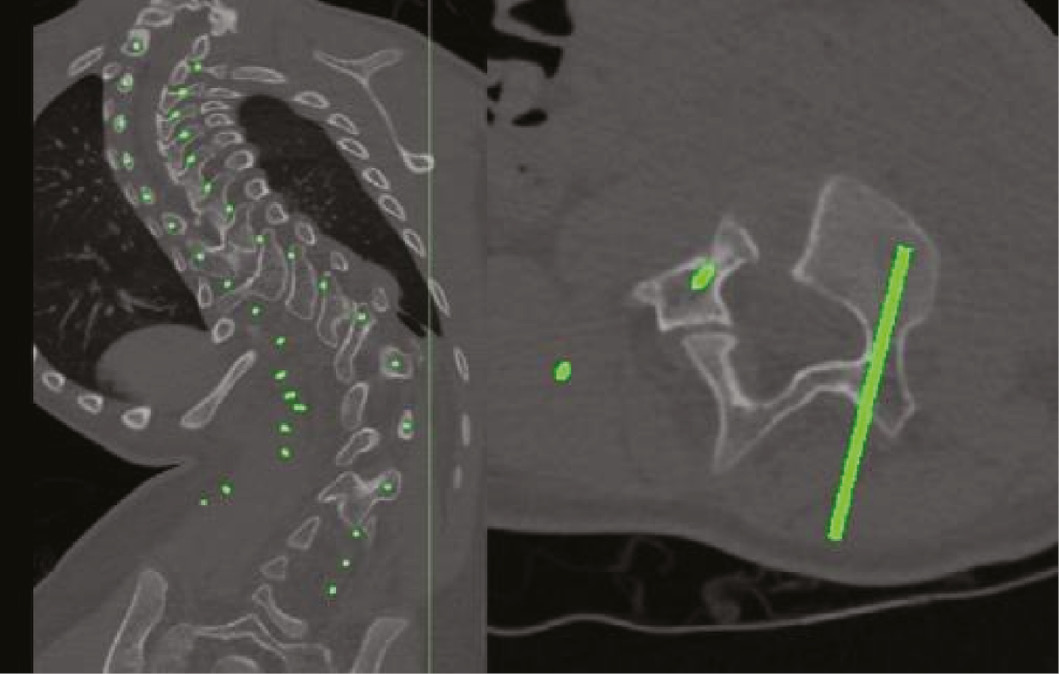
Figure 3. Static 3D printed model with interactive dowels for guidance/practice on pedicle starting points and ideal trajectories based on level.

Dynamic Model
A dynamic 3D printed model was created from the same patient scan as the static model. Benefits of the dynamic model include radiolucent soft tissue envelope, corticocancellous architecture that mimics human bone, multimaterial 3D print including intervertebral discs and supportive ligaments which provide a highly analogous and modifiable segmental range of motion, and a synthetic bone which provides high-fidelity biomechanical performance for pedicle screws and other spinal fixation devices (Figure 4).
Figure 4. Example of 3D printed model with soft tissue envelope.

Pre-Simulation
All junior-level residents (PGY1-3) who are scheduled to rotate through the pediatric spine service are required to complete the simulation training before their first pediatric spinal deformity case. All trainees are provided with the technique video and paper for “Power Pedicle Preparation and Screw Insertion in the Treatment of Pediatric Spinal Deformity.” In addition, all trainees receive the goals and objectives as outlined below:
Goals/Objectives:
- Understand the basic posterior anatomy in the spine
- Be able to identify the following:
- Spinous process, Lamina, Pars Interarticularis, Facet joint including superior and inferior articular process, Transverse process, Costovertebral joint
- Be able to identify the following:
- Identify the main instruments used in both power and manual screw pedicle screw insertion techniques
- Manual
- Curved/straight probe, Tap, Ball Tipped Pedicle probe, Tonsil
- Power
- 2 mm drill bit, 3.2 mm calibrated dull tipped reamer, Stab and grab driver
- Manual
- Perform both thoracic and lumbar level facetectomies
- Identify both thoracic and lumbar pedicle starting points based on level
- Perform both manual and power pedicle screw preparation
- Discuss common pitfalls and complications and ways to manage them
- Pedicle breaches, small pedicle channels, salvage techniques
Simulation
All simulations are performed in the Women’s Guild Simulation Center for Advanced Clinical Skills at Cedars-Sinai Medical Center. The simulation center contains two operating rooms that mimic the actual operating rooms in the hospital. The rooms are set up to simulate the operating room environment/experience, which includes full draping of the model, a scrub technician table with a full complement of posterior spinal instrumentation, and a mayo stand with essential tools for pedicle preparation and screw insertion (Figure 5).
Figure 5. Simulated operating room environment at the Women’s Guild Simulation Center for Advanced Clinical Skills at Cedars-Sinai Medical Center.

Goals/Objectives including identification of all pertinent posterior element osseous anatomy and essential surgical instruments are tested/performed as stated above.
A combination of osteotomes and wide Rongeur was used to perform lumbar and thoracic level facetectomies. A 3-mm high-speed burr was used to create a starting hole for pedicle preparation with varying locations based on region and level in the spine (Figure 6).
Figure 6. From JPOSNA® article Illingworth et al. Starting points for A. thoracic and B. lumbar pedicle screws.

Briefly, both manual and power pedicle preparation and screw insertion are described below. Expanded details of the technique can be found in Illingworth et al.2
- Manual: The curved pedicle probe was inserted with the tip aiming laterally and inserted to 20 mm. The track is checked with a ball tipped pedicle probe to ensure no breaches. The probe is then turned tip aimed medially and inserted to the anterior vertebral body. The track is again checked with a pedicle probe and the length is confirmed. An appropriately sized/length screw is inserted with a manual screwdriver.
- Power: A 2 mm drill bit is inserted on slow revolutions until 20 mm of depth. The track is checked with a ball tipped pedicle probe to ensure no breaches. The 3.2 mm calibrated dull tip reamer is then inserted on slow revolutions until the front of the vertebral body is palpated. The track is again checked with a pedicle probe and the length is confirmed. An appropriately sized/length screw is inserted with stab and grab power insertion (Figure 7).
Figure 7. A. Facetectomies performed at right L4-L5 and burr used to create pedicle starting hole. B. 2 mm drill bit inserted to 20 mm. C. Calibrated blunt tipped reamer inserted to the front of vertebral body. D. Power screw insertion with stab and grab driver.

The model provides excellent haptic feedback during pedicle preparation and screw insertion, closely mimicking human bones. Given the foam surrounding the osseous anatomy, pedicle breaches, both medial and lateral, give a realistic sensation compared to intra-operative situations. The addition of the static/interactive model is invaluable during the simulation, as it allows the trainee to visualize the trajectory of each pedicle, at each level, in real-time. The interactive dowels allow you to analyze the starting point and trajectory and apply that to the training model (Figure 8).
Figure 8. Static/Interactive model is a valuable educational tool for learning pedicle starting points and trajectories.

Post-Simulation
The simulated operating rooms are equipped with 4-way video recording for post-simulation debriefing and review as needed. Each trainee is provided with the following questionnaire.
Post-Simulation Questionnaire:
- Rate your comfort level with posterior spine anatomy prior to the simulation (1-10)
- Did you learn anything new about the anatomy? (Y/N)
- Rate your comfort level with manual pedicle screw preparation and insertion prior to simulation (1-10)
- Rate your comfort level with power pedicle screw preparation and insertion prior to simulation (1-10)
- Rate your comfort level with manual pedicle screw preparation and insertion post simulation (1-10)
- Rate your comfort level with power pedicle screw preparation and insertion post simulation (1-10)
- Did you learn anything about basic spine instrumentation that you did not know before? (Y/N)
- Did the simulation exercise improve your confidence with spine pedicle screws and instrumentation prior to your first case? (Y/N)
- After your first case implementing power pedicle techniques, rate the quality of the simulation environment to the actual OR (1-10)
Summary
The addition of the Pedicle Preparation and Screw Insertion in Pediatric Spinal Deformity simulation lab at Cedars-Sinai has been a huge benefit to the trainees. Universally, trainees have described increased confidence during their pediatric spinal deformity cases and attendings have experienced an increased level of safety. In particular, the ability to instrument a simulated model with the static/interactive model in hand provided a much greater appreciation for the impact a significant deformity has on pedicle starting point and trajectory. This cannot be gained from practicing on a model without deformity. The lab has evolved from a sawbones in an office to a fully simulated OR environment. Areas for improvement include the sustainability and cost of the simulation (see Appendix). We are working on streamlining the implant and tools needed for each lab to decrease resource utilization. Future directions include researching the impact this lab has on trainees and how these techniques influence the safety of pedicle screw insertion during pediatric spinal deformity cases.
Disclaimer
C. Johnson: No conflicts of interest to report; D. Skaggs: Research Grants: NuVasive (Co-PI, Paid to Growing Spine Foundation), Consulting: Zimmer Biomet; Grand Rounds (a healthcare 2nd opinion company); Orthobullets; Stocks options: Green Sun Medical, Stocks: Orthobullets, Board Membership: Growing Spine Study Group, Growing Spine Foundation, Paid Lecturer: Zimmer Biomet, Patents: Zimmer Biomet, Royalties: Wolters Kluwer Health; Zimmer Biomet, Editor: Orthobullets, Co-Editor in Chief, Editorial boards: Spine Deformity, Orthopedics Today, Journal of Children’s Orthopedics; K. Illingworth: Consulting: OrthoPediatrics; Data Monitoring and Safety Board: Medtronic.
References
- Skaggs DL, Compton E, Vitale MG, et al. Power versus manual pedicle tract preparation: a multi-center study of early adopters. Spine Deform. 2021;9(5):1395-1402.
- Illingworth KD, Andras LM, Claeson AA, et al. Power Pedicle Preparation and Screw Insertion in the Treatment of Pediatric Spinal Deformity: JPOSNA® [Internet]. 2019 Nov 3 [cited 2022 Mar 29];1(1). Available at: https://www.jposna.org/ojs/index.php/jposna/article/view/13.
Appendix
Supplies Cost:
- Static Model with Interactive Dowels: $1,125.00
- Dynamic Model: $1,365.00*
- Spine Instrumentation: Borrowed free of charge
- Spine Implants: Donated
- Simulation Center: Available to academic faculty at our institution free of charge
*At our institution, we are working on developing our own 3D printing protocols to allow for a more financially sustainable program going forward.