
Surgical/Technical Tips
“A Little Skin in the Game”: Full Thickness Skin Grafting in Pediatric Orthopaedic Surgery
1Division of Plastic and Reconstructive Surgery, University of Wisconsin School of Medicine and Public Health, Madison, WI; 2Department of Orthopedic Surgery, University of Wisconsin School of Medicine and Public Health, Madison, WI
Correspondence: Michael L. Bentz, MD, University of Wisconsin Health University Hospital, 600 Highland Ave., G5/361, Clinical Science Center, Madison, WI 53792. E-mail: [email protected]
Received: June 12, 2023; Accepted: July 7, 2023; Published: August 1, 2023
Volume 5, Number 3, August 2023
Abstract
Congenital orthopaedic anomalies and acquired pediatric wounds of the extremities frequently require reconstruction of the soft tissue envelope. In many of these circumstances, full-thickness skin grafting (FTSG) is a reliable and appropriate reconstructive option. However, FTSG harvest is rarely discussed in the orthopaedic literature. We present a reliable and reproducible method of full-thickness skin grafting that is easily performed. In this technique, we harvest a full-thickness skin graft from the lower abdomen using a symmetric transverse midline suprapubic incision (i.e., Pfannenstiel incision). This donor site allows for abundant skin graft harvest while providing a concealed location and the potential for additional graft harvest. Finally, we discuss the critical importance of postoperative recipient site dressings to optimize skin graft take.
Key Concepts
- Full-thickness skin grafts (FTSG) represent a straightforward and reliable strategy for pediatric orthopaedic reconstruction in the appropriate patient.
- Skin grafts rely on a healthy recipient wound bed to heal in three distinct phases—plasmatic imbibition, inosculation, and revascularization.
- FTSG result in less secondary long-term contracture than split-thickness skin grafts (STSG), which is crucial for the growing extremity and why they are preferred for use over joints and areas of motion.
- FTSG can be harvested from a symmetrically designed low transverse suprapubic midline incision to facilitate primary and repeat skin graft harvest and minimize ambiguity regarding prior abdominal surgery.
- The most common causes of skin graft failure include shear forces, fluid collections, and infection, making the recipient site surgical dressing of paramount importance.
Introduction
Reconstruction of congenital anomalies and acquired wounds of the pediatric extremities require attention to a plan for soft tissue reconstruction.1 In particular, syndactyly is the most common congenital hand malformation resulting from a failure of web space apoptosis during embryological development.2 Successful treatment of syndactyly relies on creating a pliable webspace to optimize the function and appearance of each finger.2 The pathologic webspace in syndactyly has a circumference 22% less than the two separated digits, resulting in a skin deficit commonly requiring full-thickness skin grafting after successful digital separation.2 In addition to syndactyly, congenital talipes equinovarus, congenital vertical talus, and constriction/amniotic bands are other common orthopaedic pathologies that create a soft tissue deficit after reconstruction is completed.3,4 Thus, soft tissue defects are a routinely encountered problem that require the orthopaedic or plastic surgeon to feel comfortable with various soft tissue reconstructive options. The purpose of this manuscript is to discuss the principles of skin grafting, utility of full-thickness skin grafting, and to provide a technical guide for full-thickness skin grafting.
Background
The skin is a layered structure that acts as a critical barrier from the external environment. The epidermis is the outermost layer of skin, consisting primarily of keratinocytes.5 The dermis consists of collagen, elastin fibers, and the deeper portion of epithelial appendages.5 Split-thickness skin grafts (STSG) are grafts involving the epidermis and varying levels of the dermis. In contrast, full-thickness skin grafts (FTSG) include the epidermis and the entirety of the dermis.6 Ultimately, the decision to utilize a STSG or FTSG depends on various wound and donor/recipient site factors.
Primary and secondary contraction of a skin graft is an important consideration when selecting a graft thickness, particularly for coverage of the growing extremity where maintenance of motion is paramount. Primary contraction is an elastin fiber mediated phenomenon that results in immediate graft contraction after harvest. Secondary contraction, which occurs over time as the graft heals, is a myofibroblast-mediated phenomenon that can result in significant limitations in the mobility of a healed graft due to fibrosis. Secondary contraction with thinner dermal components can cause a joint contraction depending on the placement. Due to the increased concentration of elastin in FTSG and the increased concentration of myofibroblasts in STSG, we can reliably predict that FTSG will undergo higher rates of immediate primary contraction while STSG will undergo higher rates of longer-term secondary contraction.6 Thus, contraction highlights the importance of FTSG use over joint spaces to maximize mobility, such as in patients with congenital syndactyly.
Another important consideration is the impact of donor site morbidity in relation to the graft size needed. The donor site of an FTSG allows for primary closure, limiting the size of the graft harvest. The donor site for an STSG will heal by secondary intention as deeper dermal structures, including the stratum basale, remain intact. Another consideration in choosing between FTSG and STSG is the setting where surgery is being performed. Not infrequently, surgeons may be required to provide coverage in patients from developing regions with more severe deformities and where there is no ready access to dermatomes and meshers used for STSG. In these instances, FTSGs can be chosen, provided the recipient defect meets the criteria.
Understanding the mechanisms for skin graft healing is crucial to appropriately managing skin grafts in the postoperative period. Skin grafts rely on a healthy wound bed to heal and result in maximal graft take. This process is split into three phases: plasmatic imbibition, inosculation, and revascularization. Imbibition, which takes place during the first 24 hours, is a passive process that relies on a healthy wound bed to establish adherence and growth through nutrients contained within the serum and plasma. Inosculation and revascularization occur over the next 48-96 hours and consists of growth of microvasculature into the graft from the wound bed.6 This is the impetus for surgeons to employ bolster-type dressings as they prevent shearing of the graft and minimize fluid buildup during this initial healing process. Additionally, many surgeons choose to immobilize patients to prevent shearing of the graft from the wound bed. Lastly, one must understand that due to the mechanisms of skin graft healing, thicker STSGs and particularly FTSGs, have a greater cross-sectional thickness and are associated with higher metabolic demands from the wound bed. The healing process highlights the importance of postoperative activity and wound care protocols to prevent shear and fluid accumulation.
Maximizing full-thickness skin graft healing requires thorough analysis of the recipient site. While a full-thickness skin graft can be placed anywhere on the body, they are more commonly used in areas where there are concerns for motion, as full-thickness skin grafts do not undergo as significant secondary contraction over time. Full-thickness skin grafts are also noted to have more aesthetic appeal than a split-thickness skin graft, which makes this a more appealing option for visible wounds. Full-thickness skin grafts rely on a vascularized wound bed to allow healing to occur. They cannot be placed on avascular wounds or structures. This includes bone without periosteum and tendon without paratenon.
Methods
- Mark the donor site as a symmetric transverse suprapubic incision at the abdominal fascial insertion line (Figure 1). The lower incision is marked as a gently curved transverse incision, and the upper incision is marked in an elliptical fashion to ensure tensionless closure. Subcutaneous injection of dilute epinephrine and marcaine will minimize blood loss and augment pain control.
- The maximum width of the graft should be measured so that primary closure of the donor site can be achieved.
- Locating this incision in the lower abdomen will allow for repeat skin graft harvesting if needed.
- The use of an incision designed about the midline minimizes the chance that it will be mistaken for an appendectomy incision should the graft have been harvested from the right lower quadrant groin crease.
- Incise the graft with a 15-blade making a full-thickness incision through the epidermis and dermis. Raise the entirety of the graft off the subcutaneous fat using a 15 blade. Obtain meticulous hemostasis with electrocautery.
- Thin the graft on the back table to a level just superficial to the hair follicles (Figure 2).
- Thinning the graft using tenotomy scissors to remove all the fat and hair follicles will decrease the metabolic demands needed for wound healing, improve graft take by inosculation, and limit late hair growth.
- Close the donor site primarily using interrupted inverted 5-0 PDS in a deep dermal layer and 5-0 monocryl in a running subcuticular fashion. Place steri-strips over mastisol and an occlusive tegaderm patch as dressings.
- Tailor the skin graft to cover any defect and sparingly use 5-0 vicryl simple interrupted for key inset stitches, followed predominantly by 5-0 chromic simple interrupted sutures for the remainder of the graft.
- Suture from “ship to shore” (i.e., the skin graft to the native skin) to allow for more graft stability during closure.
- By using a 15 blade, one can create a few small puncture wounds through the graft to allow fluid to egress from underneath the graft. We have infrequently found this to be necessary in a completely hemostatic wound.
- Save the entirety of the harvested and trimmed graft until the end of the procedure to ensure no additional graft is needed.
- Place bolster dressings over the graft, whether in the form of a well-padded splint/cast or Xeroform (Figure 3). A bolster dressing is crucial to prevent shear and fluid accumulation underneath the graft, which would prevent inosculation.
- The well-padded splint and dressings will stay on for 1.5-2 weeks to allow for adequate revascularization of the graft while also balancing immobilization of the extremity. This dressing allows for both prevention of fluid accumulation and minimizes shearing forces that are normally produced through joint motion. Tie-over bolsters can be used, if necessary, but commonly well-placed cotton gauze wraps suffice and avoid the challenge of removing the bolster in a child.
Figure 1. Intraoperative photograph of skin graft markings. Vertically oriented line is determined according to the patient’s midline.

Figure 2. Full-thickness skin graft following thinning. Note the absence of subcutaneous fat from the graft and relatively uniform appearance of dermis.

Figure 3. Well-padded splint applied to entire upper extremity to allow for maximal skin graft take.

To further illustrate the utility of FTSG, we present a case involving a 13-year-old female patient who underwent surgical excision of a right distal femoral osteochondroma. During the surgery, a suspicious nevus was identified on the plantar surface of the second toe. To reconstruct the nevus excision site, the decision was made to utilize an FTSG harvested from the thigh. The nevus before and after excision is demonstrated in Figure 4 and Figure 5, respectively.
Figure 4. Suspicious appearing nevus along the plantar surface of the second toe.

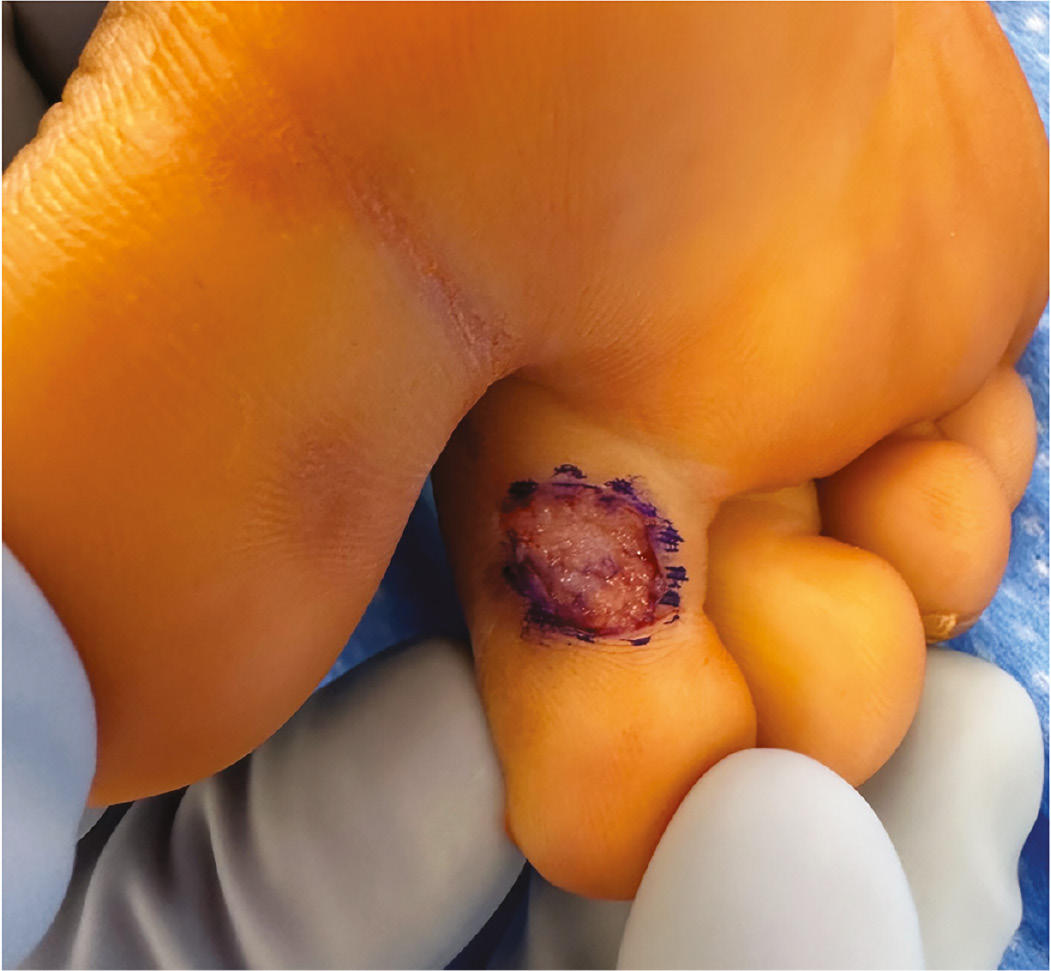
Figure 5. Resulting defect following nevus excision.
A full-thickness skin graft was harvested from the medial thigh, the donor site was closed primarily, and the graft prepared as described above (Figure 6).
Figure 6. Skin graft donor site along medial thigh.

The skin graft was trephined to facilitate fluid drainage and secured to the recipient site. To ensure appropriate compression and minimize shearing forces, a Xeroform bolster was utilized to secure the skin graft (Figure 7).
Figure 7. Xeroform bolster secured with interrupted Nylon sutures.

A 2-week postoperative follow-up revealed excellent skin graft take (Figure 8).
Figure 8. Appearance of skin graft at 2 weeks (left) and at 6 weeks final follow-up (right).

Surgical solutions regarding skin deficits in various congenital orthopaedic anomalies have been proposed in the literature. Split thickness skin grafting following syndactyly repair, club foot repair, and constriction band release has been discussed as a potential solution for coverage.7 Split-thickness skin grafting has limitations at the donor and recipient sites.8 At the donor site, split-thickness skin graft harvest can lead to considerable pain and necessitates attentive wound care due to the exudative nature of this donor site. This can lead to increased dependence on pain medications and the demand for more caretaker or nursing attention. 8 Split-thickness skin grafts have higher rates of myofibroblast activity resulting in increased fibrosis and therefore secondary contracture at the recipient site which ultimately limits mobility over a joint surface.6 It is also believed that split-thickness grafts provide minimal sensation at the recipient site, given that dermal appendages are not harvested with the graft, which is an essential consideration for extremity reconstruction.8
Rotational flaps have also been described in the literature and provide a viable option for specific soft tissue reconstructions.9 Rotational flaps provide coverage using similar pliable tissue that allows for mobility at the level of the joint. In addition, there is the preservation of sensation since the flap remains in continuity with its deeper dermal appendages. Depending on the design and elevation of rotational flaps, there is a risk of flap necrosis. Since there is a steep learning curve to design and harvest rotational flaps, we recommend using full-thickness skin grafts when appropriate as a simple and reliable form of reconstruction.
Summary
In conclusion, full-thickness skin grafting provides a reliable reconstruction method for soft tissue defects in congenital orthopaedic anomalies of the extremities, particularly those that require optimal motion at the recipient site. This surgical technique can be reproduced globally with low rates of complications. Furthermore, this method allows for the possibility of secondary grafting using the same donor site. While this approach provides many advantages when used for soft tissue reconstruction, there are potential limitations, including the wound healing complication of both recipient and donor sites.
Additional Links
- POSNAcademy: Syndactyly Skin Graft
- POSNAcademy: A Case of Bilateral Acrosyndactyly from Constriction Ring Syndrome
- POSNAcademy: Posterior Medial Release for Idiopathic Clubfoot
Disclaimer
No funding was received. The authors report no conflicts of interest related to this manuscript.
References
- Taylor B, Triplet J, Wells M. Split-thickness skin grafting: a primer for orthopaedic surgeons. J Am Acad Orthop Surg. 2021;29(20):855-861.
- Kempton SJ, Michelotti BF, Salyapongse AN, et al. Syndactyly Reconstruction. Global Reconstructive Surgery. January 2019.
- Drury BT, Rayan GM. Amniotic constriction bands: secondary deformities and their treatments. Hand (N Y). 2019;14(3):346-351.
- Rockwell WB, Daane S, Zakhireh M, et al. Human skin allograft used to treat open wounds after club foot release. Ann Plast Surg. 2003;51(6):593-597.
- Yousef H, Alhajj M, Sharma S. Anatomy, Skin (Integument), Epidermis. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022.
- Grabb WC, Smith JW, Chung KC. Grabb and Smith’s Plastic Surgery. Philadelphia, PA: Wolters Kluwer; 2020.
- Clare MP, Fitzgibbons TC, McMullen ST, et al. Experience with the vacuum assisted closure negative pressure technique in the treatment of non-healing diabetic and dysvascular wounds. Foot Ankle Int. 2002;23(10):896-901.
- Braza ME, Fahrenkopf MP. Split-Thickness Skin Grafts. [Updated 2022 Jul 25]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022.
- Lubicky JP, Altiok H. Regional fasciocutaneous flap closure for clubfoot surgery. J Pediatr Orthop. 2001;21(1):50-54.