
Quality Improvement Case Series
Commentary to Quality Improvement Case Series: Peri-Implant Fracture After Distal Femur Percutaneous Epiphysiodesis Using Transphyseal Screws
1Rainbow Babies and Children’s Hospital, Cleveland, OH; 2University of North Carolina, Chapel Hill, NC; 3Scottish Rite for Children, Dallas, TX; 4Nemours Children’s Health, Wilmington, DE
Received: April 17, 2023; Accepted: April 17, 2023; Published: May 1, 2023
Volume 5, Number 2, May 2023
Case Commentary
Raymond W. Liu, MD

Percutaneous epiphysiodesis using transphyseal screws is an interesting option in the treatment of lower limb length discrepancy in immature patients. The authors describe a previously unreported complication of a postoperative fracture through a drill hole that occurred above the medial screw. I commend the authors for reporting this complication to educate other surgeons and for their thoughtful discussion. There are a few interesting points I would like to highlight regarding this case:
- The locations of the screw starting points appear a little too proximal in the femur. As growth of bone is responsive to load in accordance with Wolff’s law, I find the thickness of the cortex to be more useful than any anatomical landmarks in determining where a screw should be placed. In the proximal femur, I try to avoid placing a screw in any region where the cortical thickness is 50% or more of the cortical thickness of the diaphysis. This typically corresponds to the level of the inferior aspect of the lesser trochanter but varies from femur to femur. In the distal femur, it is possible to place screws more in the metaphyseal region where the thickness of the cortex has essentially fully tapered off (Figure 1). At this level, such a screw should still be able to cross the physis at the desired positions on both sides. As an added benefit, when placing screws at this more metaphyseal level, the flare of the bone makes its surface more orthogonal to the path of the wire, potentially resulting in fewer errant passes.
- The limb length discrepancy was 3.3 cm. At a skeletal age of 14 years in a male, one would expect closing the distal femur to under-correct. This is a very reasonable approach, as bringing the difference under 2 cm would minimize risks of developing symptoms in the future while also maintaining some shortness can be helpful for the future. If the patient proceeds to total hip arthroplasty, that procedure would lengthen the right lower extremity.
- Both Figures 1 and 5 in the manuscript are un-lifted images. When possible, it is preferable to obtain full-length images with a lift under the short leg to balance the pelvis. This helps avoid limb positioning issues such as hip abduction/adduction, knee flexion, and ankle equinus that the child may habitually employ and which can distort the true discrepancy.
- The use of the retrograde nail by the outside institution is very interesting. An ovine study demonstrated that placement of a retrograde femoral nail up to 7% of the cross-sectional area of the physis does not inhibit growth at the distal femoral physis.1 Anatomical data suggests that cross sectional violation should be well below this amount in most clinical scenarios. Accordingly, a clinical study of 29 children in Mongolia with mean age 11 years treated with retrograde femoral nailing for femoral shaft fracture did not detect any growth arrest or obvious inhibition.2
In this case, it is unclear whether the physis continues to grow. With the metaphyseal interlocks, if the physis is growing, then the position of the distal tip of the nail versus the physis should change with time. If this occurs, the nail can become quite buried within the femur, as illustrated in Figure 2. In the authors’ case, it is possible that the combination of the previous transphyseal screws and the subsequent nail placement was enough to cause cessation of growth. If the outside hospital had wanted to increase the probability of enacting epiphysiodesis, they could have placed an epiphyseal interlocking screw in the most distal hole of the nail.
Finally, the nail has an anterior starting point, while a more central starting point would be preferable. The child should be followed until physeal closure for the potential development of recurvatum deformity, with serial examination of maximal knee hyperextension and measurement of anatomical posterior distal femoral angle.
Figure 1. Example of PETS with screw placement in the metaphyseal region of the distal femur.

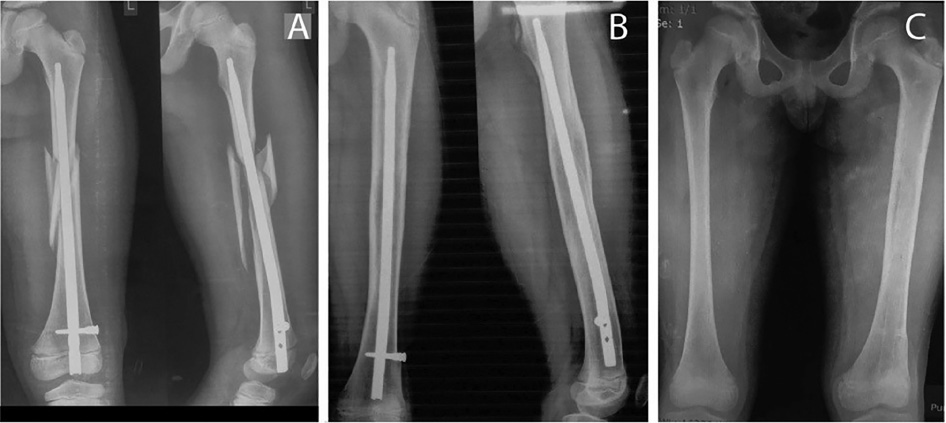
Figure 2. This 8-year-old male sustained a comminuted left femoral shaft fracture. Given the local limitations of his hospital, including lack of intraoperative fluoroscopy and limited implant options, his surgeon utilized retrograde rigid femoral nailing. (A) Immediate postoperative radiographs show acceptable positioning of the nail. (B) Images at 18 months postoperative demonstrate the expected growth of the distal femur, bringing the physis inferior to the proximal tip of the nail. There is no evidence of growth arrest. (C) The nail was removed, and a postoperative bilateral femur AP radiograph suggests equal limb lengths. Case courtesy of Batzorig Bazar, MD.
Case Commentary
James O. Sanders, MD

PETS is a very successful technique for both angular and limb length correction in growing children. Because the technique uses screws, it is susceptible to the same mechanical problems of any orthopaedic implant system, including prominence, fatigue, bending, and stress riser fracture.
Stress risers or stress concentrations occur when a material has an abrupt change in geometry or properties. Any abrupt change in stress distributions across load-bearing structures, such as bone, can exceed the ultimate strength of the structure. While failure can occur anywhere, it is most common in high-stress-bearing areas, particularly holes in cortical, weight-bearing bone.3
The distal femur has several potential trajectories for percutaneous transepiphyseal screws. One, shown by the authors, has lateral and medial cortical start points which must cross to enter the epiphysis. The authors also comment on an antegrade approach to remain in more metaphyseal bone, which is less prone to stress concentrations. My preference is another path that starts in the anterior distal femoral metaphysis and is directed distally and posteriorly (Figure 3). This metaphyseal bone is not as dependent on cortical continuity for structural integrity. While I have not experienced a stress riser fracture through this area and expect the mechanical properties minimize the risk, it will never be zero, and patients must be counseled appropriately before surgery that a risk exists.
Figure 3. Placing PETS implants in this trajectory may decrease risk of diaphyseal fracture.

Case Commentary
David Podeszwa, MD

I applaud the authors for counseling the family to undergo an epiphysiodesis. For a relatively small, asymptomatic limb length difference, there is no need to recommend lengthening. Although this patient is a candidate for a femoral lengthening with a motorized intramedullary rod, the patient will be subject to a 6-month treatment process and a different (and often more severe) set of potential complications.
PETS has become an attractive technique for many surgeons because it is “fast,” “less invasive,” and an “easy recovery” for the patient. Even the simplest procedure, performed expertly, can have a complication, and PETS is no different.4 Our enthusiasm for PETS should not cloud our memory of the Phemister technique and/or similar open curettage techniques for the treatment of LLD that have proven efficacious with a low complication rate. Makarov et al. analyzed a cohort of 863 patients undergoing epiphysiodesis, of which 822 (95.3%) underwent open curettage/Phemister technique. They identified a 2.6% rate of peri-operative complications, 4.4% rate of physis-related complications.5 No fractures were reported, and there was only a 2.1% re-operation rate. Song et al. report a re-operation rate for PETS of 83%, primarily for hardware removal.4 The added time of an open curettage may slightly prolong recovery, but it eliminates the cost of the hardware, the complications associated with the hardware, and the costs and risks of surgery for hardware removal should it be symptomatic.
Case Commentary
L. Reid Boyce Nichols, MD

Nothing ruins good results like follow-up. This saying bothers me, especially when problems arise after things look good!
In this case, this child has a bone age of 14 and limb length discrepancy of 3.3 cm. You may want the right leg to remain slightly shorter secondary to the right hip shape and history of Perthes. By the multiplier method, epiphysiodesis would be best around 13 years and 6 months. Comparing this to the arithmatic method, 2 years of growth may equalize by 1.8 cm. Although the PETS technique can have excellent results, hardware complications can happen, even requiring a second surgery to remove.
This patient is nearing skeletal maturity, which needs to be considered when using the PETS technique. Métaizeau pointed out that growth arrest via PETS shows 6 months’ latency and efficacy is progressive, peaking at 1 year. If it appears that a growth arrest might not recoup the projected discrepancy due to advanced maturity (as Dr. Podeszwa points out), maybe a permanent drill epiphysiodesis would be a good choice for the next case.
Additional Links
- JPOSNA® Vol. 5, No. 2: May 2023, Peri-Implant Fracture After Distal Femur Percutaneous Epiphysiodesis Using Transphyseal Screws
Disclaimer
The authors have no conflicts of interest to report related to this manuscript.
References
- Knapik DM, Zirkle LG, Liu RW. Consequences following distal femoral growth plate violation in an ovine model with an intramedullary implant: a pilot study. J Pediatr Orthop. 2018;38(10):e640-e645.
- Benedick A, Bazar B, Zirkle LG, et al. Retrograde intramedullary nailing of pediatric femoral shaft fractures does not result in growth arrest at the distal femoral physis-a retrospective cases series. J Orthop Trauma. 2021;35(11):e405-e410.
- Zhou S, Jung S, Hwang J. Mechanical analysis of femoral stress-riser fractures. Clin Biomech (Bristol, Avon). 2019;63:10-15. Epub 20190214.
- Song MH, Choi ES, Park MS, et al. Percutaneous epiphysiodesis using transphyseal screws in the management of leg length discrepancy: optimal operation timing and techniques to avoid complications. J Pediatr Orthop. 2015;35(1):89-93.
- Makarov MR, Dunn SH, Singer DE, et al. Complications associated with epiphysiodesis for management of leg length discrepancy. J Pediatr Orthop. 2018;38(7):370-374.