
Master’s Surgical Technique
Percutaneous Fixation of Pediatric Proximal Humerus Fractures
1Scottish Rite Hospital for Children, Dallas, TX; 2Department of Orthopaedic Surgery, University of California San Francisco, San Francisco, CA; 3Department of Orthopedics and Rehabilitation, University of Wisconsin, Madison, WI
Correspondence: Ishaan Swarup, MD, University of California, San Francisco, 747 52nd St., OPC First Floor, Oakland, CA 94609. E-mail: [email protected]
Received: March 31, 2023; Accepted: April 17, 2023; Published: May 1, 2023
Volume 5, Number 2, May 2023
Abstract
Proximal humerus fractures can be seen in children and adolescents after a fall or following significant trauma, like motor vehicle accidents. Significant remodeling potential from the proximal humeral physis along with the wide arc of motion of the shoulder allows for good outcomes with nonoperative care for minimally displaced fractures and fractures in younger children. Operative management is reserved for fractures with greater displacement and angulation, particularly in adolescents nearing skeletal maturity. Closed reduction techniques in the operating room can be difficult due to patient size, fracture displacement, interposed tissue, and deforming forces acting on the proximal humerus. Skeletal stabilization after closed reduction can include percutaneous pins, screws, and flexible nails. Here, we describe a technique for percutaneous reduction and fixation of the difficult-to-reduce proximal humerus fracture.
Key Concepts
- The proximal humeral physis has considerable remodeling potential, allowing for significant tolerance of deformity in skeletally immature children.
- Radiographic and age-based indications for reduction and fixation of proximal humerus fractures remain controversial, but multiply injured patients and significantly displaced fractures in those nearing skeletal maturity are most likely to benefit from surgical management.
- Percutaneous reduction techniques can aid in improving fracture alignment when closed maneuvers fail without the need for an extensive open approach.
- Screw fixation may provide certain advantages in comparison to pin fixation.
Introduction
Pediatric proximal humerus fractures are relatively uncommon upper extremity injuries, estimated to comprise 0.45-2% of upper extremity fractures and occur in up to 3% of the pediatric population.1 Traumatic proximal humerus fractures typically result either from a direct blow to the shoulder or less commonly, a fall on an outstretched hand. Because the proximal humeral physis is responsible for 80% of the growth of the humerus, there is substantial remodeling capacity after fractures involving the proximal humerus. Therefore, indications for acceptable alignment of proximal humerus fractures remain controversial. Numerous authors have published proposed algorithms for determining which fractures should be reduced with or without internal fixation, and age and fracture displacement are important factors in determining management.2–4
The purpose of this paper is to present strategies and techniques to be employed in the operating room when trying to reduce and stabilize proximal humerus fractures in children and adolescents.
Surgical Indications
Parameters for what constitutes “unacceptable” alignment for pediatric and adolescent proximal humerus fractures remain controversial. Generally speaking, surgical fixation is reserved for older children approaching skeletal maturity with displaced and angulated fractures. Kim et al.’s recent publication nicely summarizes the proposed treatment algorithms published over the last 30 years.5 Less controversial indications for surgical stabilization include open fractures, polytrauma requiring early weight-bearing of the affected upper extremity, and multiple ipsilateral extremity fractures (the “floating elbow”).
Treatment Challenges
There are a number of potential factors that can make successful closed reduction of these fractures difficult. The nature of the fracture itself can be challenging; in general, fractures are more easily reduced when some control can be exerted on each segment of a bone. This is not the case with the highly mobile proximal humerus, as the surgeon has no way to “grab it.” In addition, the humeral shaft is small in diameter in comparison to the proximal humerus. Oblique pin placement from distal to proximal can be challenging and made more difficult in patients with severe swelling or a high BMI. The proximity to the patient’s head and airway introduces challenges with positioning and applying force to gain reduction. Some surgeons prefer to use a beach chair position, while others position the patient supine on a radiolucent table. Strategies to safely secure the patient to the operating table are critical, as substantial traction may be needed to reduce overlap. Another common challenge is obtaining adequate imaging and being able to gain orthogonal fluoroscopic images not obstructed by the bed, the patient’s head, or the thorax. Finally, the strategic placement of image monitors is critical so the surgeon can see without difficulty.
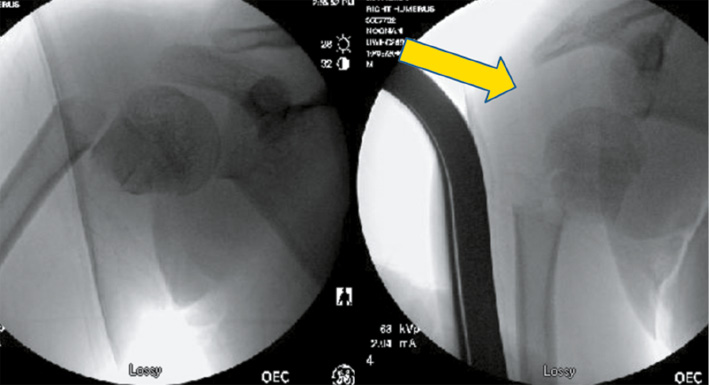
There are a number of muscles that act upon the fracture fragments and can lead to displacement. The rotator cuff musculature tends to externally rotate the proximal fragment while the deltoid exerts an abduction force. The pectoralis and latissimus tendons can adduct the shaft away from the abducted proximal fragment. The posterior periosteum tends to be more robust than the anterior, making these fractures more susceptible to apex anterior angulation6 (Figures 1 and 2).
Figure 1. Significantly displaced proximal humerus fracture with anterior angulation and shortening.

Figure 2. Deforming forces around the proximal humerus. a) The supraspinatus, infraspinatus, and teres minor insert into and externally rotate the greater tuberosity. b) The subscapularis inserts into the lesser tuberosity and pulls the tuberosity anteromedially. c) The pectoralis major inserts into the intertubercular sulcus and displaces the shaft of the humerus anteromedially. d) The deltoid inserts into the deltoid tuberosity of the humeral shaft and abducts the humerus. Figure created with BioRender.com.

In addition to comminution, which can block reduction, a number of soft tissue structures can be interposed in the fracture fragments, including the biceps,7 periosteum, deltoid muscle (Figure 3), or glenohumeral joint capsule.
Figure 3. Puckering of the skin after proximal humerus fracture demonstrates likely entrapment of the anterior deltoid.

Anatomically, surgeons have to consider adjacent structures which could be compromised in obtaining reduction/fixation, and chief among these is the axillary nerve. O’Shea et al. describe that the axillary nerve is typically found at a distance from the lateral edge of the acromion equal to 18.6% of the humeral length, allowing for relative localization of the nerve in even young children.8 Another means of avoiding injury to axillary nerve branches is by utilizing the “one mountain, three valleys” concept as described by Stavinhoa, et al.9 This MRI-based study of children aged 10-17 found that by calculating the vertical distance from the lateral-most aspect of the proximal humeral physis to the apex of the physis then multiplying this number by three, defined the distance distal to the lateral physis where no axillary nerve branches are crossing. Incising skin only, using blunt dissection to the level of the fracture, and utilizing a drill sleeve can limit risk of injury to traversing branches of the nerve.
Another factor to consider is time to treatment—greater than 10 days after injury risks inability to reduce fractures in a closed manner. In many cases, these injuries are indicated for treatment as a result of polytrauma. Thus, surgical stabilization of proximal humerus injuries may occur days later resulting in muscle contracture of the deltoid, biceps, pectoralis major, and latissimus teres requiring mandatory muscle relaxation. In this time period, the proximal humerus and shoulder can swell significantly and make implant placement even harder.
With these challenges in mind, the purpose of this manuscript is to describe strategies and a technique for reduction and percutaneous fixation of proximal humerus fractures.
Description of the Method
Closed Reduction
There are a number of factors that may contribute to the likelihood of success of closed reduction and the orthopaedic surgeon will need to be actively involved in preoperative planning and positioning of the patient. The surgical team will require at least two pairs of experienced hands. Multiple hands are needed to reduce (via traction, angulation, and rotation) and stabilize the reduction while implants are placed.
The treating anesthesiologist should be informed that muscle relaxation is required, and the endotracheal tube should be secured on the contralateral side of the fracture. The operating table must allow for the passage of C-arm fluoroscopy and be free from radio-opaque bars that could block imaging of the shoulder. We prefer a diving board table in a reversed position with the head on the “diving board” end and the feet overlying the base. The table can be rotated 90 or 180 degrees so that either the head or operative arm is in the center of the room. Either is acceptable so long as the C-arm can then enter from the head, angled in such a position that the C-arm can “swing through” to obtain an axillary view with the arm abducted 70 to 90 degrees.10 Because of the potential for use of substantial axial traction, special attention should be paid to securing the patient to the table with the use of multiple safety straps. The patient’s head should be laid on a gel donut and secured to the bed with a towel and tape or equivalent (Figure 4).
Figure 4. This patient is secured to the table with multiple straps while his head is stabilized on a gel donut, and his airway is secured with an endotracheal tube placed on the contralateral side.

Some surgeons prefer a plexiglass sheet to be placed under the pads of the table to expand the working area of the operating table and a small blanket bump placed under the ipsilateral scapula and hip.10
The procedure begins with a closed reduction maneuver utilizing axial traction, abduction, and external rotation of the arm. Posterior directed pressure on the fracture apex and the distal fragment while elevating the arm can help reduce apex anterior angulation. Closed manipulation can often achieve acceptable alignment, yet the challenge remains to maintain reduction while stabilization is attempted and often requires persistent axial traction by an assistant.
As mentioned above, one of the challenges is the difficulty in obtaining a reduction because it is very difficult to control the proximal fragment (Figure 5).
Figure 5. Attempts were made to gain fracture apposition with longitudinal traction in this 14-year-old boy, leading to inferior humeral head displacement.
As a result of this issue, if initial attempts at closed reduction fail, a Schanz pin can be placed into the humeral head to hold it in place while the distal fragment is manipulated. A percutaneous incision is made 1-2 fingerbreadths lateral to the acromion with blunt dissection carried to the level of the capsule. Using fluoroscopic guidance, a 4.5 or 6 mm Schanz pin (size may be adjusted depending on the size of the patient) is placed through a drill guide into the humeral head roughly parallel to the physis, advancing at low rotations per minute to avoid undue torque on the proximal fragment (Figure 6). Once secure, the pin can then be used as a joystick to aid in reduction.
Figure 6. A Schanz pin is slowly advanced into the proximal humerus, and a screw guide is used to prevent soft tissue injury.

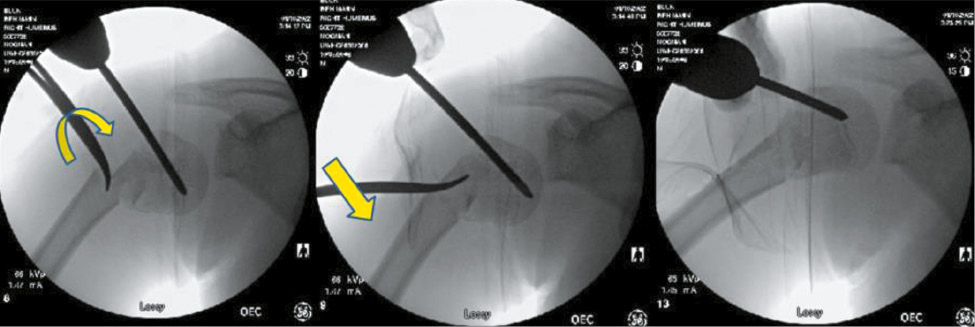
In the process of performing a closed reduction with or without proximal pin stabilization fixation, it is common to find the fracture alignment improved in angulation and cortical contact. If closed reduction is unsuccessful at achieving acceptable alignment, prior to open reduction, one can use a modification of the Kapandji method to reduce the fracture. A stout k-wire or surgical instrument can be percutaneously placed into the fracture site and leverage the fracture fragments into place. We prefer to use a blunt hemostat, as it can be used to gain access to the fracture site safely, and the curved nature can hook the cortex of the “distal bone” and translate to the “proximal bone” to align. Prior to leveraging the bone, one can open the tines of the hemostat when in the fracture site which may prevent comminution during reduction (Figure 7).
Figure 7. The curved portion of the tonsil is then used in a Kapandji-type or shoehorn maneuver: inserted into the intramedullary space, rotated, and used to lever the fracture fragments into a reduced position.
Definitive Fixation with Smooth Pins
With the fracture reduced, the next step is to place wires to either definitively stabilize the fracture or serve as guide pins for cannulated screws. Percutaneous pin fixation is cheaper, and because these fractures heal quickly, they can be removed at 3-4 weeks before pin tract infection can become problematic. When using this method, we use smooth pins that can be removed in clinic, and we have not found the need to use terminally threaded pins. In the senior author’s opinion, we have found that placing these wires is a challenging task. The humeral shaft is relatively narrow compared to the surrounding shoulder girdle which is usually swollen from the trauma. Wires are introduced from distal below the path of axillary nerve and driven from the shaft into the humeral head. The trajectory required to fix both bones requires an oblique entry into hard cortical bone. The entry angle needed for pins to traverse the fracture can prove difficult, as the pins will tend to skive as a more distal-to-proximal trajectory is pursued. Drilling through a drill guide to more firmly anchor the wire, first with the pin perpendicular to the cortex and then slowly angling more proximal once small amount of purchase is obtained, can limit this pitfall (Figures 8 and 9).
Figure 8. The oblique nature of pin entry avoids the axillary nerve but can be difficult to gain entry into the bone. (Figures courtesy Dr. Haemish Crawford).

Figure 9. Use of a drill guide allows the surgeon to stabilize the pin entry site. (Figures courtesy Dr. Haemish Crawford).

If smooth pin fixation is the final planned construct, we will use 3-4 pins that are 2.0 to 2.4 mm in diameter (Figure 10).
Figure 10. A 13-year-old football player, with Division 1 football skills and aspirations, has a significantly displaced proximal humerus fracture treated with closed reduction and pin fixation.

Once the fracture is reduced and stabilized, the arm is rotated under fluoroscopic imaging to ensure fracture stability and that the pins are confirmed to be within the humeral head and not intra-articular. Pins are cut and plastic balls are clamped to pin ends, or the pins are bent over the skin and cut off with sterile felt pads between the plastic ball/pins and the skin. We choose to immobilize in a coaptation splint that extends up over the deltoid for 3-4 weeks, which helps avoid pin migration. We leave this splint on until pins are then pulled in clinic with sling/swath immobilization for another 2-3 weeks. Some practitioners have found that some of these pins can migrate out over time and will then clamp some of the pins together with small external fixation components (Figure 11). Swarup et al. detail placing the patient in either a supine or beach chair position and using closed reduction techniques similar to those outlined above.11 If closed reduction fails, then open reduction via a deltopectoral approach is used. The fracture is secured with two 2.5 mm threaded pins left outside of the skin and further stabilized with a pin-to-pin clamp. Pins are left in place for approximately 4 weeks and removed in the office or under sedation.
Figure 11. After reduction and pin fixation, a small external pin to bar fixator construct can be used to prevent pin migration.

Ho describes a similar stepwise approach to reduction and recommends securing the fracture with two smooth wires that can be removed in 2-3 weeks.6 Ali and colleagues describe the “modified palm tree” method, highlighting the divergent course of the three smooth pins they opt to place with the intent to maximize stability.12 They opt to leave pins in place until radiographic union, typically around 7 weeks. There are no studies to our knowledge comparing smooth versus threaded pins, though experience suggests a lower risk of pin migration with threaded pins.
Definitive Fixation with Cannulated Screws
Initially, we treated all patients with smooth pins, yet concerns of pin site irritation and fracture displacement have led to using cannulated screws as preferred fixation. We use 4.5 mm cannulated screws and place the guide pins with similar techniques as described above. Once three guide pins are placed, we carefully drill (using drill sleeve) the near cortex of the humeral shaft and place fully threaded screws into the metaphysis of the humeral head (Figures 12 and 13). Although we don’t intend to remove, theoretically, fully threaded screws as opposed to partially threaded screws, would be easier to remove if ever indicated at a later date.
Figure 12. A 14-year-old boy from an ATV accident with multiple fractures.
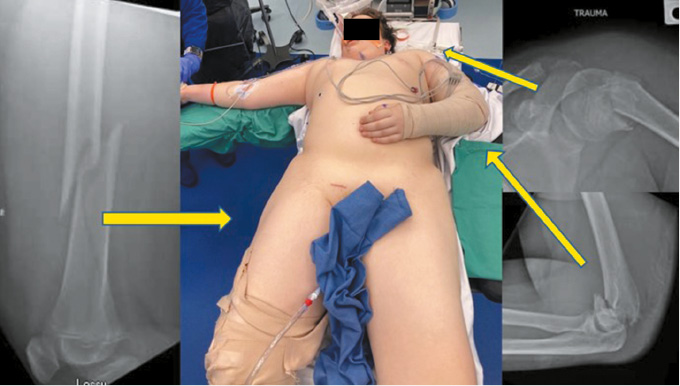
Figure 13. The proximal humerus was treated with closed reduction and screw fixation. At 1 year, he has had good healing and has no complaints of shoulder pain.

Although screw fixation is our preferred methodology, each of these screws is likely to cross some portion of the proximal humerus growth plate. Thus, the surgeon has to be cognizant of indications. In general, younger patients with proximal humerus fractures do not undergo surgical fixation, as their growth plates are more likely to remodel the fracture. Older children and adolescents with less growth potential for remodeling are more likely to need surgical treatment, and early growth cessation would not be expected to lead to clinical problems. That being considered, a younger child that required operative fixation (open fracture or multiple trauma) would be considered for smooth pin stabilization.
Once the fracture is definitively stabilized, the arm should be internally and externally rotated under fluoroscopy to ensure there has been no penetration of the humeral head by the fixation. It is critical to make sure there is no intraarticular penetration by the hardware. In questionable cases, an intraoperative CT scan can be used to definitively document screw placement. The arms are placed in a sling and swath for 3 weeks with pendulum exercises beginning as early as postoperative day 1 and active range of motion is progressed as tolerated at 3 weeks.
Comparison to Other Methods
There are several considerations when deciding which type of percutaneous fixation is best for each patient. Screws allow for more stable fixation and avoid issues with smooth pin migration. Threaded pins are also thought to have decreased risk for migration. In the patient near or at skeletal maturity, screws have minimal consequence to future growth. In patients with significant growth remaining, smooth pins may be more desirable. Screws do not need to be removed, obviating the need for repeat sedation or return to the OR. Additionally, screws avoid the risks of infection and skin irritation that unburied pins impose. In one study, 7/15 patients who had percutaneous fixation with exposed pins developed an infection as compared to 1/9 with buried k-wires.1
Another alternative to percutaneous fixation after closed reduction is flexible intramedullary nailing. Samara et al. describe a technique using closed reduction and a single 3 mm titanium retrograde intramedullary nail, inserted laterally, that resulted in union with satisfactory alignment in their series of 19 patients.13 Techniques with two intramedullary flexible nails have also been described. Hutchinson et al. compared percutaneous pinning to intramedullary nails, noting that use of flexible nails resulted in greater operative time and blood loss but avoided pin-related complications such as pin tract infection and migration, which occurred in approximately 15% of those patients treated with percutaneous pinning.14 Another study found comparable operative times for intramedullary versus percutaneous fixation, and outcomes at mean 5.8 years were similar between groups.15
Plate fixation is rarely used for skeletally immature children. Freislederer et al. report a series of six children and adolescents (ages 8-16) treated with deltopectoral open reduction and internal fixation using a T-plate. It was noted all cases had interposed soft tissue or bony fragments preventing the authors from achieving closed reduction.16 All patients underwent scheduled hardware removal approximately 4 months post injury and had good Constant scores at 2 years postoperatively.
Summary
Pediatric proximal humerus fractures can tolerate a greater range of angulation than many other fractures secondary to the substantial remodeling potential and wide arc of motion of the shoulder. When angulation and displacement are unacceptable, our technique of closed reduction combined with percutaneous reduction and pin or screw fixation allows for a reproducible means of achieving acceptable reduction and stable fixation without the need for future implant removal.
Disclaimer
The authors report no conflicts of interest related to this manuscript.
References
- Hannonen J, Hyvönen H, Korhonen L, et al. The incidence and treatment trends of pediatric proximal humerus fractures. BMC Musculoskelet Disord. 2019;20(1):1-7.
- Shahriar R, Hosseinzadeh P. Proximal humerus fractures: what alignment is acceptable in children 10 and up? J Pediatr Orthop. 2021;41(6):S20-S23.
- Dobbs MB, Luhmann SL, Gordon JE, et al. Severely displaced proximal humeral epiphyseal fractures. J Pediatr Orthop. 2003;23(2):208-215.
- Cruz AI, Kleiner JE, Gil JA, et al. Inpatient surgical treatment of paediatric proximal humerus fractures between 2000 and 2012. J Child Orthop. 2018;12(2):111-116.
- Kim AE, Chi H, Niknam K, et al. Management of pediatric proximal humerus fractures: current concept review. J Pediatr Orthop Soc N Am. 2023;5(1). https://doi.org/10.55275/JPOSNA-2023-580.
- Ho C. Upper extremity injuries. In: JA Herring, ed. Tachdjian’s Pediatric Orthopaedics. Elsevier; 2022:1175-1273.
- Al-Omari AA, Alrawashdeh M, Obeidat O, et al. Entrapped long head of biceps tendon in pediatric proximal humerus fracture dislocation: a case report and review of the literature. Ann Med Surg. 2021;67(June):102510.
- O’Shea R, Panwar J, Chu Kwan W, et al. Establishing safe zones to avoid nerve injury in the approach to the humerus in pediatric patients: a magnetic resonance imaging study. J Bone Joint Surg Am. 2019;101(23):2101-2110.
- Stavinoha TJ, Randhawa SD, Trivedi S, et al. The axillary nerve danger zone in percutaneous fixation in the pediatric shoulder: the “1-mountain-3-valleys” principle. J Bone Joint Surg Am. 2022;104(14):1263-1268.
- Miller AN. Proximal humerus fractures. In: Harborview Illustrated Tips and Tricks in Fracture Surgery. 2nd ed. Wolters Kluwer; 2019.
- Swarup I, Hughes MS, Bram JT, et al. Percutaneous pinning of pediatric proximal humeral fractures. JBJS Essent Surg Tech. 2019;9(4):e33.
- Ali AM, Fawzy SI, Moaty M, et al. Treatment of proximal humerus fractures in children with a modified palm tree technique. J Pediatr Orthop Part B. 2018;27(2):99-102.
- Samara E, Tschopp B, Kwiatkowski B, et al. single retrograde intramedullary nail technique for treatment of displaced proximal humeral fractures in children: case series and review of the literature. JB JS Open Access. 2021;6(1):e20.00119.
- Hutchinson PH, Bae DS, Waters PM. Intramedullary nailing versus percutaneous pin fixation of pediatric proximal humerus fractures: a comparison of complications and early radiographic results. J Pediatr Orthop. 2011;31(6):617-622.
- Kraus T, Hoermann S, Ploder G, et al. Elastic stable intramedullary nailing versus Kirschner wire pinning: outcome of severely displaced proximal humeral fractures in juvenile patients. J Shoulder Elb Surg. 2014;23(10):1462-1467.
- Freislederer F, Bensler S, Specht T, et al. Plate fixation for irreducible proximal humeral fractures in children and adolescents-a single-center case series of six patients. Children (Basel). 2021;8(8):635.