
Master’s Surgical Technique
Z-plasties for the Pediatric Orthopaedic Surgeon
Boston Children’s Hospital, Boston, MA
Correspondence: Donald S. Bae, MD, Boston Children’s Hospital, 300 Longwood Ave., Hunnewell 2, Boston, MA 02115. E-mail: [email protected]
Received: March 30, 2023; Accepted: May 7, 2023; Published: August 1, 2023
Volume 5, Number 3, August 2023
Abstract
Z-plasty refers to a local soft-tissue transposition using interdigitating triangular flaps and is a simple but powerful surgical technique to transpose skin, lengthen scars, and shift topography. There are a host of applications of this technique within pediatric orthopaedics, given the spectrum of traumatic, post-traumatic, and congenital differences affecting the growing child. The purpose of this Master’s Surgical Technique supplement is to describe the principles and common applications of z-plasties in pediatric orthopaedic surgery.
Key Concepts
- Z-plasties are defined by the number of triangular flaps, length of the equilateral limbs, and angles subtended by the incision lines.
- As skin and soft tissue are transposed, the central limb of the Z is “lengthened” or “deepened.”
- The basic principles of the two-part z-plasty may be applied to different variations, including z-plasties in series, multi-part z-plasties, and double-opposing z-plasties.
- Meticulous flap elevation and closure will allow for primary healing without ischemic tip necrosis.
Introduction
When faced with congenital, post-traumatic, or developmental disorders, pediatric orthopaedic surgeons are often challenged with skin and soft-tissue issues in addition to musculoskeletal considerations. Syndactyly, constriction band syndrome, burn contractures, or restrictive post-surgical scars are just some examples where additional attention must be given to the skin and subcutaneous tissue. Often, local transposition or advancement flaps may be utilized to aid in surgical reconstruction or address post-operative complications. “Z-plasty” refers to the local soft-tissue transposition of interdigitating triangular flaps and may be used to transpose tissue, lengthen (or shorten) skin, break up scars, and shift topography.1–4
While z-plasty is a simple but powerful surgical tool, not all orthopaedic surgeons are formally trained in the principles or surgical applications of this technique. The purpose of this Master’s Surgical Technique manuscript is to describe the fundamental principles and common applications of z-plasties in pediatric orthopaedic surgery.
Principles of the Two-Part Z-plasty
The principles of z-plasties are best understood by examining the simple two-part transposition. Indeed, all variations and applications are built upon the foundation of the two-part z-plasty. By convention, z-plasties are defined by the number of interdigitating triangular flaps, the length of each limb, and the angle subtended by the limbs. By definition, all limb lengths are equal as are the resultant angles. Figure 1A illustrates a standard, two-part z-plasty. The two triangular flaps are colored blue and red. As the limbs each measure 1 cm and the angles formed measure 60 degrees, this z-pasty would be described as a “two-part, 1 cm, 60-degree z-plasty.”
Figure 1A. A two-part, 1 cm, 60-degree z-plasty. (Figure courtesy of Children’s Orthopaedic Surgery Foundation.)

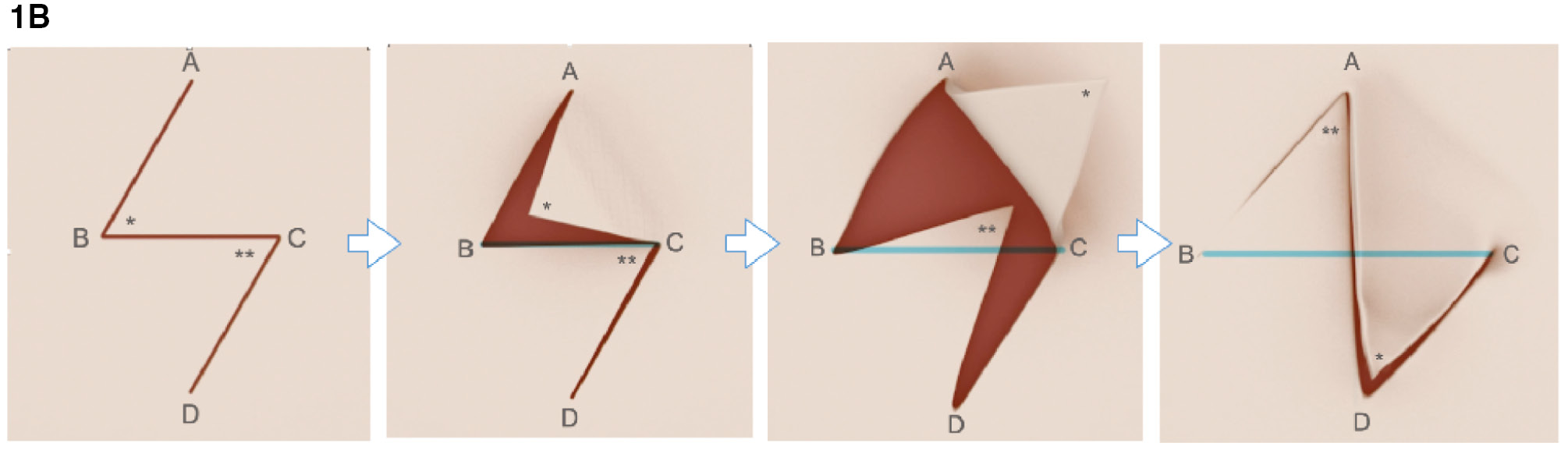
When the skin and soft tissue flaps are elevated and transposed, theoretically, the limb lengths and angles remain constant. However, the direction of the resultant incision lines change. In the example provided, note that flaps have adopted new positions—the central limb of the z-plasty, which previously ran from point B to C, now lies between points A and D (Figure 1B).
Figure 1B. Diagrams depicting sequence of flap transposition in a two-part z-plasty. (Figure courtesy of Children’s Orthopaedic Surgery Foundation.)
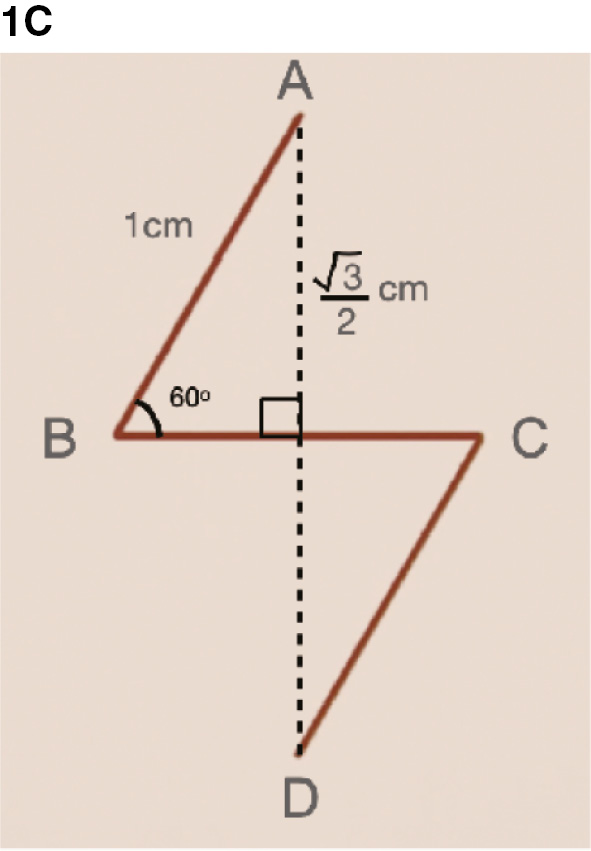
To understand how this transposition resulting in lengthening or recontouring of the soft-tissue, the original z-plasty design is re-examined.4,5 Dropping a perpendicular line from point A to point D will bisect the central limb, creating two right triangles (Figure 1C). As the angle ABC is 60 degrees, a 30-60-90-degree right triangle is formed. Using Pythagorean theorem, the limb opposite the 60-degree angle measures √3/2 cm in length.
Figure 1C. Dropping a perpendicular dotted line, a 30-60-90 right triangle is formed. In this example, the limb opposite angle ABC will measure √3/2 cm in length. (Figure courtesy of Children’s Orthopaedic Surgery Foundation.)
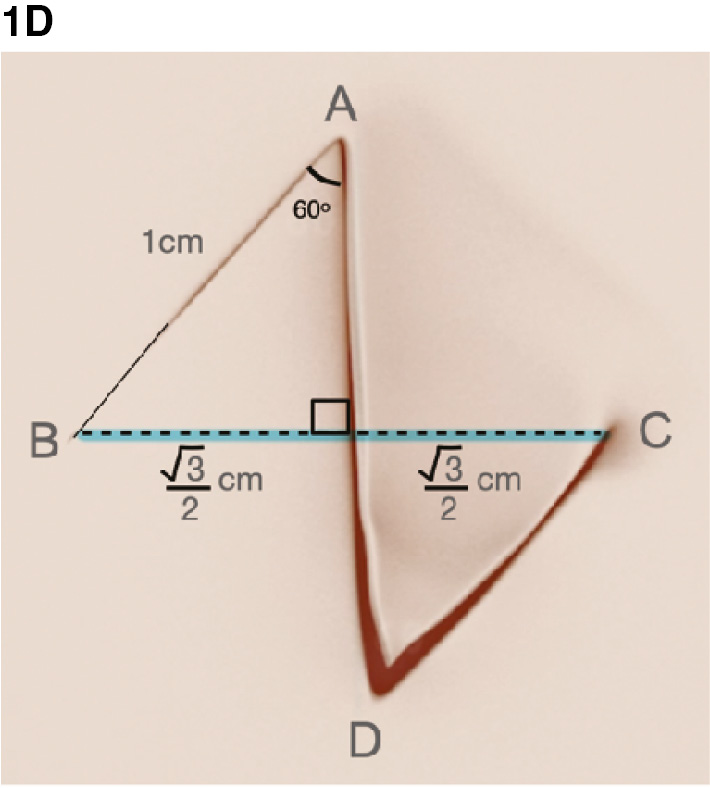
After the limbs are transposed, given that the limb lengths and angles remain constant, the orientation of this perpendicular line is also changed, now lying between points B and C (Figure 1D). The resultant length of the perpendicular line is 2 x √3/2 cm = √3 cm = 1.732 cm. Thus, the lengthening conferred by a two-part 60-degree z-plasty is approximately 75%. Similar derivations can be performed for 30- and 45-degree z-plasties based on the geometry of parallelograms.2,4
Figure 1D. After the flaps are transposed, the distance from point B to point C measures 2 x √3/2 cm = √3 cm = 1.732 cm. Given that line BC originally was 1 cm in length, the resultant lengthening is approximately 75%. (Figure courtesy of Children’s Orthopaedic Surgery Foundation.)
While the geometric foundations behind this two-dimensional transposition are fundamental, a number of practical considerations are worth noting when utilizing z-plasties on three-dimensional tissue. First, z-plasties typically incorporate 45- or 60-degree angles. While wider angles theoretically produce greater lengthening along the central axis (e.g., 100% for 75 degrees), z-plasties that incorporate larger angles result in greater tension on the line of wound closure.4,6 Conversely, smaller angles produce narrower triangular flaps which are more susceptible to flap necrosis given the random-pattern vascularity. Second, any lengthening or deepening achieved by the z-plasty along the central limb is created by adjacent tissue transposition. If the adjacent skin is scarred, immobile, or dysvascular, other means of bringing healthy tissue to the recipient site (e.g., skin graft, peddled flaps) may be warranted.3 Third, it is not uncommon to encounter “dog ears” along the suture lines when the triangular flaps are differentially draped along three-dimensional contours. Judicious suture placement will allow the relatively elastic skin to dissipate tension to facilitate even primary closure. Finally, the theoretical lengthening derived from geometric calculations is not always reproduced in clinical practice, due to the realities of skin pliability, elasticity, and tension lines in individual patients.6 60-degree z-plasties remain the author’s preferred design, as it optimizes the balance of lengthening (75%) and resultant scar orientation (90 degrees from the original orientation of the central limb).7
Variations
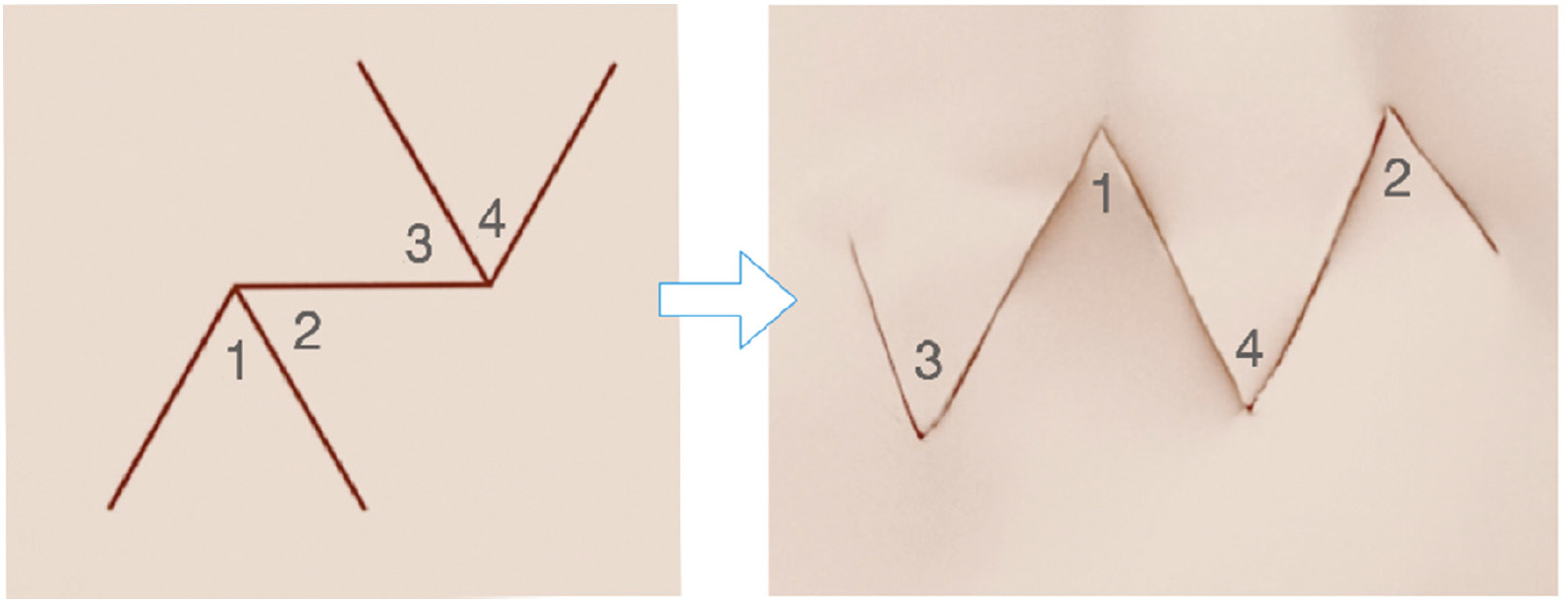
There are a number of variations of the two-part z-plasty that are commonly used in all of surgery, including pediatric orthopaedics.3 The first is multi-part z-plasties in which there are more than two triangular flaps. Figure 2 illustrates a four-part 60-degree z-plasty. Again, as the flaps are elevated and transposed, the length along the original central limb is increased.
Figure 2. Schematic illustration of a four-part z-plasty. Flaps are numbered to illustrate their final position after transposition. (Figure courtesy of Children’s Orthopaedic Surgery Foundation.)
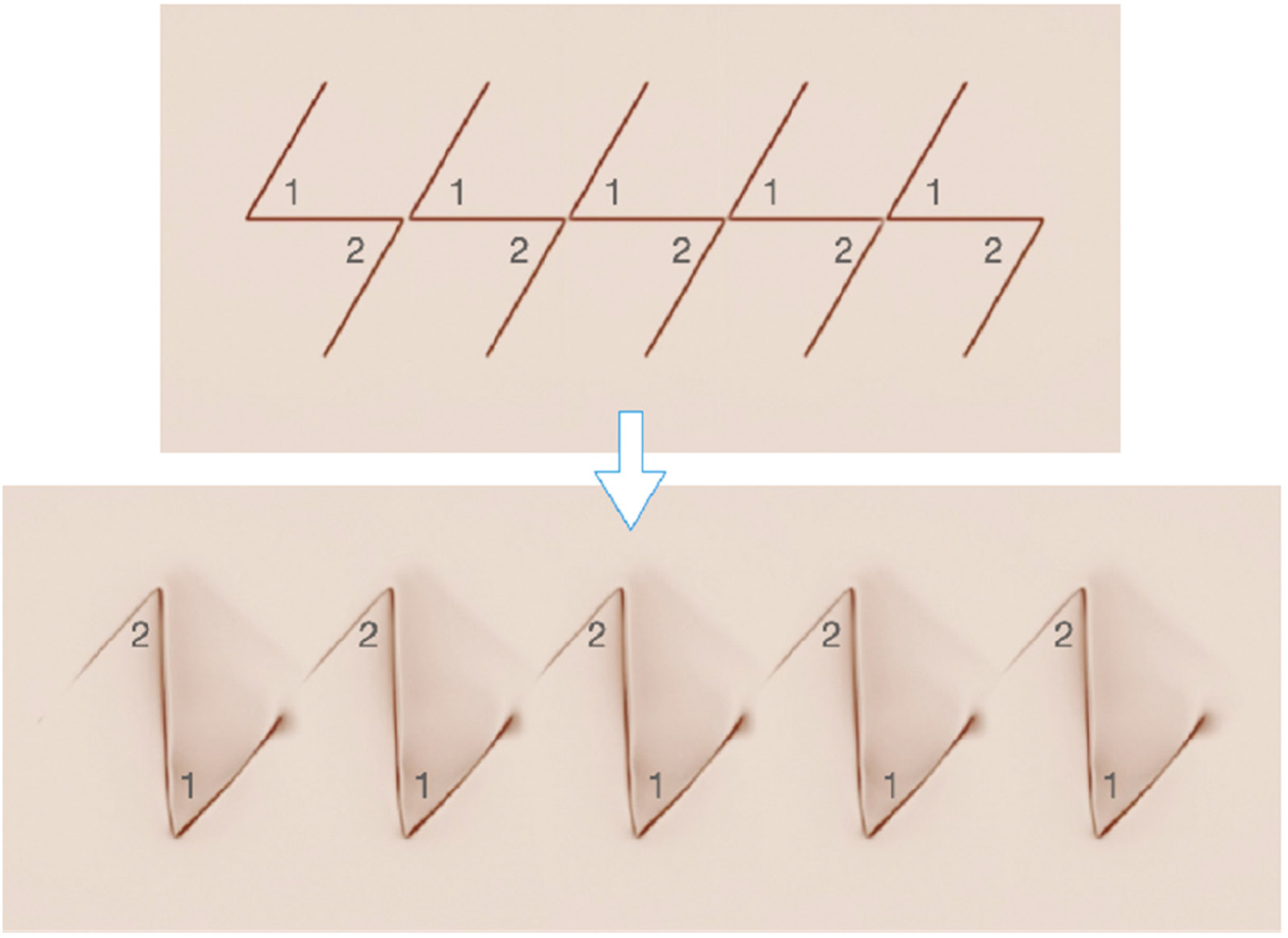
Z-plasties may also be placed in series, repeatedly adjacent to each other with co-linear central limbs (Figure 3). The flaps are similarly elevated and transposed, resulting in aggregate increase in length over a longer longitudinal distance.
Figure 3. Schematic diagram of z-plasties in series. Flaps are numbered to illustrate how they transpose. (Figure courtesy of Children’s Orthopaedic Surgery Foundation.)
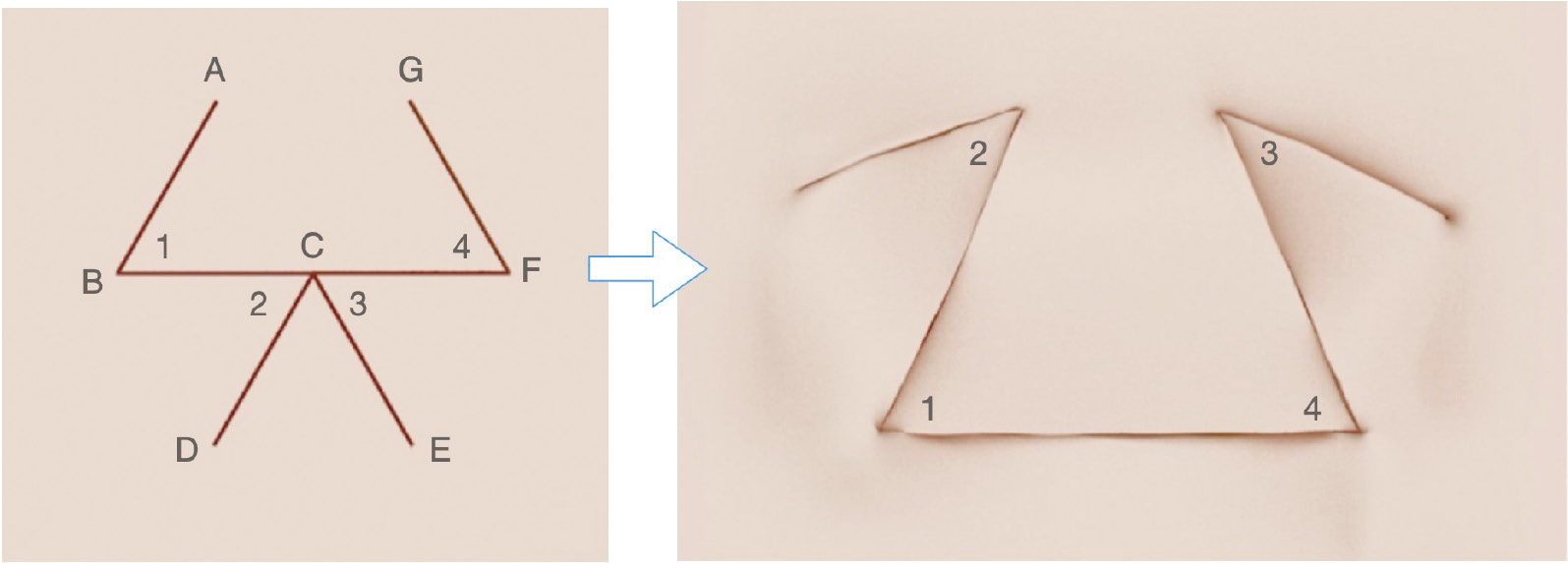
Finally, two z-plasties may be placed in series but in mirror images of each other. This configuration has been called the double-opposing z-plasty (Figure 4). As the flaps are elevated and transposed, the incision line from points D to C to E is lengthened and “flattened” into a straight line, which receives the leading edge BCF of the advancing rectangular flap. Given concerns about tip necrosis of the triangular flaps BCD and ECF, a “stem” is often added; by widening the tips, the theoretical risk of tip necrosis to the random pattern flap is reduced.
Figure 4. Schematic diagram of a double-opposing z-plasty. (Figure courtesy of Children’s Orthopaedic Surgery Foundation.)
Clinical Applications
Clinically, z-plasties are simple but powerful surgical techniques that may be used to lengthen skin or scars, break up lines of tension, and shift topography to create web or cleft depth. The choice of a two-part simple z-plasty versus the other variations depends upon the nature of the problem, the location of the planned transposition, and available adjacent tissue.
Two-part z-plasties may be universally utilized; however, given the fixed length of the incisional limbs, the local tissue availability may not be sufficient to achieve the desired lengthening. Four-part (or even six-part) z-plasties may be considered when the topography of the adjacent soft tissue is limited and a greater lengthening or recontouring is needed. This is most commonly seen in first web space deepening of the hand, particularly in younger patients. Z-plasties in series are ideally suited for lengthening along a longitudinal but relatively narrow segment, such as the digit or extremity. Double opposing z-plasties are ideally suited for interdigital web space deepening, as vascular tissue is advanced into the new web commisure.
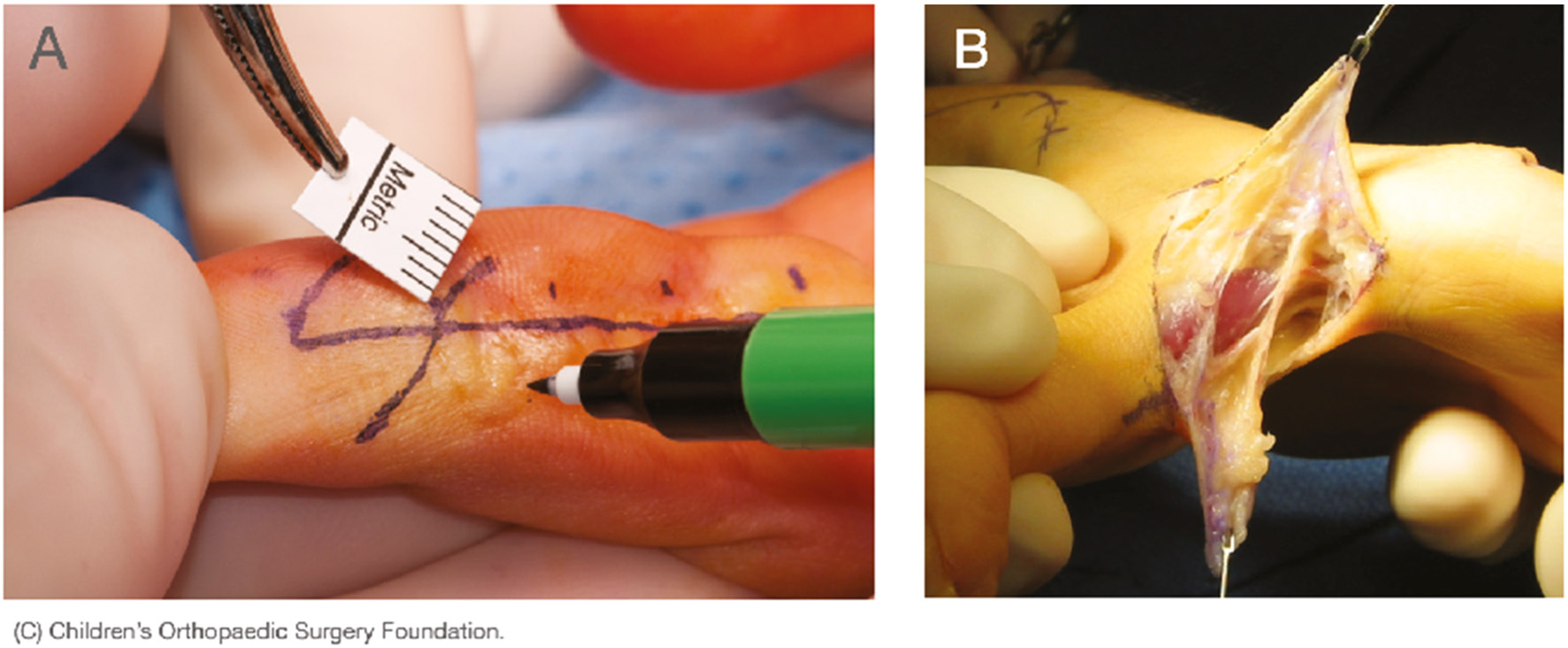
Regardless of which incisional design is chosen, a number of technical considerations bear mention. First, careful measurement and skin marking are important to ensure that the flaps will transpose according to expectations. Typically, we utilize a flexible, paper ruler and a fine-tipped marking pen to carefully mark out the planned incisions (Figure 5A). Second, full-thickness flaps are elevated with the underlying adipose tissue in an effort to preserve the random pattern vascularity of the flaps as well as to optimize the recontouring of the soft tissues (Figure 5B). Failure to elevate full-thickness cutaneous flaps with the underlying fat may increase the risk for flap necrosis and/or suboptimal transposition of the soft tissues. Furthermore, if used in areas of scar tissue, undermining the flaps to release any deep fibrotic tissue is important to optimize soft tissue mobility. Finally, once the flaps are elevated and fully mobilized to their bases, meticulous suture placement is advised. Sutures placed deep within the flap rather than at the skin margins increase the risk of marginal necrosis, particularly in areas of skin tension. In younger children, we typically utilize absorbable sutures with fine cutting needles (e.g., 4-0 or 5-0 Chromic gut suture on P3 needles, Ethicon, Bridgewater, NJ).
Figure 5. (A) Meticulous incision design with ruler and fine-tip marking pen. (B) Full thickness flap elevation in the first web space. (Figure courtesy of Children’s Orthopaedic Surgery Foundation.)
1st Web Space Deepening
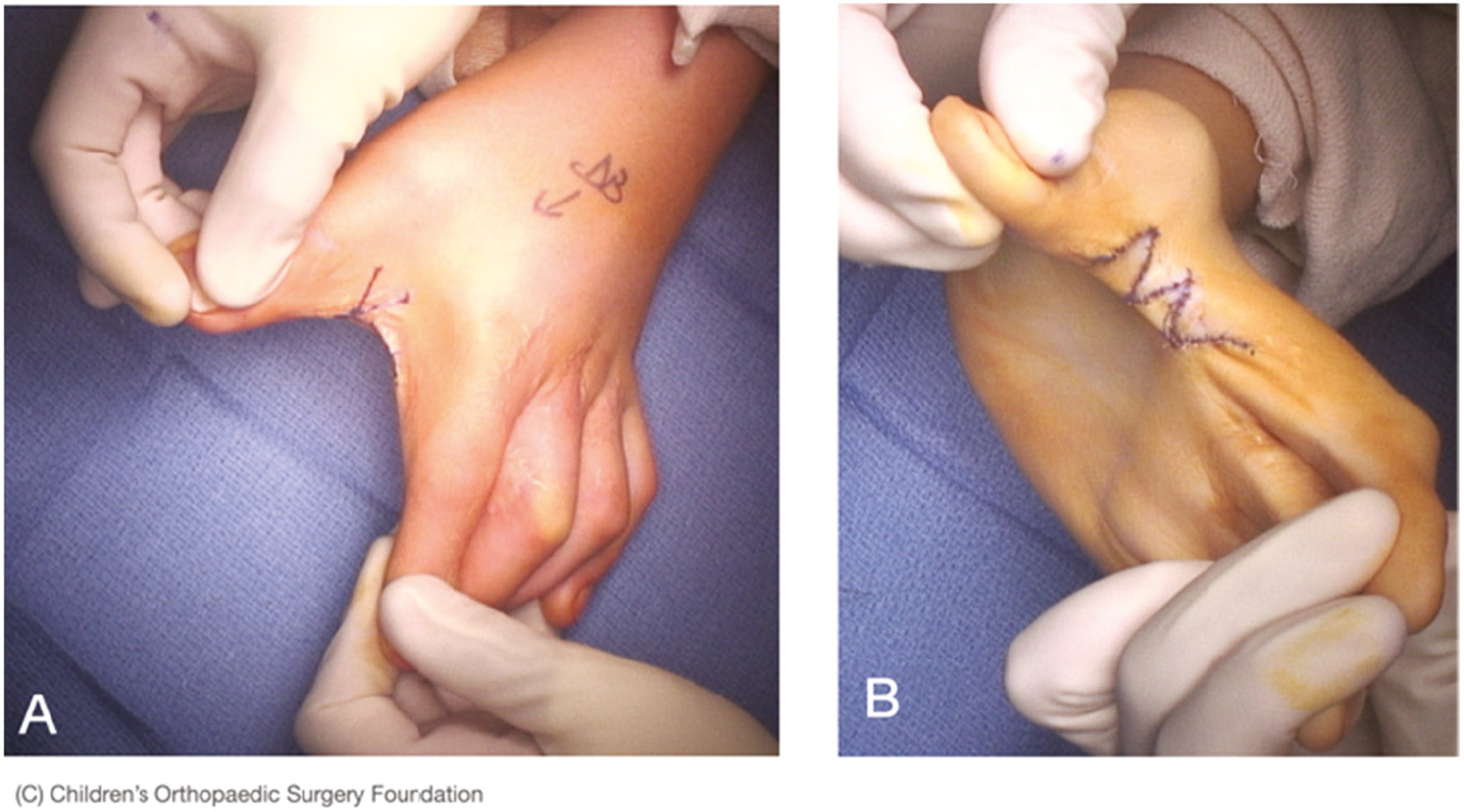
A broad, deep first web space is important for hand function, particularly opposition and large object manipulation. In patients with congenital, developmental, or post-surgical narrowing of the interval between the thumb and more ulnar digits, simple two-part or four-part z-plasties will allow for reconstitution of a wider first web space (Figure 6). As noted above, surgically, the central limb of the z-plasty is placed along the tight leading edge of the web commissure. Typically two- or four-part 60-degree z-plasties are utilized. After careful skin incision and flap elevation, the fascia of the adductor policies may be released to further increase the interdigital span. The heads of the adductor and first dorsal interosseous muscle are typically preserved, though selective tenotomy or muscular release may be performed in some patients (e.g., cerebral palsy, arthrogryposis). After the flaps are rotated, interrupted absorbable sutures are placed for primary wound closure, avoiding “large bites” to preserve vascularity of the tips of the flap.
Figure 6. (A) First web space narrowing due to scar contracture after prior syndactyly release. (B) Restoration of a wider, deeper web space after four-part z-plasty. (Figure courtesy of Children’s Orthopaedic Surgery Foundation.)
Cutaneous Incomplete Syndactyly
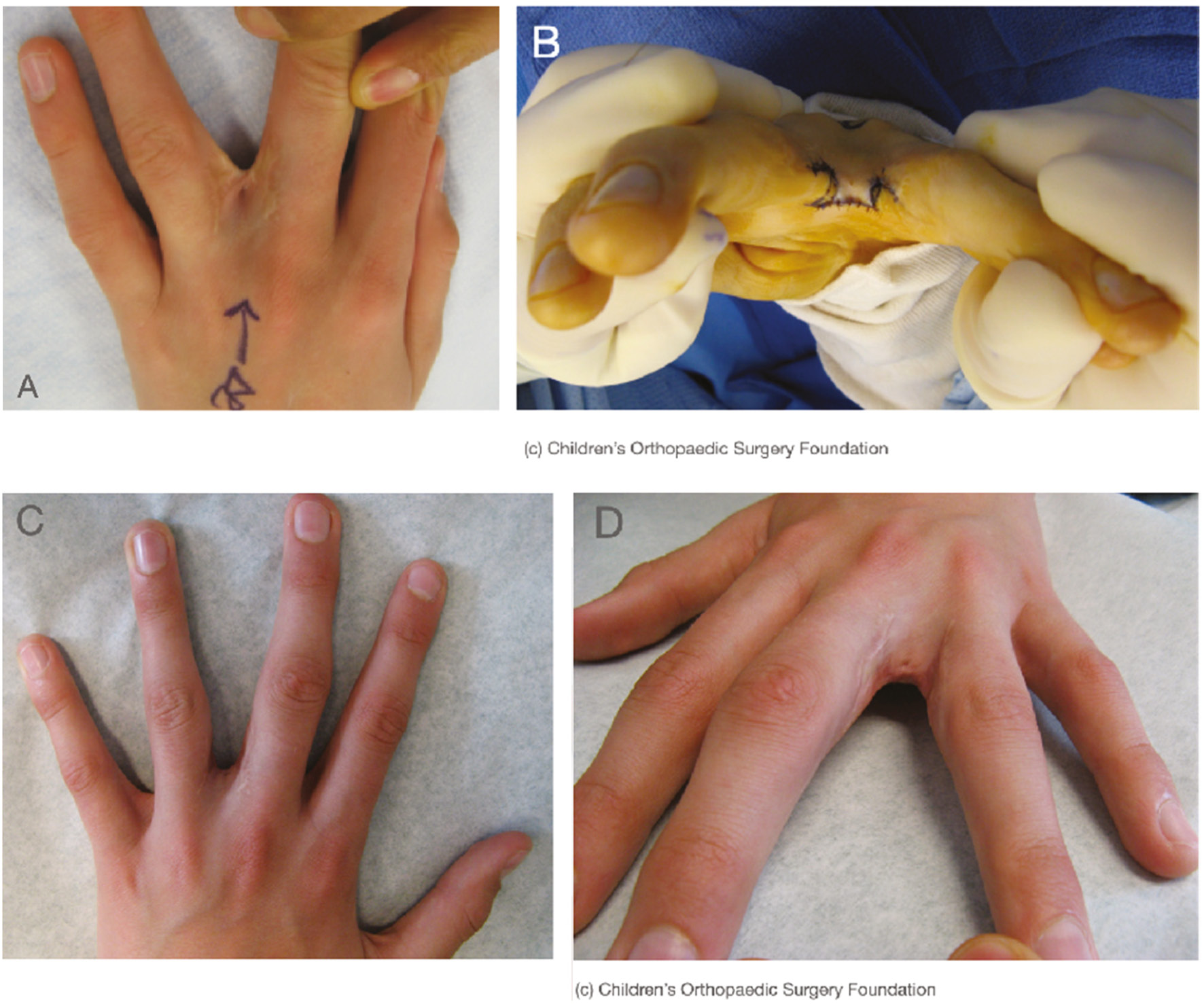
For cutaneous incomplete syndactyly in which the conjoined skin does not extend to the proximal interphalangeal joint or beyond, double-opposing z-plasties are ideally suited to reconstruct a vascular web commissure with the appropriate pliability and contour (Figure 7). Again, the transverse limb of the z-plasty is placed on the leading edge. A “stem” may be placed volarly to widen the tips of the triangular flaps. Elevation of the flaps with the underlying subcutaneous fat and release or excision of any deep scar will allow for reconstitution of the mobile web space.
Figure 7. (A) Preoperative dorsal image of a 3rd web space contracture. (B) Intraoperative photograph after double-opposing z-plasty. (C, D) Postoperative photographs depicting restoration of a normal webspace. (Figure courtesy of Children’s Orthopaedic Surgery Foundation.)
Longitudinal Skin or Scar Contractures
Longitudinal scars or skin contractures can often lead to progressive deformity and functional impairment, particularly when crossing a joint. Common examples include burn contractures of the palm or digits or pterygia crossing the elbow or knee. As these situations commonly affect longitudinal segments of the extremities, with limited available tissue circumferentially around the affected part, z-plasties in series may be utilized (Figure 8). This transposition design will move available local tissue without adversely affecting the dorsal (digit, palm, elbow) or anterior (knee) surfaces.
Figure 8. (A) Preoperative flexion contracture of the middle finger secondary to a burn contracture. (B) Intraoperative use of z-plasties in series. (C) Restoration of full passive extension after z-plasties. (Images courtesy of Children’s Orthopaedic Surgery Foundation.)

Constriction Band Syndrome
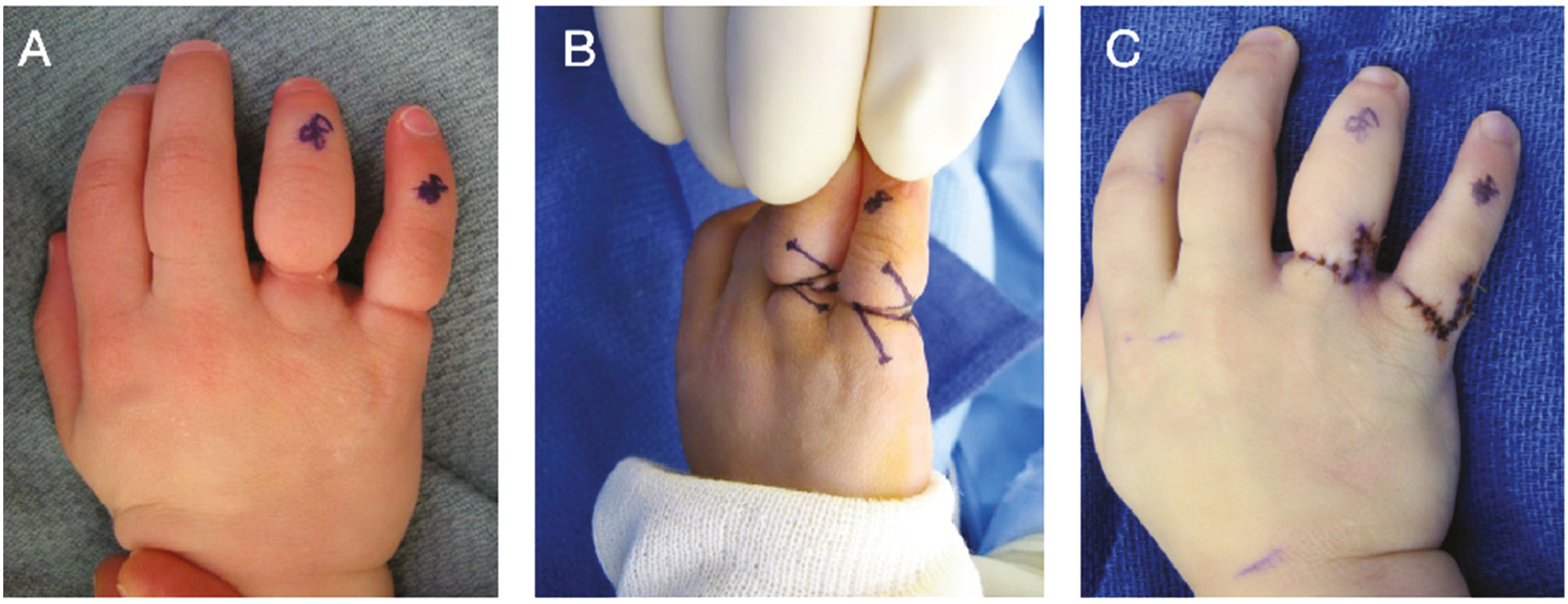
The phenotypic manifestations of constriction band syndrome are variable, ranging from mild cutaneous “bands” to congenital amputations in which there is tissue loss distal to the constriction. In patients with deep bands, there may be distal lymphedematous changes beyond the constriction site; in these situations, the band may result in an annular—not linear—contracture.3 Surgical treatment typically involves both excision of the abnormal constriction band as well as recontouring of the adjacent soft tissue to provide mobile skin and soft tissue and improved aesthetics (Figure 9). Z-plasties in series placed circumferentially around the affected part are very useful in these cases; band excision is accounted for by the central limbs of the z-plasties. When utilized in the fingers, very careful flap elevation is needed, as often the neuromuscular bundle is closely apposed to the overlying skin.
Figure 9. (A) Preoperative image of constriction bands of the ring and small finger. (B) Intraoperatively, bands were excised and z-plasties utilized to increase the circumference of the digit. (C) Final intraoperative appearance after flap transpositions. (Images courtesy of Children’s Orthopaedic Surgery Foundation.)
Index Finger Politicization
Z-plasty principles and incision designs have also been used creatively in other conditions, particularly congenital limb differences. One of the most striking examples is the incisions popularized by Buck-Gramcko for index finger politicization in the setting of thumb hypoplasia or aplasia.8 Buck-Gramcko initially proposed incisions that allow for the index finger to be transferred on its neuromuscular pedicle to the position of the thumb, simultaneously reconstituting a broad first web space and avoiding the need for skin grafting (Figure 10). While seemingly complex for the surgical trainee, careful inspection of these incisions reveal z-plasties placed circumferentially around the native index finger. This ingenious adaptation of z-plasty principles is still used by surgeons today, providing reliable soft-tissue transposition in the creation of a more functional pollex and ultimately improved function in countless patients with hypoplastic or absent thumbs.
Figure 10. Circumferential images around a left hand with an absent thumb. Buck-Gramcko’s incisions for index finger politicization are outlined in black. “Z-plasties” are delineated in blue. (Images courtesy of Children’s Orthopaedic Surgery Foundation.)

Summary
Z-plasties provide a simple, reproducible, and elegant solution for many skin and soft-tissue problems encountered by the pediatric orthopaedic surgeon. With proper patient selection, thoughtful flap design, and meticulous surgical technique, z-plasties can effectively lengthen tight tissue, break up scar contractures, and recontour soft tissues, providing improved mobility and function for children with a variety of congenital, developmental, and post-traumatic conditions.
Acknowledgements
The author wishes to acknowledge Aimee Choi, MS, CMI, for her assistance with the illustrations.
Additional Links
Z-plasties for the Pediatric Orthopaedic Surgeon, Donald S. Bae, MD
Disclaimer
The author reports no conflicts of interest related to this manuscript.
References
- Denonvilliers CP. Blepharoplastie. Bull Soc Chir Paris. 1856;7:243.
- McCurdy SL. Z-plastic surgery. Surg Gynecol Obstet. 1913;16:209-211.
- McGregor IA. The z-plasty. Br J Plast Surg. 1966;19:82-87.
- Furnas DW. The four fundamental functions of the X-plasty. Arch Surg. 1968;96:458-463.
- Rohrich RJ, Zbar RIS. A simplified algorithm for the use of Z-plasty. Plast Reconstr Surg. 1998;103:1513-1517.
- Furnas DW, Fischer GW. The Z-plasty: biomechanics and mathematics. Br J Last Surg. 1971;24:144-160.
- Aasi SZ. Z-plasty made simple. Dermatol Res Pract. 2010;2010:982623.
- Buck-Gramcko D. Pollicization of the index finger. J Bone Joint Surg. 1971;53:1605-1617.