
Quality Improvement Case Series
Commentary to Quality Improvement Case Series: Loss of Fixation of a Type IV Supracondylar Humerus Fracture Treated with Three Divergent Lateral Pins
1Seattle Children’s Hospital, University of Washington Department of Orthopaedics, Seattle, WA; 2Stanford University School of Medicine, Department of Orthopaedic Surgery, Lucile Packard Children’s Hospital / Stanford, Palo Alto, CA; 3Texas Scottish Rite Hospital, Dallas, TX; 4Cedars-Sinai Spine Center, Los Angeles, CA
Received: February 8, 2023; Accepted: March 29, 2023; Published: May 1, 2023
Volume 5, Number 2, May 2023
Case Commentary
Jennifer M. Bauer, MD MS

A very unstable supracondylar humerus fracture can quickly humble even the most experienced surgeons. The surgeon in this scenario obtained a great result for the patient. A few things in these difficult cases have helped me, especially focusing on rotational stability. Every fracture is different; thus, we should move away from the dogma held by some that type X needs X number of pins and instead assess the individual fracture and construct’s stability. I owe my understanding of this to my training at Vanderbilt and their continued work on the topic.1–4
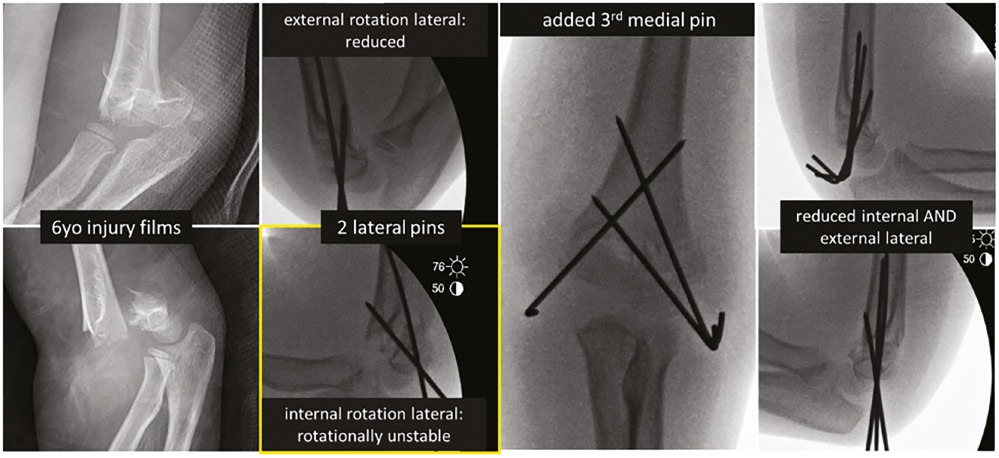
- Internal rotation lateral: there is no way to assess the rotational stability of this pinned fracture without comparing an external rotation to an internal rotation lateral radiograph; it cannot be said with any certainty that this elbow left the OR initially with rotational stability. Most intra-op laterals are external rotation while all post-op laterals are taken in internal rotation—these are not the same, so these radiographs cannot be compared to determine loss of alignment. I am not convinced that either the 1 wk or 2.5 wk postoperative radiographs demonstrate a change to the intra-operative position, only that they are being taken from different angles, which captures the rotation of the fragments, including the medial comminution piece in different views than were obtained intra-op. The attempted lateral at both time points appears unchanged (and even at the 3 mos mark), without loss of the two distal pin fixation points, and with the same medial spike from comminution (note now this appears to be part of the distal piece on 2.5 wk oblique, but part of the proximal fragment on the 2.5 wk lateral). Especially when there is medial column comminution, as with this patient, you may not be able to get a pin flat and low enough to get enough medial column fixation; this is the perfect time to put the elbow in a position of rotational reduction (luckily usually an external rotation lateral) and pass a medial pin. Then, recheck the internal lateral radiograph and prove to yourself the stability the medial pin gained you by the disappearance of that medial spike, which is the column rotating off (Figure 1). In the case presented, I predict that an initial intra-op internal rotation lateral would have shown rotational instability, warranting a medial pin.
- Mini-open medial approach: this has been proven safe in a number of studies and with it, a medial pin need not be avoided. As described in the literature, I do not try to find or see the nerve, only come down onto the directly visualized cartilage/bone of the epicondyle and pass the pin while ensuring no soft tissue becomes caught in the pin.
- Use larger pins: these look like 0.62 pins, which are not as stiff and may lead to torsional weakness of the construct. I routinely use 2.0 mm pins on any elbow over 2 years old, unless I have concerns that my assistant may need several passes for the first pin, and then will switch to 2.0 mm on all subsequent pins. I find many type 3 extension fractures are stable with only two widely divergent lateral 2.0 mm pins. If I place a third lateral, it is because one of my first two lateral pins was not ideally positioned with spread at the fracture, since mechanically, the middle lateral pin does not provide added fixation in the rotational axis.
- Make sure all pins fully cross the far cortex: the highest pin in these limited images appears to only nearly do so. If that is the case, toggle through the fracture from rotational instability, and a less stiff construct with smaller pins may have caused that pin which wasn’t quite fully engaged to back out and lose fixation. This was the only pin that did so.
- These don’t need to be perfect! Kids’ healing is more amazing than our abilities. With all my soapboxing on rotational stability, I have no functional data on its importance. While I do not repeat radiographs until the pin-pull appointment, I likely would have accepted the healing fracture at 2.5 weeks since Baumann’s angle looks within normal range. However, the surgeon is still to be commended for being proactive about their concerns.
Figure 1. Intra-operative images for patient to exemplify internal rotation stability testing.
Case Commentary
Steven Frick, MD

I agree with the comments from Dr. Bauer about the importance of assessing rotational stability with an internal rotation view as well as the value of increasing pin size in very unstable fracture patterns.5 I also commend the authors on taking care of a very difficult problem well. A perfused pulseless supracondylar humerus (SCHF) fracture with comminution is a challenging injury and coupled with an ipsilateral distal radius fracture is at high risk for developing ischemia and compartment syndrome. I agree with the emergent treatment of this injury. We don’t have images of the distal radius and ulna fractures, but my preference is to stabilize those injuries first, bend the pins and wrap the wrist with Coban, and then proceed with reduction and fixation of the elbow. A key point for any pinning of a SCHF is the importance of good bone purchase by each pin—first in the distal fragment and then across the fracture and in the proximal fracture fragment—thus the surgeon needs to feel that each pin has good purchase in bone on one side of the fracture and then again on the other side.
The pin construct itself looks excellent (grade A), with three pins with apparent bicortical fixation with good pin spread—one pin crossing in the lateral third of the distal humerus at the level of the fracture, one pin in the central third, and one pin in the medial third. (See Scannell JBJS 95:1913 for grading reduction and pin constructs.)6 After pinning, I place the elbow first in maximum external rotation and then fluoroscopically look at the fracture during flexion and extension of the elbow. Then, under live fluoroscopy, I look at the fracture as I go from maximum external rotation to maximum internal rotation.7 Any motion between the two fracture fragments leads me to revise my pin construct, most commonly adding a supplemental medial pin.
Deciding on a method of safe immobilization after severe SCHF, particularly in the setting of loss of the pulse, is very important. With a perfused pulseless fracture and an ipsilateral forearm fracture, I agree with the use of either a splint or a bivalved above-elbow cast that would allow easy palpation of the forearm if there were any early postoperative concerns for swelling and compartment syndrome. I also tend to cut out a place in the splint or the cast for post-operative monitoring of the radial pulse.
In very unstable fracture patterns, I think it is also helpful to take fluoroscopy views in the operating room after you have placed your splint or cast. In this case, the final fluoroscopic x-rays in the sagittal plane show the elbow is flexed about 15 degrees above neutral, yet the initial x-rays in the splint in the office show the elbow to be extended about 15 degrees below neutral, with about a 30-degree difference. In this case, if the surgeons had looked at the elbow in the operating room with the elbow extended, they may have seen some instability or malposition. Hennrikus8 noted the risk of loss of flow in the radial artery distally with elbow flexion above 90 degrees after SCHF; thus, in severe injuries like this case, the elbow will be immobilized in 60-80 degrees of flexion. In this more extended position, there may be loss of reduction and so the surgeon should check stability with live fluoroscopic flexion-extension as well as rotation and imaging in the OR after the cast or splint is applied. When concerned about very unstable fractures, follow-up at 1 week for radiographs makes sense. I think the subsequent radiographs show a change in position between the first week after surgery and day 17.
At day 17, I agree with the authors’ decision-making. I treat a nascent malunion of the distal humerus in the first 6 weeks after pin fixation with repeat closed or open manipulation and repeat pinning as was done here. One final point about perfused pulseless SCHF cases is the concern for development of avascular necrosis of the trochlea after these severe injuries. I follow perfused pulseless SCHF longer than the typical 9 to 12 weeks and have them return for a final x-ray 6 to 12 months after the injury to look for any signs of osteonecrosis.
Case Commentary
Christine A. Ho, MD

There are several radiographic features that should alert the surgeon that this fracture is going to be a bad actor—it is a posterolaterally displaced SCH Fx with comminution and the medial metaphyseal spike is buttonholed over the flexor-pronator mass. In addition, the patient clinically has a pink pulseless hand, positive brachialis sign with ecchymoses, and concomitant displaced forearm fracture, all of which speak to the high severity and energy of the injury. In this scenario, the surgical plan should be to reduce and pin this fracture on an arm board rather than the flat camera of the C-arm, as this will facilitate having the C-arm rotate for lateral views rather than rotating the unstable elbow and displacing the fracture. In addition, the surgeon should communicate to the surgical team that they should have a minor bone tray ready in the room in case an open reduction is required to extricate the medial metaphyseal spike, as well as a sterile Doppler to assess the radial artery flow after pinning if the radial pulse is still not palpable.
Once a SCH Fx has been identified as unstable intra-operatively, I personally have to prove to myself that an all-lateral pinning construct is stable. After pinning, I stress the fracture live under fluoroscopy as well as obtain an internal rotation lateral. Watching your construct fall apart is humbling but also informs me that a medial entry pin is needed. In addition, paying close attention to the amount of internal or external rotation that the forearm is positioned relative to parallel to the floor when you obtain the “best lateral” view in the OR also corresponds the amount of malrotation that is present in the reduction. I recommend getting (and saving!) the “worst” lateral view if one accepts malrotation, as this is often the view that you get in clinic. I agree with Dr. Bauer that I am not convinced that there is truly a change in the malrotation of the fracture compared to what was accepted intra-operatively and that there is still malrotation present at the final follow-up radiograph.
Deciding to revise a SCH Fx is never easy. In these cases where I am considering this, I examine the child’s elbow under fluoroscopy in our fracture clinic to see if I can obtain the “same” lateral view (which is typically not the perfect lateral view with the forearm parallel to the floor) that was saved from the OR fluoroscopy. If I can obtain the same view that was accepted intraoperatively, I conclude that there is rotational malalignment that was considered to be acceptable. Given that there are no studies that I am aware of that correlate rotational malalignment of the distal humerus with functional deficiencies (given normal shoulder motion), I personally would not revise fixation for rotational malalignment alone, but I would for hyperextension through the fracture site or clinically apparent coronal plane deformity (especially varus that can be accentuated by excessive internal malrotation). Based on 3D printed models that I have made of malrotated SCH Fx (Figures 2 and 3), I would estimate that this particular SCH Fx is internally malrotated around the intact lateral column about 15-20 degrees. Is this functionally significant? Who knows? In this case, I likely would have accepted the malrotation at 2.5 weeks given that there does not appear to be sagittal or coronal plane malreduction.
Figure 2. Lateral view of a 3D printed model of SCH Fx in 15 degrees of internal rotation with an intact lateral column (Figure courtesy of Dr. Ho).

Figure 3. Lateral view of a 3D printed model of SCH Fx in 20 degrees of internal rotation with an intact lateral column (Figure courtesy of Dr. Ho).

Case Commentary
Kenneth David Illingworth, MD and
David Skaggs MD, MMM


Aww yes, the unstable type IV supracondylar humerus fracture. The fracture that can humble even the most experienced pediatric orthopaedic surgeon and strike fear into fellows and junior attendings everywhere. But even amongst type III and type IV patterns, not all fractures are created equal. Before even going to the operating room, we know this case is a supracondylar “plus.” The degree of displacement is obvious, but on closer look, one can appreciate areas of comminution on the distal segment. In addition, there is comminution along the medial column of the proximal fragment. These “bonus” pieces make the fracture inherently more unstable, even with a near-perfect reduction. This leaves little room for error when considering the remaining factors that put you at risk for loss of reduction.
At first glance, the intra-operative photos show a successful operation and likely a “high five” situation upon leaving the operating room. It is easy to play “Monday morning quarterback” here, knowing the sequence of events that unfolded; however, there are things we can critique on the intra-operative fluoroscopic images.
First, there are signs of malreduction in multiple planes. In orthopaedics, anatomic reduction inherently provides stability. Now, the comminution certainly contributes to this challenge, and we certainly have our own cases of malreduction which don’t result in clinical significance. Here, there are signs of some coronal and sagittal plane malreduction and likely rotational malreduction (which is difficult to assess from the views provided but likely, given the post-operative films). Multiple planes of malreduction may result in decreased fracture stability and leave yourself prone to suboptimal pin placement, despite classic AP and lateral views demonstrating adequate positioning.
Second, is the pin construct. The spread of the pins here is wonderful and they did a good job of capturing the medial column just above the area of comminution that can be seen on the injury films. What is unclear here is whether the lateral column pin sufficiently engages the posteromedial cortex. Pins should be confirmed to be adequately bicortical to avoid a potential risk factor for loss of reduction. On the lateral view, we have routinely advocated for a pin to go from a slightly anterior to posterior direction (Figure 4). This allows you to capture some of the ossification of the lateral condyle, which in theory, provides improved fixation over purely being in the cartilaginous lateral condyle. In addition, in kids older than 5 years, we will often use 2 mm k-wires, which is a significantly more rigid pin and likely increases fixation. What we cannot gain from the fluoroscopic images was how many passes were needed to place these pins. Smooth pins are just that, smooth, and a single pass in the correct position under fluoroscopic guidance, without “swiss-cheesing” the bone, optimizes pin fixation. We emphasize to our trainees when putting these pins in to have “orthopaedic zen,” full speed and slow advance through the far cortex without plunging or pulling the pin back, to eliminate unnecessary pin manipulation once it is in its desired location. The best chance at fixation is the first chance/pass.
Figure 4. Three lateral-based pins for unstable type 4 supracondylar humerus fracture. You can appreciate the anterior to posterior trajectory of one of the k-wires taking advantage of the bony purchase of the ossification of the capitellum. In addition, two of these pins are 2 mm, one 0.062 k-wire. 2 mm k-wires provide increased construct rigidity.

Another important tip, especially in the setting of allowing for some malreduction, is to save fluoroscopic images which demonstrate the greatest degree of displacement/malreduction. This will allow you to compare to post-operative radiographs which may not be the same exact view that you were able to obtain in the operating room. Although, in this case, it appears there has been loss of reduction over time. How do we know that for sure? All six post-operative radiographs are different from the intra-operative fluoroscopy images. It is possible we are getting clearer views of the malreduction over significant loss of reduction? We think this is the more likely scenario.
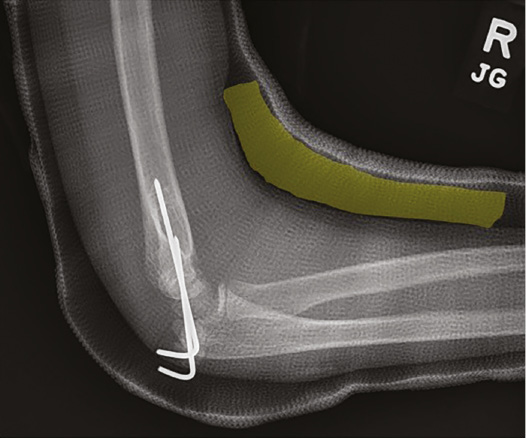
Regardless of fracture type, one critical component of the operation is to clearly demonstrate intra-operative stability prior to completion of the case as the other experts have clearly expressed. We always perform varus/valgus, flexion/extension, and rotational stress testing prior to determining the final pin construct. If there are any signs of coronal, sagittal, or axial plane instability, your job is not complete! Although we feel strongly that medial entry pins are rarely needed to achieve intra-operative stability, we will not hesitate to place medial entry pins, if necessary, especially in the setting of medial column comminution. With a stable construct intra-operatively, one can place post-operative immobilization which protects the pins and allows for post-operative swelling but is not relied upon for providing fracture stability. Our preference is to place a circumferential long arm fiberglass cast with sterile foam applied to the antecubital fossa to allow for swelling as needed (Figure 5). We have found this to be safe, reliable, and without need for cast modifications.9 Even in the setting of an ipsilateral forearm fracture, we employ this technique if there are no intra-operative concerns for excessive swelling. Again, if the cast is needed to provide stability to the construct, you have not adequately completed your surgical objective. If there are significant concerns for swelling or vascular compromise, we will place the child in a plaster splint to allow compartment checks and neurovascular examinations.
Figure 5. Lateral post-operative radiograph demonstrating placement of sterile foam (yellow) within the cast placed at time of surgery. This allows for ample room for swelling and prevents a tight cast. The cast protects the percutaneous pins but should not be relied upon for providing significant stabilization to the fracture/construct.
Additional Links
- JPOSNA® Vol. 5, No. 2: May 2023, Loss of Fixation of a Type IV Supracondylar Humerus Fracture Treated with Three Divergent Lateral Pins
Disclaimer
The authors have no conflicts of interest to report related to this manuscript.
References
- Bauer JM, Stutz CM, Schoenecker JG, et al. Internal rotation stress testing improves radiographic outcomes of type 3 supracondylar humerus fractures. J Pediatr Orthop. 2019;39(1):8-13.
- Rees AB, Schultz JD, Wollenman LC, et al. Internal rotation stress test reduces cross-pinning and improves outcomes in displaced pediatric supracondylar humeral fractures. JBJS Open Access. 2021;6(3):e21.00014.
- Prusick VW, Gibian TJ, Ross KE, et al. Surgical technique: closed reduction and percutaneous pinning of posterolaterally displaced supracondylar humerus fractures. J Orthop Trauma. 2021;35(3):e108-e115.
- Rees AB, Schultz JD, Wollenman LC, et al. A mini-open approach to medial pinning in supracondylar humerus fractures may be safer than previously thought. J Bone Joint Surg Am. 2022;104(1):33-40.
- Srikumaran U, Tan EW, Erkula G, et al. Pin size influences sagittal alignment in percutaneously pinned pediatric supracondylar humerus fractures. J Pediatr Orthop. 2010;30(8):792-798.
- Iobst CA, Bunhor D, Skaggs DL, et al. Intra-operative bone stability test. Tech Orthop. 2018;33(4):279-282.
- Scannell BP, Jackson JB 3rd, Bray C, et al. The perfused, pulseless supracondylar humeral fracture: intermediate-term follow-up of vascular status and function. J Bone Joint Surg Am. 2013;95(21):1913-1919.
- Mapes RC, Hennrikus WL. The effect of elbow position on the radial pulse measured by Doppler ultrasonography after surgical treatment of supracondylar elbow fractures in children. J Pediatr Orthop. 1998;18(4):441-444.
- Seehausen DA, Kay RM, Ryan DD, et al. Foam padding in casts accommodates soft tissue swelling and provides circumferential strength after fixation of supracondylar humerus fractures. J Pediatr Orthop. 2015;35(1):24-27.