
Current Concept Review
Best Practices for Orthopaedic Treatment of Pediatric Gunshot Injuries
1Department of Orthopaedic Surgery, University of California Davis, Sacramento, CA; 2Shriners Children’s Hospital—Northern California, Sacramento, CA
Correspondence: Amanda T. Whitaker, University of California Davis, Department of Orthopedic Surgery, 4860 Y St., Suite 3800, Sacramento, CA 95817. E-mail: [email protected]
Received: March 5, 2023; Accepted: March 29, 2023; Published: August 1, 2023
Volume 5, Number 3, August 2023
Abstract
Gun injuries arise from increased access to firearms across the U.S. More firearm injuries are presenting to emergency departments and non-trauma centers. Most are treated with antibiotics, bedside I&D, and non-operative stabilization for simple wounds of <1 cm without contamination and stable fracture patterns. More complex injuries (usually caused by high-velocity weapons) with larger soft tissue defects with contamination, bone loss, operative fracture patterns, intraarticular projectiles, vascular injuries, compartment syndromes, and nerve injuries warrant IV antibiotics and further treatment in the operating room. Only 28% of nerve injuries regain function. Loss to follow-up is high (43%). Growth arrest and lead toxicity are long-term sequelae that must be monitored—the new CDC acceptable blood lead level is <3.5 μg/dL. Gun injuries are now the leading cause of death in children. Evaluation of the child’s environment and access to guns and education is important for preventing future injuries on an individual level; however, research and legislation are needed to decrease this epidemic of gun violence injuring and killing children today.
Key Concepts
- Gun injuries are currently the leading cause of death in children.
- Gun injuries with minimal soft tissue damage and contamination can be treated in the emergency room with bedside debridement, oral antibiotics, and splinting.
- Gun injuries with large soft tissue defects, contamination, bone loss, operative fracture patterns, intraarticular projectiles, vascular injuries, compartment syndromes, and nerve injuries warrant further treatment in the operating room and IV antibiotics.
- Children with gun injuries involving the physis should be followed for growth arrests and those with retained bullet fragments close to bone or joints for lead toxicity.
- Education, research, and legislation are necessary to protect children from gun injuries.
Introduction
Firearm injuries are an increasing problem in the United States. Recent data from The Centers for Disease Control and Prevention (CDC) reported that firearm-related injuries are now the leading cause of death in children and adolescents in the United States, surpassing motor vehicle accidents.1 With 29.5% of deaths in children attributed to firearms, this is double the death percentage of the general population.1 Firearm deaths in children ages 1-4 years old were on the rise before the pandemic due to increased handgun access in the home.2 Gun sales were the highest ever in U.S. history during the COVID-19 pandemic, increasing the risk of firearm-related injuries and deaths in our most vulnerable populations now and in the future.3 Between 2009 and 2017, approximately 85,694 emergency visits each year were related to nonfatal gunshot injuries, with unintentional injuries being the most common cause (51%) followed by assault (35%).4 Due to increased firearm injuries in children, many are being treated in non-trauma centers.5 Clear treatment guidelines and descriptions of pediatric-specific variables do not exist.
We realize that guns, gun violence, and politicization of this healthcare crisis can polarize people and perspective. In order to provide an objective and comprehensive review, we felt it important to perform a comprehensive assessment of the available published information using PRISMA guidelines. Searches were conducted through Cochrane, PubMed, Scopus, and Google Scholar. Screening consisted of full-text articles written in English with the following terms in either the title or abstract: pediatric/children, gunshot/firearm, or treatment/management excluding case reports. The second round involved a full review and focus on injury to the extremities. This process was repeated twice to arrive at our final relevant articles from which the references were explored for additional literature.
This review aims to summarize the available literature on pediatric orthopaedic gun injuries of the extremities and identify an evidence-based orthopaedic treatment algorithm for gun injuries in children. We also conclude with areas of need for future research and advocacy to keep children safe.
Reference Selection
As of February 5, 2023, 682 articles were identified from the initial search in Cochrane, PubMed, Scopus, and Google Scholar. Search terms included pediatric, children, gunshot wound, gunshot injury, and extremities or fracture. Exclusion criteria were non-English articles and case reports. Six hundred thirty articles were excluded, and the remaining 30 articles were reviewed in their entirety for injuries to the extremities. The search yielded 10 articles and 12 additional articles from references. In total, 22 articles were identified. This included 18 single-center, 2 multicenter, and 2 database studies. The level of evidence was as follows: one level II, one level III, and 20 level IV studies (Table 1).
Table 1. Summary of published gun injuries and sequelae in children.
| Papers | Injuries | Outcomes | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| First Author | Years | Level of Evidence | Patients | Extremity Injuries | Fractures | Soft Tissue | ED | OR | Infection Superficial | Infection Deep | Amputation | Nerve Injury | Nerve Recovery | Vessel Injury | Joint | Bullet Removal | Nonunion | Malunion |
| Heins6 | 1962-1971 | IV | 131 | |||||||||||||||
| Letts7 | 1964-1973 | IV | 54 | 32 | 15 | 17 | 5 | 1 | 12 | 3 | 5 | 7 | ||||||
| Barlow8 | 1970-1980 | IV | 108 | 27 | 2 | 5 | 3 | 6 | ||||||||||
| Ordog9 | 1973-1983 | IV | 255 | 60 | 21 | 78 | 32 | 21 | 8 | |||||||||
| Valentine10 | 1976-1981 | IV | 90 | 29 | 29 | 7 | 2 | 8 | 7 | 2 | ||||||||
| Stucky11 | 1979-1988 | IV | 85 | 93 | 51 | 17 | 48 | 38 | 2 | 8 | 1 | 7 | ||||||
| Scribano12 | 1983-1994 | IV | 166 | 63 | 58 | 2 | 2 | 0 | ||||||||||
| Victoroff13 | 1985-1989 | IV | 75 | 76 | 23 | 53 | 65 | 11 | 0 | 0 | 2 | 2 | 0 | 1 | 15 | |||
| Stricker14 | 1988-1994 | IV | 51 | 66 | 34 | 26 | 12 | 39 | 2 | 0 | 0 | 12 | 9 | 5 | 0 | |||
| Washington15 | 1991-1994 | II | 37 | 36 | 26 | 17 | 20 | 5 | 6 | 2 | 2 | 5 | 1 | |||||
| Davis16 | 1991-2011 | IV | 740 | 246 | ||||||||||||||
| Arsland17 | 1993-2000 | IV | 22 | 27 | 27 | 6 | 15 | 11 | 1 | 1 | 6 | 3 | 4 | 3 | 2 | |||
| Senger18 | 1999-2010 | IV | 194 | 85 | 49 | 36 | ||||||||||||
| Blumberg19 | 2003-2012 | III | 34494 | 11116 | 2814 | 9349 | 1767 | |||||||||||
| Veenstra20 | 2003-2013 | IV | 303 | 5 | 1 | 4 | 4 | 1 | 1 | |||||||||
| Naranje21 | 2005-2013 | IV | 49 | 58 | 58 | 13 | 35 | 1 | 1 | 9 | 4 | 4 | 2 | |||||
| Dabash22 | 2005-2015 | IV | 10 | 10 | 6 | 3 | 6 | 1 | 4 | 4 | 1 | 1 | ||||||
| Newgard5 | 2006-2008 | IV | 505 | 70 | ||||||||||||||
| Perkins23 | 2006-2013 | IV | 46 | 46 | 44 | 2 | 22 | 24 | 5 | 1 | 6 | 1 | 2 | 6 | 4 | |||
| Allaready24 | 2008 | IV | 14831 | 7401 | 1414 | 5987 | ||||||||||||
| Mazotas25 | 2008-2010 | IV | 107 | 38 | 2 | 2 | 14 | |||||||||||
| Lieu26 | 2008-2018 | IV | 61 | 65 | 25 | 40 | 18 | 7 | 1 | 1 | 1 | |||||||
Demographic Information
Gun violence research in children spans from 1962 through 2018 (Figure 1). There were 52,414 children with gun projectile injuries included in this review.1 Of those injured, 19,583 (38%) had an injury to their extremity.5,7,9–13,15–24,26 The lower extremity was more often involved than the upper extremity (51%).6,11,13,15,17,19–21,23,24,26
Figure 1. Timeframe of pediatric gun injuries studied by 5-year intervals. From 2005-2009 is the most studied timeframe, including 50,600 patients in this review.

Handguns were involved in 76% of the incidents, followed by shotguns (11%), non-powdered weapons (7%), and rifles (2%) (Figure 2).7–11,13–15,17,20–23 Most of the victims were assaulted (63%) or a target for violence, whereas 33% were accidental, 3% were suicide attempts, and 1% were due to law enforcement.8,9,11–14,17–19,23,24 Thirty-six percent had a prior police report, firearm injury, or significant trauma/legal event.13,14
Figure 2. A 2-year-old shot with a pellet gun. A) Clinical image of the entrance wound on her forearm. B) Radiographs demonstrating retained pellet posterior to her humerus.

Older children were more likely to be a victim of gun violence, with 88% greater than 14 years-old.5,6,9,11,12,14,15,17–19,22 They were more likely to be assaulted, compared to younger children who were most often unintentionally shot.8,11,14,23
One-third of pediatric fatalities from gun violence died in the field.5 Mortality once at the hospital was 6% overall; however, when associated with multiple areas of injury, this rose to 12%. There were no mortalities with only an extremity injury.5,9,16,18,24
Fractures were present in 22% (12,926) of all firearm injuries to the extremities (Figure 3).7,9,11,14,15,17,19–24,26 Most involved the soft tissue only (78%).5,7,9,11,14,20,23,24,26 The extremity injuries were treated in the emergency room in 82% and 17% required operative intervention.9,11–15,17–23,26
Figure 3. 3D CT scan A) anterior view and B) posterior view of a left distal humerus fracture due to gunshot through a car with an ulnar nerve injury. Courtesy of Holly Leshikar, MD.

Evaluation and Treatment of Pediatric Gun Injuries
Several good evaluation and treatment diagrams of the orthopedic evaluation of pediatric gun violence victims have been published (Figure 4).15,21
Figure 4. Decision chart for Initial Evaluation of Pediatric Gun injuries of the Extremity. From Naranje SM, Gilbert SR, Stewart MG, et al. Gunshot-associated Fractures in Children and Adolescents Treated at Two Level 1 Pediatric Trauma Centers. J Pediatr Orthop. 2016;36(1):1-5.21 Copyright clearance CC-BY-NC-ND. The Creative Commons license does not apply to this content. Use of the material in any format is prohibited without written permission from the publisher, Wolters Kluwer Health, Inc. Please contact [email protected] for further information.

Antibiotic Usage: After the primary survey, tetanus and antibiotics should be administered.13,21 Cefazolin is recommended for simple, uncontaminated wounds, or other antibiotics depending on the environment of the projectile. For example, ciprofloxacin for pseudomonas if the bullet passed through the shoe and gentamycin if the projectile passed through the bowel and would be at risk for enteric contamination from gram-negative rods. The literature varies on the length of antibiotics; however, most support IV antibiotics for contamination, fractures, and complex soft tissue injuries for at least 48 hrs.12,13 If the wound is less than 1 cm with no contamination (and was not shot through clothes or other objects), a course of oral cefalexin for 7 days or ciprofloxacin for 3 days is sufficient per adult literature; however, this has not been confirmed in children.11,13,21,23,27,28
Management of Vascular and Nerve Injury: A vascular injury is present in 6% of extremities.7,10,11,13–15,17,21–23,26 The vascular status of each extremity should be evaluated using palpation, doppler, and angiography if necessary. If there is an obvious vascular injury, this should be addressed by immediate exploration and repair with possible fasciotomies due to the risk of reperfusion injury.10,21 Examine the path of the bullet based on position when shot (if known) and the entry/exit wounds.7 If the examination is questionable or the path of the bullet was in close vicinity to any major vessels, angiography may be recommended.10 Any limb with compartment syndrome without vascular injury should undergo fasciotomies to prevent further muscle and nerve damage. For limb ischemia time >6 hrs after repair of the major vessel, prophylactic fasciotomies should be considered.29
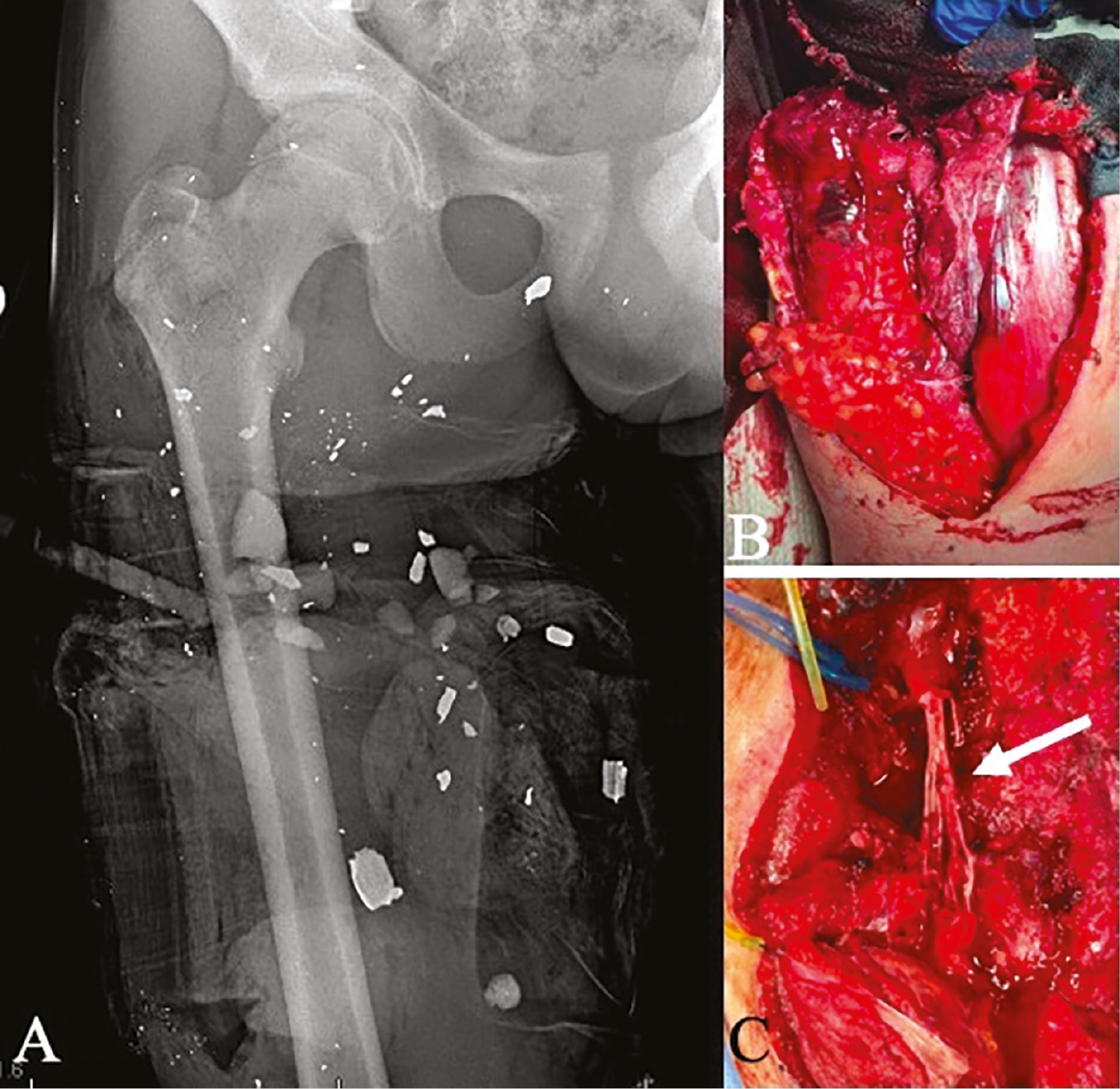
Nerve injury occurs in 11% of children (Figure 6).7,8,10–15,17,20–23,26 Of the 76 nerve injuries, only 28% recovered. Due to the low recovery rate, high rate of transection from the bullet, and high rate of loss to follow-up, several recommend exploring the nerve in the OR so it can be identified and repaired on an acute basis.11,14
Soft Tissue Management: Soft tissue injury varies with the type of weapon (high velocity, low velocity), type of projectile, range, and contamination of the projectile. Antibiotic courses and type of debridement are variable in the literature without clear guidelines for children; however, reported infection rates are low. Infection occurred in 10% of injuries, with 7% superficial and 3% deep, including osteomyelitis.7,10,11,13,14,17,21,25 Simple entry/exit wounds can undergo bedside debridement and irrigation, and simple fractures can be treated with closed reduction and immobilization.8,11–14,20,21,23,26 Late infections have occurred due to retained clothing items.8,25 Larger soft tissue defects usually caused by high-velocity weapons or shotguns, contamination, bone loss, operative fracture patterns, intraarticular projectiles, vascular injuries, compartment syndromes, and nerve injuries warrant further treatment in the operating room.7,9–11,13–15,17,18,21,23
Bone and Joint Injury: The joint has been involved in 6% of firearm injuries (Figure 5).7–9,11,13,15,17,23 Joint involvement is an indication for operative irrigation, debridement, and bullet removal for several reasons. The bullet contaminates the joint and increases the risk of infection, loose bodies, and cartilage injury. When the exit wound is at the joint, there is an increased risk for contractures.7 Bullets and fragments in the joint also have an increased risk of lead toxicity.25,30,31
Figure 5. Gunshot though a knee. A) AP and B) Lateral radiograph of a knee after gunshot injury with fracture visible on the AP and air visible on the lateral. CT (C and D) further demonstrate air in the joint and fracture.
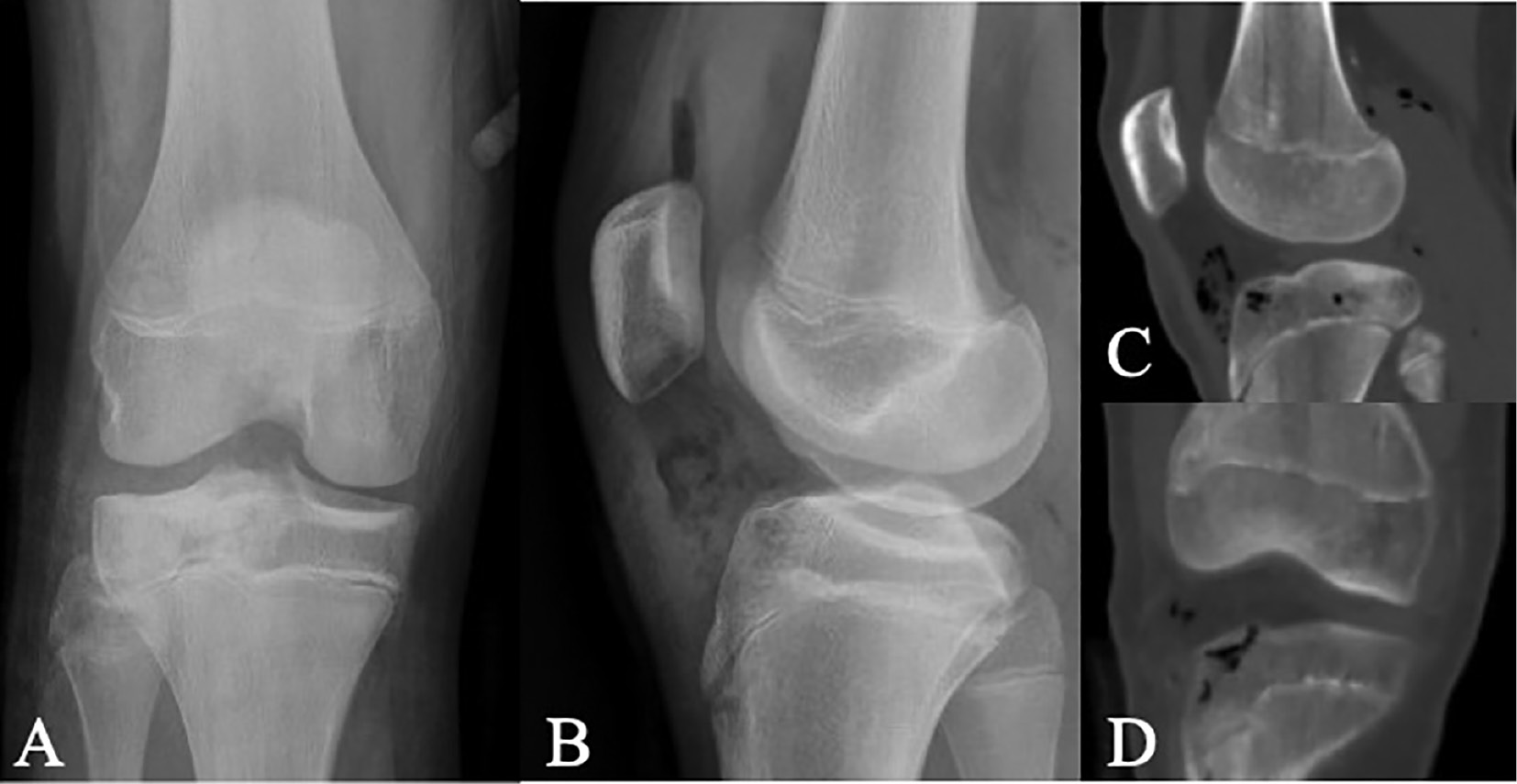
Figure 6. Firearm injury with a rifle with multiple bullet fragments on radiograph A) and large soft tissue defect B). Further evaluation revealed a large sciatic nerve transection. He underwent multiple wound debridement’s prior to undergoing nerve grafting (arrow) C). Courtesy of Holly Leshikar, MD.
Amputations have been reported (Figure 7).17,23 The nonunion rate was 3%, with 66% associated with infection. Physeal injuries were reported in 16% of cases in limited studies.7,15 Letts et al. reported 33% of their physeal injuries did not result from direct trauma to the physis but the bullet passing close to the physis.7 Another reported a case without physeal arrest with direct contact through the physis, and no physeal arrests occurring without contact with the physis.15 This data is limited to a few case series, as follow-up was poor (66%).11,13,14,22,23,25,26
Figure 7. Traumatic amputation of the great toe in a 2-year-old. Courtesy of Dr. Holly Leshikar.

Projectile Removal: Bullets were removed in 14%, either at initial surgery or subsequently due to pain, infection, or cosmesis.13,21,25 Children are at higher risk for lead poisoning with retained bullets due to the length of time the bullet will be present.31 Other factors that increase the risk for lead poisoning are the surface area of the bullet, the number of retained fragments, and the proximity of the fragments to the bone or joint (Figure 8).25,31 The threshold for elevated blood lead levels is >3.5 μg/dL from the CDC in 2021, a drop from >5 μg/dL in 2015, further emphasizing the toxicity and adverse effects of lead.32 The suggested protocol to monitor for lead poisoning is to test at admission, within 2 weeks after injury, monthly for the first 3 months, and then yearly.31 Symptoms of lead toxicity include decreased school performance, slowed growth and development, hearing and speech declines, headaches, abdominal pain, neuropathy, hypertension, encephalopathy, vomiting, and anorexia.30 Discuss with social work and be familiar with your state laws and hospital policies with regard to disposal of the bullet after removal, as some states may require the bullet for later forensics.
Figure 8. This 14-year-old is at risk for elevated lead levels if fragments are not removed due to fragmentation of the bullet, close to bone, and length of exposure to the lead-containing fragments.

Psychology of Gun Violence: There is psychological significant morbidity associated with gun violence, beyond the initial treatment of the injury. Almost half of adult patients have signs of post-traumatic stress disorder (PTSD) after their injury, with increased risk through 5 years.33 Reported employment and physical function decreased. Pain, substance abuse, and alcohol use increased after their injury. PROMIS data was worse in Global Physical Health, Global Mental Health, Physical Function, Emotional Support, and Ability to Participate in Social Roles and Activities. In children exposed to trauma, about 16% develop PTSD; however, this rate is higher with those that are injured as a result of violence, up to 32%.34 In those exposed to a mass shooting event, PTSD ranged from 11-62%.35 Anxiety, depression, somatic disease, and recurrent injuries are high.35 Parents of children who survived mass shooting events had 5 times higher rate of PTSD and 2 times higher rate of depression.35 In adults who have been hospitalized after injury, a multidisciplinary approach with care management, pharmacotherapy, and cognitive behavior therapy decreased PTSD symptoms and increased physical function compared to controls.36 In children who are injured by firearms; the provider should be aware of the high rates of PTSD and provide resources for these children and their families. Research is needed in the prevalence and treatment of the psychological and social effects of gun violence in children and their families.
Discussion
This review illuminated the difficulties with firearm research in children. The numbers presented are smaller than we would expect due to many studies only accounting for those under the age of 15. This is due to many centers being stand-alone children’s hospitals that do not have an adult emergency room as many of the older adolescent gun violence victims are being transported to adult hospitals.
Some findings were not expected. The “watch-and-wait” philosophy on nerve recovery in pediatric gun injuries may not work if 43% of patients do not attend the follow-up appointments, even with casts on.11 The lack of follow-up plus the low return of nerve function (28%) may encourage a more aggressive evaluation at the time of debridement for those that have large soft tissue defects, contamination, or warrant operative intervention.
Younger “accidental” victims of gun violence may live in a neglectful environment and are at higher risk for poor social outcomes.6,9 This includes lack of supervision, poor parental health, a culture of male gun activities, and firearm availability. Social services evaluation should be considered for firearm injuries as we would make mandatory for non-accidental trauma. Good gun safety needs to be practiced in their home environment—if discovered by a 3-year-old, we must recognize that they have the strength to fire most available handguns.37 Young victims of gun injuries are at high risk for future accidents such as more gun violence, motor vehicle accidents, burns, lacerations, and poisonings.6,8 As children get older, many of them (36%) had a significant past trauma history or had been previously shot in the studies reviewed.13 An “unusual number of violent deaths in the immediate family” were also reported.8 One study reported an alarming 19% of gun violence victims were of school age but not enrolled.8
There are many factors on why gun violence is increasing, and more children are falling victim. One of the earlier papers had one pediatric admission in 10 years prior to the change in adult drug offender laws in New York State and 108 admissions in the 10 years after.8 In states with less firearm regulations, pediatric gun injuries are 3.75 times higher.38 Gun-related deaths in children between 1 and 4 years old have risen before the pandemic due to increased handgun access in the home, with 72% of families that own a firearm will have handguns and young children.2 Gun sales were the highest ever in U.S. history during the COVID-19 pandemic, increasing the risk of firearm-related injuries and deaths in our most vulnerable populations.3 This concern demonstrates traction when school gun violence is plotted over the past 10 years with an increase since the pandemic began in 2020 (Figure 9).39
Figure 9. School gunfire, injuries, and deaths from 2013 to 2022.39 There is an increase in gunfire, injuries, and death after 2020 with the increase in gun availability.3

What has not been associated is the relationship between economics and gun injuries in children.16 Also, there appears to be more extremity and multiple-shot traumas over time, suggesting more general violence than targeted assaults.16 In addition, healthcare charges for pediatric firearm injuries has increased by 23.1% from 2009 to 2016 with an average cost of $3642 for an ED visit.24,40 Gun violence will increase healthcare costs for the foreseeable future unless the trend of access and violence is stopped.
What can we do as pediatric orthopaedic surgeons? In our review, patient follow-up was poor, highlighting a missed opportunity for intervention. Physicians are essential in educating parents and the public regarding gunshot injuries.41,42 The American Academy of Pediatrics endorses physicians to counsel children and families regarding firearms, such as proper storage.41 Guns should be locked and unloaded with ammunition locked in a separate location.43 Firearm safety discussions occur in only 4.4% of patient encounters.42 As a pediatric orthopaedic surgeon, “Is there anything else I can do to keep my kids injury-free?” is a frequently heard segue to this topic of conversation.
States with stricter gun laws have lower firearm fatalities in children, with a 59% reduction in unintentional fatalities.44 However, there are powerful lobbies against gun reform. For example, the National Rifle Association successfully lobbied Congress to prohibit funding the CDC and the National Institutes of Health for firearm-related research from 1996-2013.45 Unless we begin considering gun violence as a public issue and create legislation to address this, children will continue to be unnecessarily injured.46
In summary, pediatric gun injuries are a growing issue in the United States due to the abundance of guns and decreased regulation. Most orthopaedic extremity injuries with minimal soft tissue damage can be treated with bedside irrigation and debridement, oral antibiotics, tetanus, and splinting for fractures. However, the most severe injuries will require IV antibiotics, angiography with possible vascular repair, possible nerve explorations and repair, soft tissue debridement with possible soft-tissue coverage, lead level assessment with risk/benefit bullet removal consideration for long-term lead exposure and continued monitoring for physeal growth arrest and lead toxicity. Prevention of these injuries is key with education, strict home gun safety, and increased regulations on firearms and their use.
Disclaimer
The authors report no conflicts of interest related to this manuscript.
References
- Goldstick JE, Cunningham RM, Carter PM. Current causes of death in children and adolescents in the United States. N Engl J Med. 2022;386(20):1955-1956.
- Prickett KC, Gutierrez C, Deb S. Family firearm ownership and firearm-related mortality among young children: 1976–2016. Pediatrics. 2019;143(2):e20181171.
- Bleyer A, Siegel SE, Thomas CR Jr. Increasing rate of unintentional firearm deaths in youngest Americans: firearm prevalence and Covid-19 pandemic implication. J Natl Med Assoc. 2021;113(3):265-277.
- Kaufman EJ, Wiebe DJ, Xiong RA, et al. Epidemiologic trends in fatal and nonfatal firearm injuries in the US, 2009-2017. JAMA Intern Med. 2021;181(2):237-244.
- Newgard CD, Kuppermann N, Holmes JF, et al. Gunshot injuries in children served by emergency services. Pediatrics. 2013;132(5):862-870.
- Heins M, Kahn R, Bjordnal J. Gunshot wounds in children. Am J Public Health. 1974;64(4):326-330.
- Letts RM, Miller D. Gunshot wounds of the extremities in children. J Trauma. 1976;16(10):807-811.
- Barlow B, Niemirska M, Gandhi RP. Ten years’ experience with pediatric gunshot wounds. J Pediatr Surg. 1982;17(6):927-932.
- Ordog GJ, Prakash A, Wasserberger J, et al. Pediatric gunshot wounds. J Trauma. 1987;27(11):1272-1278.
- Valentine J, Blocker S, Chang JH. Gunshot injuries in children. J Trauma. 1984;24(11):952-956.
- Stucky W, Loder RT. Extremity gunshot wounds in children. J Pediatr Orthop. 1991;11(1):64-71.
- Scribano PV, Nance M, Reilly P, et al. Pediatric nonpowder firearm injuries: outcomes in an urban pediatric setting. Pediatrics. 1997;100(4):E5.
- Victoroff BN, Robertson WW Jr, Eichelberger MR, et al. Extremity gunshot injuries treated in an urban children’s hospital. Pediatr Emerg Care. 1994;10(1):1-5.
- Stricker SJ, Volgas DA. Extremity handgun injuries in children and adolescents. Orthopedics. 1998;21(10):1095-1100.
- Washington ER, Lee WA, Ross WA. Gunshot wounds to the extremities in children and adolescents. Orthop Clin North Am. 1995;26(1):19-28.
- Davis JS, Castilla DM, Schulman CI, et al. Twenty years of pediatric gunshot wounds: an urban trauma center’s experience. J Surg Res. 2013;184(1):556-560.
- Arslan H, Subasi M, Kesemenli C, et al. Problem fractures associated with gunshot wounds in children. Injury. 2002;33(9):743-749.
- Senger C, Keijzer R, Smith G, et al. Pediatric firearm injuries: a 10-year single-center experience of 194 patients. J Pediatr Surg. 2011;46(5):927-932.
- Blumberg TJ, DeFrancesco CJ, Miller DJ, et al. Firearm-associated fractures in children and adolescents: trends in the United States 2003-2012. J Pediatr Orthop. 2018;38(7):e387-e392.
- Veenstra M, Patel V, Donoghue L, et al. Trends in pediatric firearm-related injuries over the past 10 years at an urban pediatric hospital. J Pediatr Surg. 2015;50(7):1184-1187.
- Naranje SM, Gilbert SR, Stewart MG, et al. Gunshot-associated fractures in children and adolescents treated at two level 1 pediatric trauma centers. J Pediatr Orthop. 2016;36(1):1-5.
- Dabash S, Gerzina C, Simson JE, et al. Pediatric gunshot wounds of the upper extremity. Int J Orthop. 2018;5(2):910-915.
- Perkins C, Scannell B, Brighton B, et al. Orthopaedic firearm injuries in children and adolescents: an eight-year experience at a major urban trauma center. Injury. 2016;47(1):173-177.
- Allareddy V, Nalliah RP, Rampa S, et al. Firearm related injuries amongst children: estimates from the nationwide emergency department sample. Injury. 2012;43(12):2051-2054.
- Mazotas IG, Hamilton NA, McCubbins MA, et al. The long-term outcome of retained foreign bodies in pediatric gunshot wounds. J Trauma Nurs. 2012;19(4):240-245.
- Lieu V, Carrillo LA, Pandya NK, et al. Pediatric firearm-associated fractures: analysis of management and outcomes. World J Clin Pediatr. 2021;10(6):151-158.
- Dickson K, Watson TS, Haddad C, et al. Outpatient management of low-velocity gunshot-induced fractures. Orthopedics. 2001;24(10):951-954.
- Knapp TP, Patzakis MJ, Lee J, et al. Comparison of intravenous and oral antibiotic therapy in the treatment of fractures caused by low-velocity gunshots. A prospective, randomized study of infection rates. J Bone Joint Surg Am. 1996;78(8):1167-1171.
- Bernot M, Gupta R, Dobrasz J, et al. The effect of antecedent ischemia on the tolerance of skeletal muscle to increased interstitial pressure. J Orthop Trauma. 1996;10(8):555-559.
- Coon T, Miller M, Shirazi F, et al. Lead toxicity in a 14-year-old female with retained bullet fragments. Pediatrics. 2006;117(1):227-230.
- McQuirter JL. Change in blood lead concentration up to 1 year after a gunshot wound with a retained bullet. Am J Epidemiol. 2004;159(7):683-692.
- Center for Disease Control and Prevention. Childhood Lead Poisoning Prevention. Published online May 14, 2021. Available at: https://www.cdc.gov/nceh/lead/default.htm. Accessed February 25, 2023.
- Vella MA, Warshauer A, Tortorello G, et al. Long-term functional, psychological, emotional, and social outcomes in survivors of firearm injuries. JAMA Surg. 2020;155(1):51.
- Alisic E, Zalta AK, van Wesel F, et al. Rates of post-traumatic stress disorder in trauma-exposed children and adolescents: meta-analysis. Br J Psychiatry. 2014;204(5):335-340.
- Ranney M, Karb R, Ehrlich P, et al. What are the long-term consequences of youth exposure to firearm injury, and how do we prevent them? A scoping review. J Behav Med. 2019;42(4):724-740.
- Zatzick D, Jurkovich G, Rivara FP, et al. A randomized stepped care intervention trial targeting posttraumatic stress disorder for surgically hospitalized injury survivors. Ann Surg. 2013;257(3):390-399.
- Naureckas SM, Galanter C, Naureckas ET, et al. Children’s and women’s ability to fire handguns. The Pediatric Practice Research Group. Arch Pediatr Adolesc Med. 1995;149(12):1318-1322.
- Safavi A, Rhee P, Pandit V, et al. Children are safer in states with strict firearm laws: a National Inpatient Sample study. J Trauma Acute Care Surg. 2014;76(1):146-150; discussion 150-151.
- Gunfire on School Grounds in the United States. Available at: https://everytownresearch.org/maps/gunfire-on-school-grounds/. Accessed February 20, 2023.
- Bongiorno DM, Badolato GM, Boyle M, et al. United States trends in healthcare charges for pediatric firearm injuries. Am J Emerg Med. 2021;47:58-65.
- Petty JK, Henry MCW, Nance ML, et al. Firearm injuries and children: position statement of the American pediatric surgical association. Pediatrics. 2019;144(1):e20183058.
- Stokes SC, McFadden NR, Salcedo ES, et al. Firearm injuries in children: a missed opportunity for firearm safety education. Inj Prev J Int Soc Child Adolesc Inj Prev. 2021;27(6):554-559.
- Grossman DC, Mueller BA, Riedy C, et al. Gun storage practices and risk of youth suicide and unintentional firearm injuries. JAMA. 2005;293(6):707-714.
- Azad HA, Monuteaux MC, Rees CA, et al. Child access prevention firearm laws and firearm fatalities among children aged 0 to 14 years, 1991-2016. JAMA Pediatr. 2020;174(5):463.
- Carter CW, Sharkey MS, Fishman F. Firearm-related musculoskeletal injuries in children and adolescents. J Am Acad Orthop Surg. 2017;25(3):169-178.
- Goyal MK, Badolato GM, Patel SJ, et al. State gun laws and pediatric firearm-related mortality. Pediatrics. 2019;144(2):e20183283.