
Original Research
Opioid Prescription Trends for Isolated Diaphyseal Femur Fractures in Pediatric Patients
1Division of Plastic and Reconstructive Surgery, UMass Chan Medical School, Worcester, MN; 2Department of Biomedical Statistics & Informatics, Mayo Clinic, Rochester, MN; 3Division of Pediatric Orthopedic Surgery, Mayo Clinic, Rochester, MN
Correspondence: Todd A. Milbrandt, MD, Department of Orthopedic Surgery, Mayo Clinic, 200 1st St SW, Rochester, MN 55902. E-mail: [email protected]
Received: February 6, 2023; Accepted: May 8, 2023; Published: August 1, 2023
Volume 5, Number 3, August 2023
Abstract
Purpose: Despite the ongoing opioid epidemic, there is a lack of research on narcotic prescribing in the pediatric orthopaedic population. The Pediatric Orthopaedic Society of North America (POSNA) therefore published a survey on pain management to provide recommendations for opioid dosing. The goal of this study was to characterize opioid prescribing patterns for pediatric femur fractures in the context of the opioid epidemic and emerging national studies/guidelines.
Methods: A retrospective review of 128 pediatric patients (age < 16) with isolated diaphyseal femur fractures was conducted between 2003-2019 at a level I pediatric trauma center. Comparison groups included before distribution of the POSNA survey (pre-POSNA = 01/01/2016 or earlier, N = 85) and after the survey (post-POSNA, N = 43).
Results: Median total hospital postoperative opioids prescribed was 27.2 morphine milligram equivalents (MME). The two groups differed in age (pre-POSNA = 9.0 years, post-POSNA = 3.7 years, P = 0.0381), hospital length of stay (LOS) (pre-POSNA = 2 days, post-POSNA = 1 day, P < 0.0001), and procedural incision required for fracture reduction (pre-POSNA = 28.3%, post-POSNA = 58.1%, P = 0.0019). Adjusted postoperative opioid dosing was significantly lower post-POSNA (median reduction of 18.351 MME per year, P = 0.0408).
Conclusions: The period following the POSNA survey was associated with a significant decline in postoperative narcotic prescriptions for pediatric femur fractures. The timing of the survey likely represents an increased concern for pediatric opioid use and a shift in clinical practice. Further work is needed to optimize injury and patient-specific narcotic prescribing.
Level of Evidence: Therapeutic Level III
Key Concepts
- The 2016 POSNA survey identified a lack of consensus on opioid prescribing practices for common orthopaedic procedures in the United States.
- The 2016 POSNA survey and subsequent 2019 published narcotic prescription recommendations represent a shift in the specialty of orthopaedic surgery regarding opioid usage in the pediatric population.
- Postoperative morphine milligram equivalents significantly decreased for the treatment of pediatric diaphyseal femur fractures at a single-level I pediatric trauma center following administration of the 2016 POSNA survey.
Introduction
The United States continues to experience a severe epidemic caused by the overuse and misuse of opioid medications. In 2008, the United States constituted 4.6% of the world’s population but consumed 80% of the global opioid supply.1 The amount of opioids prescribed has tripled in the past 2 decades and deaths related to prescription narcotic overdosing are five times higher.2,3 The situation is similar for children and adolescents: the rate of opioid prescriptions in adolescents doubled from 1994-2007.4 Additionally, 21-25% of high school seniors report having used prescription narcotics, with 4-13% regularly abusing them.5,6
Despite the risk of future abuse associated with legitimate medical opioid use,7 there is still limited research on opioid prescribing patterns and recommendations for pediatric narcotic dosing. For those who sustain orthopaedic trauma, no injury-specific narcotic prescribing guidelines are available. As a result, pediatric patients who sustain femur fractures are prescribed similar amounts of opioids as patients who sustain elbow fractures,8 despite femur fractures being rated as significantly more painful.9
To better understand current practices, the Pediatric Orthopaedic Society of North America (POSNA) conducted a survey in 2016 asking surgeons how they would manage pain for several orthopaedic scenarios.10 The results showed a lack of consensus on how to manage pain in even the most common situations with a wide variety in the total amount of opioids prescribed and length of time for which prescriptions were provided. A need for national recommendations was identified and have since emerged.11 The timing of the survey and subsequent guidelines represent a significant shift within the specialty of orthopaedic surgery in consideration of narcotic use in children.
To determine whether this period of increasing awareness of the opioid epidemic and emerging standardized narcotic prescriptions are associated with significant clinical practice changes, we sought to characterize the postoperative opioid prescribing trends at our institution over a 16-year period for femur fractures in pediatric patients. Our hypothesis was that inpatient postoperative narcotic dosing would decrease in the time after the POSNA survey compared to prior.
Materials and Methods
After obtaining IRB approval, we queried the pediatric trauma database at a level I pediatric trauma center for all femur fractures from 01/01/2003 (when the database was created) to 12/31/2019 (when this study was initiated). Patients under the age of 16 years old with an injury severity score of 9 and no additional injuries (isolated traumatic diaphyseal femur fractures only) who were prescribed post-procedural (surgery or closed reduction) narcotics were selected for this retrospective study. Patients who had underlying disease processes such as neuromuscular diseases or syndromic conditions were excluded as were those with pathologic fractures. A total of 128 patients met inclusion criteria.
The electronic medical record was used to retrospectively collect data on patient demographics, injury and surgical characteristics, and narcotic prescriptions during hospitalization. Opioid doses were calculated in morphine milligram equivalents (MME) using standard conversions.
Statistical analyses were completed using R Statistical Software (Foundation for Statistical Computing, Vienna, Austria). Univariate analyses were conducted using the non-parametric tests Wilcoxon rank sum and Fisher’s exact test. Segmented linear regression analysis with a t-test was used to determine both the univariate and multivariate association between timing of the POSNA survey (01/01/2016 or earlier versus 01/02/2016 or later) and changes in postoperative opioid MME prescribed.
Results
Patient and Surgical Characteristics (Table 1)
Table 1. Patient and Surgical Characteristics
| Variable N (%) | Overall N = 128 (100.0) | Pre-POSNA N = 85 (66.4) | Post-POSNA 43 (33.6) | P-value |
|---|---|---|---|---|
| Patient Demographics | ||||
| Age (years)1 | 8.1 (2.9-11.6) | 9.0 (4.6-12.4) | 3.7 (2.3-10.4) | 0.0381 |
| Age categorical (years) | ||||
| <4 | 42 (32.8) | 19 (22.4) | 23 (53.5) | 0.0035 |
| 4-9 | 36 (28.1) | 29 (34.1) | 7 (16.3) | |
| 10-13 | 35 (27.3) | 28 (32.9) | 7 (16.3) | |
| 14+ | 15 (11.7) | 9 (10.6) | 6 (14) | |
| Sex | ||||
| Female | 34 (26.6) | 21 (24.7) | 13 (30.2) | 0.5300 |
| Male | 94 (73.4) | 64 (75.3) | 30 (69.8) | |
| Surgical Characteristics | ||||
| Reduction type | ||||
| No incision (closed reduction) | 49 (38.3) | 24 (28.2) | 25 (58.1) | 0.0019 |
| Incision (open reduction, hardware placed) | 79 (61.7) | 61 (71.8) | 18 (41.9) | |
| Flexible intramedullary nail | 39 (49.4) | 30 (49.2) | 9 (50.0) | |
| Rigid intramedullary nail | 14 (17.7) | 9 (14.8) | 5 (27.8) | |
| Submuscular plate | 25 (31.6) | 21 (34.4) | 4 (22.2) | |
| External fixation | 1 (1.3) | 1 (1.6) | 0 (0) | |
| Hospital length of stay (days)1 | 2 (1-3) | 2 (2-3) | 1 (1-2) | <0.0001 |
1Median(IQR)
Of the 128 patients, 85 (66.4%) were treated before distribution of the POSNA survey (pre-POSNA) and 43 (33.6%) were treated after the survey (post-POSNA). The median age of all patients was 8.1 years (interquartile range (IQR) 2.9-11.6). Those in the post-POSNA cohort were significantly younger than those before the survey (3.7 years vs. 9.0 years, P = 0.0381). The majority of patients in this study were male (N = 94, 73.4%), with no significant differences in sex between the two groups (pre-POSNA 75.3% male vs. pre-POSNA 69.8% male, P = 0.5300).
Most patients (N = 79, 61.7%) underwent an open reduction of their femur fracture (“open” is defined in this study as a procedure requiring an incision) with significantly more performed in the pre-POSNA group (71.8% vs. 41.9%, P = 0.0019). The median hospital length of stay was 2 days (IQR 1-3) for the overall cohort and was significantly shorter in the post-POSNA group (1 day) than the pre-POSNA group (2 days; P < 0.0001).
Postoperative Opioid Prescription Characteristics (Table 2, Figures 1 and 2)
Table 2. Postop Opioid MME Prescription Characteristics
| Variable | Overall | Pre-POSNA | Post-POSNA | P-value |
|---|---|---|---|---|
| Total postop hospital MME1 | 27.2 (9.9-61.8) | 28.4 (9.3-75.5) | 24.4 (12.6-48.6) | 0.3828 |
| Maximum MME | 504.3 | 504.3 | 234.4 | |
| Daily postop hospital MME1 | 14.7 (5.4-25.3) | 11.8 (4.3-25.8) | 17.5 (11.2-23.3) | 0.2036 |
| Maximum MME | 106.5 | 106.5 | 73.6 |
1Median(IQR)
Figure 1. Total postop hospital opioid MEE prescription doses for all patients with overlay of median doses by year.
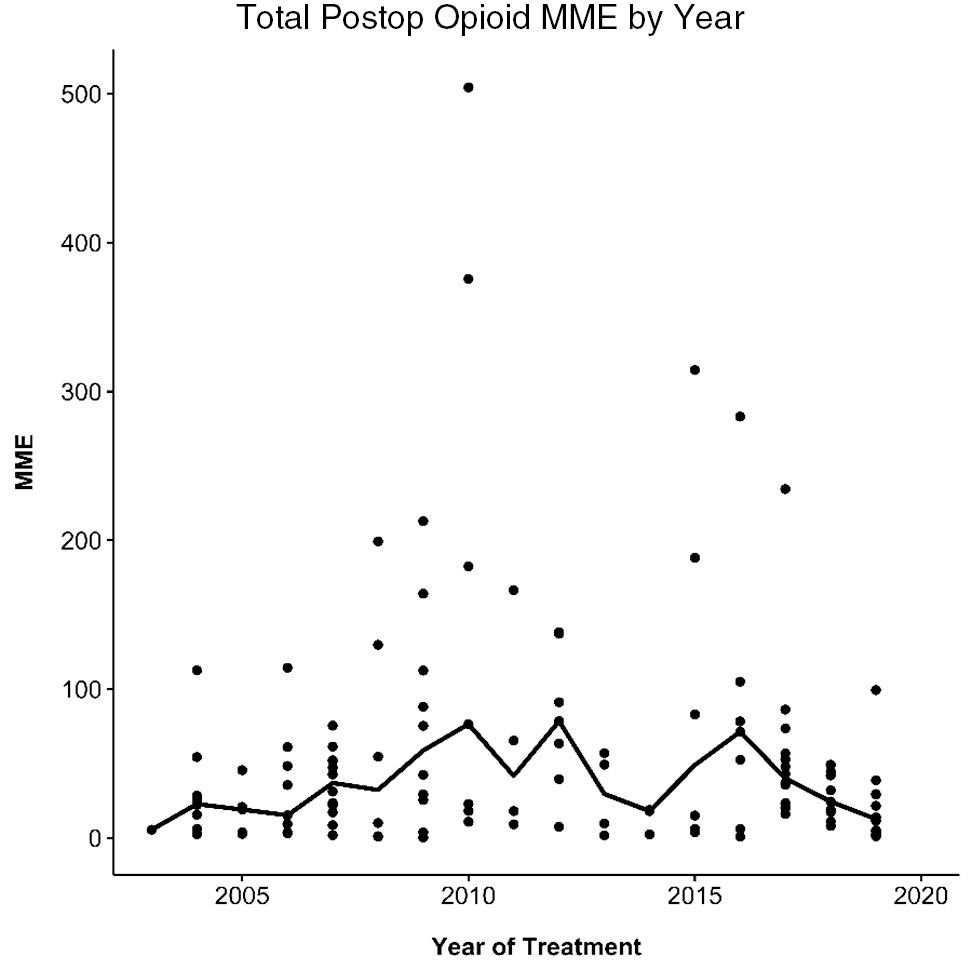
Figure 2. Average daily postop hospital MME prescription doses with overlay of median daily doses by year.
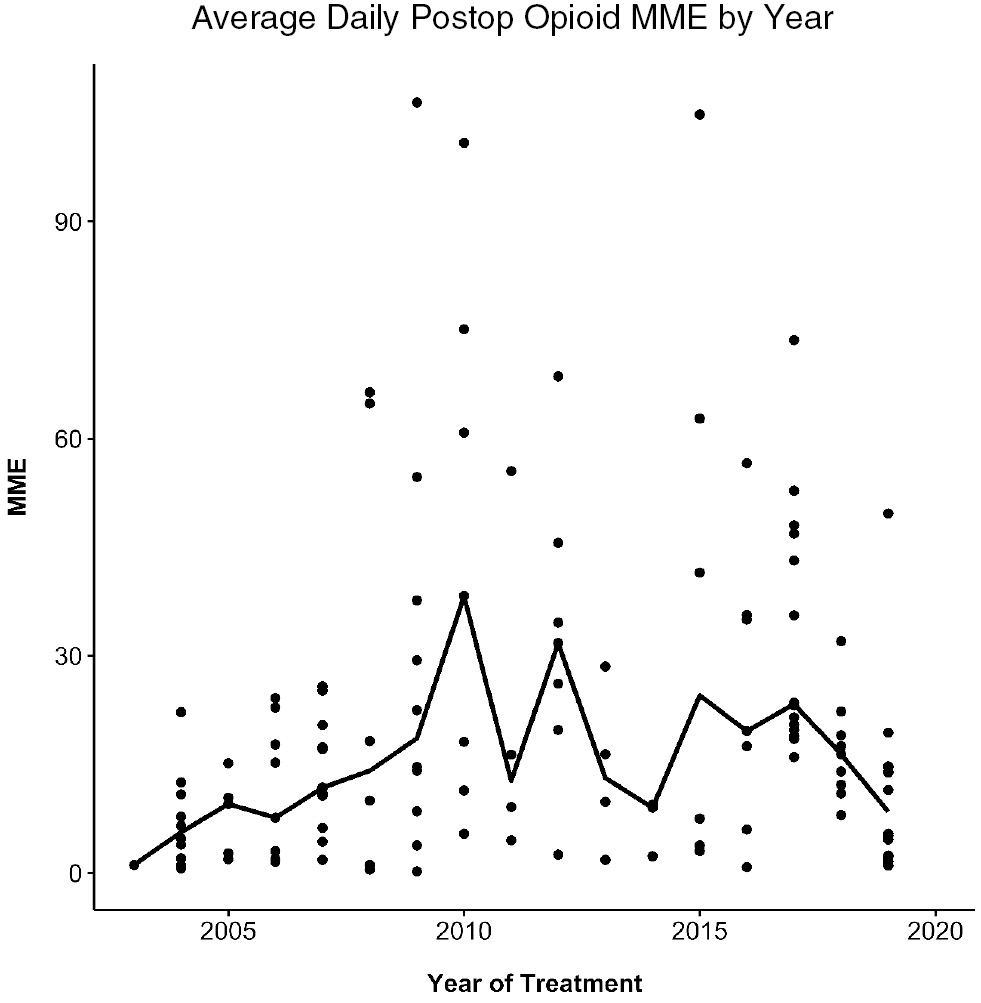
The median total postoperative hospital MME prescribed for the entire cohort was 27.2 (IQR 9.9-61.8) and the median daily postoperative hospital MME prescribed was 14.7 (IQR 5.4-25.3). The total MME prescribed was similar for both the pre-POSNA group (28.4) and the post-POSNA group (24.4, P = 0.3828) as well as for the daily MME prescribed (pre-POSNA 11.8, post-POSNA 17.5, P = 0.2036).
Unadjusted Segmented Linear Regression (Table 3)
Table 3. Unadjusted Segmented Regression Model Coefficients
| Variable | Estimate | Standard Error | T-value | P-value |
|---|---|---|---|---|
| Intercept | 24.340 | 14.751 | 1.650 | 0.1015 |
| Time overall | 7.173 | 2.334 | 3.074 | 0.0026 |
| Post-POSNA (yes) | −44.969 | 30.561 | −1.471 | 0.1437 |
| Time after POSNA | −20.199 | 10.323 | −1.957 | 0.0526 |
An unadjusted segmented linear regression model of total postoperative hospital opioid MME per patient by year of treatment was comprised of two time segments: 1/01/2016 (year of administration of the POSNA survey) or earlier and 1/02/2016 or after. In Table 3 are the parameters of the predictor variables and the intercept of the unadjusted model. The variable of interest—the time period after the POSNA survey (time after POSNA)—represents an associated decrease in 20.2 morphine milligram equivalents for each later year of fracture treatment, although this finding is not significant (P = 0.0526).
Adjusted Segmented Linear Regression (Tables 4–8, Figures 3 and 4)
Tables 4–7. Segmented Regression Model Coefficients Adjusting for Hospital Length of Stay, Procedural Incision, and Patient Age
| Variable | Estimate | Standard Error | T-value | P-value |
|---|---|---|---|---|
| Intercept | −99.958 | 18.947 | −5.276 | <0.0001 |
| Time overall | 10.944 | 1.963 | 5.576 | <0.0001 |
| Post-POSNA (yes) | −58.029 | 25.129 | −2309 | 0.0226 |
| Time after POSNA | −17.946 | 8.233 | −2.180 | 0.0312 |
| Length of stay | 23.124 | 4.938 | 4.683 | <0.0001 |
| Incision (yes) | −55.706 | 22.521 | −2.474 | 0.0148 |
| Age | 9.740 | 2.137 | 4.577 | <0.0001 |
| Variable | Estimate | Standard Error | T-value | P-value |
|---|---|---|---|---|
| Intercept | −69.563 | 19.298 | −3.605 | 0.0005 |
| Time overall | 10.261 | 2.077 | 4.940 | <0.0001 |
| Post-POSNA (yes) | −48.603 | 26.485 | −1.835 | 0.0689 |
| Time after POSNA | −17.894 | 8.951 | −1.999 | 0.0478 |
| Length of stay | 28.363 | 4.367 | 6.494 | <0.0001 |
| Variable | Estimate | Standard Error | T-value | P-value |
|---|---|---|---|---|
| Intercept | −69.657 | 19.125 | −3.642 | 0.0004 |
| Time overall | 9.596 | 2.092 | 4.588 | <0.0001 |
| Post-POSNA (yes) | −39.394 | 26.731 | −1.477 | 0.1421 |
| Time after POSNA | −18.351 | 8.875 | −2.068 | 0.0408 |
| Length of stay | 22.789 | 5.322 | 4.282 | 0.0744 |
| Incision (yes) | 26.279 | 14.604 | 1.799 | <0.0001 |
| Variable | Estimate | Standard Error | T-value | P-value |
|---|---|---|---|---|
| Intercept | −86.892 | 18.573 | −4.678 | <0.0001 |
| Time overall | 9.849 | 1.952 | 5.046 | <0.0001 |
| Post-POSNA (yes) | −43.006 | 24.890 | −1.728 | 0.0865 |
| Time after POSNA | −18.472 | 8.401 | −2.199 | 0.0298 |
| Length of stay | 18.703 | 4.699 | 3.980 | 0.0001 |
| Age | 5.517 | 1.312 | 4.204 | <0.0001 |
Due to concerns about multicollinearity between patient age and procedural incision, we generated multiple linear regression models that adjusted for patient age and procedural incision separately to determine the impact these variables had on the variable of interest, time after POSNA. To act as a reference, a model that included hospital length of stay was created (Table 5). The time after POSNA coefficient was −17.894, a decrease in magnitude from −20.199 in the unadjusted model but still significantly associated with a change in opioid MME (P = 0.0478). The next model adjusted for both length of stay and procedural incision (Table 6). The time after POSNA coefficient changed to −18.351 (P = 0.0408). In the final model (Table 7), length of stay and patient age were adjusted for, with the coefficient of interest = −18.472 MME/year (P = 0.0298).
Table 8. Variable Inflation Factor Values for Each Coefficient in the Segmented Regression Model
| Variable | VIF |
|---|---|
| Time overall | 3.8237 |
| Post-POSNA (yes) | 5.3661 |
| Time after POSNA | 3.8961 |
| Length of stay | 1.8304 |
| Incision (yes) | 4.5648 |
| Age | 3.7939 |
Figure 3. Jitterplot of patient age by procedural incision.
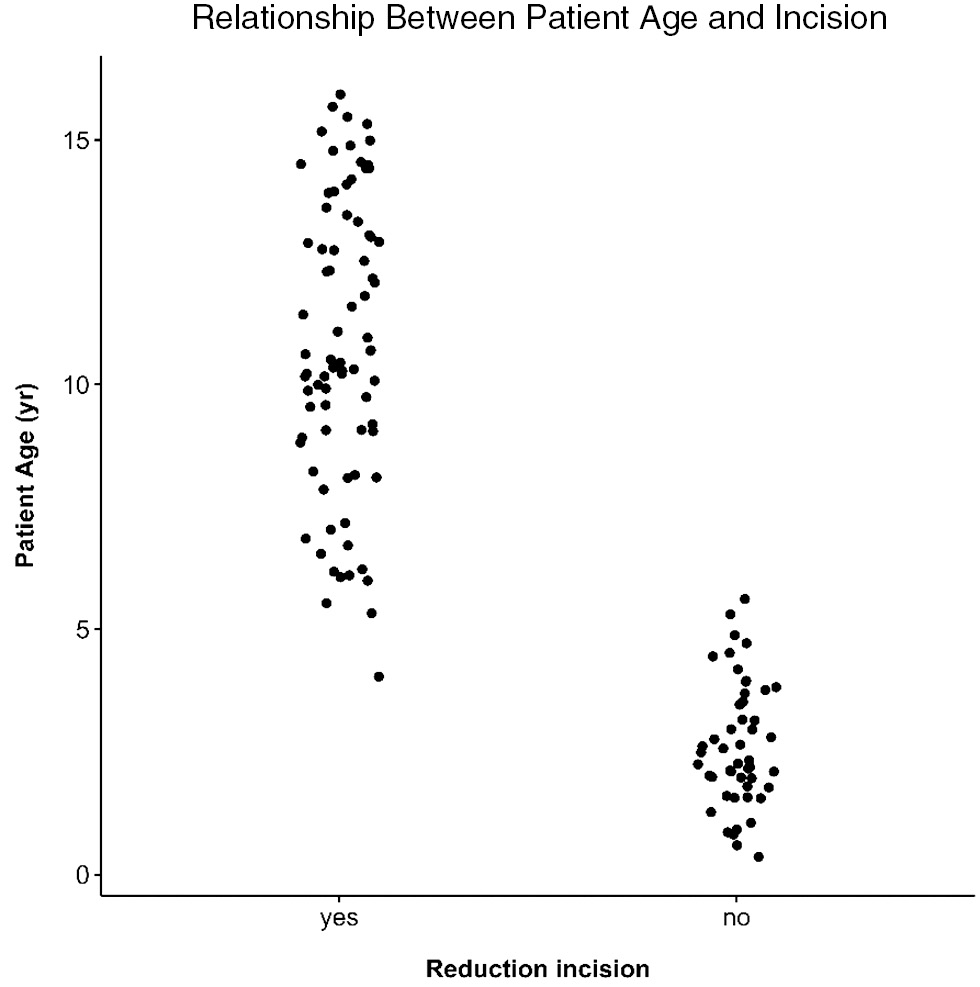
Figure 4. Segmented regression of pre- and post-POSNA survey total postop hospital opioid MMEs adjusted for length of stay and procedural incision.
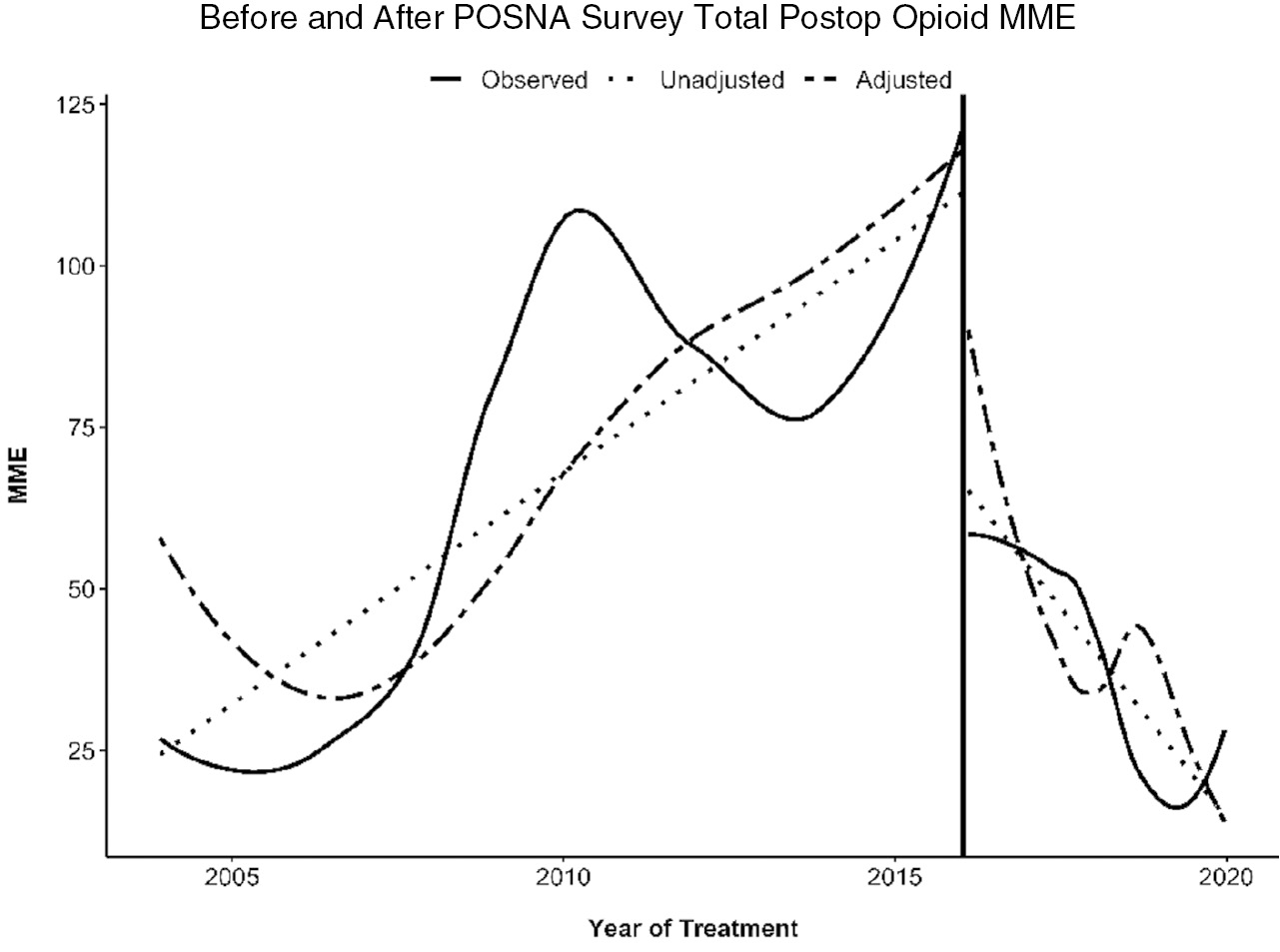
To build the adjusted segmented linear regression model of total postoperative hospital opioid MME by year of treatment, predictor variables that were significantly different between the two comparison groups were adjusted for patient age, procedural incision, and hospital length of stay. The parameters of this fully adjusted model are summarized in Table 4. Time after the POSNA survey in this model was significantly associated with −18.351 opioid MME per year (P = 0.0408).
To better visualize the relationship between the two predictor variables and potential multicollinearity, a jitterplot of patient age by procedural incision was generated (Figure 3). The jitterplot shows near-complete delineation between patient age and procedural incision, with almost all patients 5 years of age or younger undergoing closed reduction with no incision.
Finally, the variable inflation factor (VIF), which is a measure of how well variables correlate with others in the model, was calculated (Table 8). The patient age VIF was 3.7939 and the procedural incision VIF was 4.5648, showing moderate correlation between the two coefficients.
Due to evidence of multicollinearity between patient age and procedural incision, a segmented regression model that adjusts for hospital length of stay and procedural incision was chosen as the final model for analyses (Figure 4).
Discussion
In response to the worsening opioid epidemic, multiple national guidelines for pain control have been introduced.12,13 However, these guidelines do not address narcotic prescriptions in the pediatric population and they lack injury-specific considerations.8 Several studies have shown that medical use of opioids is associated with up to a 33% increased risk of future persistent use and development of abuse in adolescents.7,14,15
In 2016, the Pediatric Orthopaedic Society of North American conducted a survey asking surgeons across the United States how they would manage pain in seven common scenarios. Seventy five percent of respondents reported making pain management decisions, yet there were no guidelines or studies cited for how narcotic dosing was determined—only anecdotal experience. Additionally, the amount of time for which opioid medications were prescribed varied widely, even up to 4 weeks following minor procedures. The majority of respondents (58%) admitted to providing prophylactic opioid prescriptions in case patients ran out and were not able to be seen by the same provider due to time or distance constraints.10 Based on these findings, POSNA recently released recommendations for postoperative pain management.11 The recommendations include initial and secondary scripts for narcotics and length of time as well as maximum number of tablets or liquid formulation that should be prescribed in each prescription based on procedure. However, these guidelines are meant to act as a template for which individual institutions could develop their own opioid prescribing practices. Although the authors cite a 50% reduction in the amount of opioids prescribed, they still do not account for injury-specific considerations nor do they cite any studies upon which they based their opioid dosing.
In the current study, we retrospectively compared two groups: before the POSNA survey (pre-POSNA), and after the POSNA survey (post-POSNA). We did not find significant differences in the total (P = 0.3828) or daily (P = 0.2036) postoperative opioid MME prescribed on univariate analysis. However, our pre- and post-POSNA groups differed in certain patient and surgical factors that may clinically impact narcotic prescribing; the pre-POSNA group was significantly older than the post-POSNA group (9.0 vs. 3.7 years, P = 0.0381), and the pre-POSNA group underwent significantly more open (and incisional) reductions of their femur fractures (61.7% vs. 41.9%, P = 0.0019). Additionally, patients in the pre-POSNA group stayed in the hospital longer than those in the post-POSNA group (2 vs. 1 day, P < 0.0001).
While this study cannot directly answer why there were significantly younger patients in the post-POSNA group, one reason may be changes in practice at our institution. These include the increasing size of the pediatric orthopaedic division (from two surgeons in 2005 to four surgeons) and becoming a busier center following level I trauma designation in 2009. Coupled with national trends of pediatric orthopaedic trauma being increasingly treated at designated pediatric hospitals,14–16 the influx of young patients would be expected to impact the overall cohort demographics. The cause for the significant decline in hospital length of stay is likely multifactorial; improved treatment modalities and comfort with managing children on an outpatient basis as well as concern for increased cost for both patient families and the institution with longer stays.
Given that patient age strongly influences pediatric diaphyseal femur fracture treatment,17,18 (i.e., closed vs. open treatment), there was concern for multicollinearity between variables. This would cause the adjusted model to overly account for the same opioid MME predictor data. The jitterplot (Figure 3) showed near complete delineation between patient age and procedural incision, which correlates with our clinical concern that both variables account for much of the same opioid prescriptions and that only one should be included in the adjusted model. This is supported by the variable inflation factor for both coefficients which showed moderate correlation (Table 8 - age VIF = 3.7939, procedural incision VIF = 4.5648).
Finally, we tested for multicollinearity by generating two segmented regression models—one adjusting for hospital length of stay and patient age and the other adjusting for hospital length of stay and procedural incision. After adjusting for length of stay only, 17.894 less opioids MMEs were prescribed per year of treatment after POSNA. Adjusting for patient age caused a slight change in the magnitude of the coefficient to −18.472 as did procedural incision (−18.351). Both models showed little change in the predictor variable of interest. Because our practice considers procedural incision to be a greater clinical predictor of opioid dosing, we chose the model which adjusts for both hospital length of stay and procedural incision for our final analyses.
Our present study on postoperative prescriptions for femur fractures in children has many strengths. By choosing to focus on isolated diaphyseal femur fractures, we examined a focused patient cohort to identify injury-specific opioid prescription patterns. Most studies have focused on pediatric orthopaedic trauma, common or major orthopaedic procedures, or pediatric surgical patients in general. However, femur fractures are recognized to be the most painful fracture location9 and thus warrant injury and treatment-specific pain management.8 Another strength is the study length (16 years) which provides long-term trends on opioid prescribing patterns that encompass almost the entirety of the opioid epidemic: from the early stages when pediatric opioid prescriptions reached a peak plateau to more recently when increasing awareness and guidelines have shown a decline in prescriptions.19 Also, by studying opioid prescriptions at a single institution, there are relatively consistent fracture treatment and opioid prescription patterns across surgeons.
There are also limitations of this study. Because we chose to focus on isolated diaphyseal femur fractures, we have a small overall cohort size. Because of this, we were not able to conduct meaningful age-specific analyses based on best-practice recommendations for specific surgical procedures. Additionally, the use of a single institution does not provide insight into trends across the United States, so our results may be of limited generalizability. Our study also does not consider alternative pain management modalities including NSAIDs, muscle relaxants, and other analgesics. It must also be noted that national trends in the treatment of femoral diaphyseal fractures have shifted over the study period with increasing use of rigid locked intramedullary nails in those younger than 11 years and an overall increase in surgery for those under the age of 5.20 At our institution, however, the use of flexible intramedullary nails remained constant, whereas the rate of submuscular plating decreased (34.4% to 22.2%) and rigid nailing increased (14.8% to 27.8%) between the cohorts. While the specific surgical procedure could theoretically impact postoperative pain, this has not been reported in the acute perioperative period.21 Our institution utilizes similar narcotic prescribing patterns regardless of specific surgical procedure, which we expect to minimize differences in post-procedure MME prescribed. Finally, using the POSNA survey as our breakpoint for changes in opioid prescriptions does not represent a true “intervention.” Although we cannot attribute the significant decline in postoperative prescriptions to the survey, it reflects an inflection point within the healthcare system regarding the recognized danger of opioids and need to reduce prescriptions. The decline is likely multifactorial given the influx of research suggesting negative outcomes and national announcements/guidelines in adults and increasing concern about the impact on the pediatric population.
This is the first study to provide postoperative narcotic prescribing trends in pediatric diaphyseal femur fractures. We showed that increasing patient age, hospital length of stay, and procedural incision are all significant predictors of higher opioid prescriptions, with procedural incision and length of stay being the most clinically impactful variables. Since 2016, there has been a significant decline in opioids prescribed, likely the result of increased awareness and concern for narcotic use in pediatric patients. Future studies that optimize opioid prescriptions for specific pediatric orthopaedic injuries and surgical procedures are warranted.
Disclaimer
This study was funded by CTSA Grant Number UL1 TR002377 from the National Center for Advancing Translational Sciences (NCATS), a component of the National Institutes of Health (NIH). Its contents are solely the responsibility of the authors and do not necessarily represent the official view of NIH. The authors report no conflicts of interest related to this manuscript.
References
- Manchikanti L, Singh A. Therapeutic opioids: a ten-year perspective on the complexities and complications of the escalating use, abuse, and nonmedical use of opioids. Pain Physician. 2008;11(2 Suppl):S63-S88.
- Wide-ranging online data for epidemiologic research (WONDER). CDC: National Center for Health Statistics; 2020. Available at: http://wonder.cdc.gov.
- Rudd RA, Aleshire N, Zibbell JE, et al. Increases in drug and opioid overdose deaths--United States, 2000-2014. MMWR Morb Mortal Wkly Rep. 2016;64(50-51):1378-1382.
- Fortuna RJ, Robbins BW, Caiola E, et al. Prescribing of controlled medications to adolescents and young adults in the United States. Pediatrics. 2010;126(6):1108-1116.
- Hudgins JD, Porter JJ, Monuteaux MC, et al. Prescription opioid use and misuse among adolescents and young adults in the United States: a national survey study. PLoS Med. 2019;16(11):e1002922.
- McCabe SE, West BT, Teter CJ, et al. Medical and nonmedical use of prescription opioids among high school seniors in the United States. Arch Pediatr Adolesc Med. 2012;166(9):797-802.
- Miech R, Johnston L, O’Malley PM, et al. Prescription opioids in adolescence and future opioid misuse. Pediatrics. 2015;136(5):e1169-1177.
- Iobst CA, Singh S, Yang JZ. Opioid prescription patterns for pediatric orthopaedic fracture patients. J Clin Orthop Trauma. 2020;11(2):286-290.
- Kane RL, Bershadsky B, Rockwood T, et al. Visual Analog Scale pain reporting was standardized. J Clin Epidemiol. 2005;58(6):618-623.
- Raney EM, van Bosse HJP, Shea KG, et al. Current state of the opioid epidemic as it pertains to pediatric orthopaedics from the advocacy committee of the Pediatric Orthopaedic Society of North America. J Pediatr Orthop. 2018;38(5):e238-e244.
- Pediatric Orthopedic Society of North America. Postop pain management prescription guidelines. 2019. Available at: https://posna.org/Physician-Education/QSVI/PostOp-Pain-Management-Prescription-Guidelines.
- Dowell D, Haegerich TM, Chou R. CDC guideline for prescribing opioids for chronic pain--United States, 2016. JAMA. 2016;315(15):1624-1645.
- Interagency Pain Research Coordinating Committee. National pain strategy: a comprehensive population health-level strategy for pain. Washington, DC: US Department of Health and Human Services, National Institutes of Health; 2016. Available at: https://www.iprcc.nih.gov/node/5/national-pain-strategy-report
- Holt JB, Glass NA, Bedard NA, et al. Emerging U.S. national trends in the treatment of pediatric supracondylar humeral fractures. J Bone Joint Surg Am. 2017;99(8):681-687.
- Salazar JH, Goldstein SD, Yang J, et al. Regionalization of pediatric surgery: trends already underway. Ann Surg. 2016;263(6):1062-1066.
- Sessions WC, Nickel AJ, Truong WH, et al. Regionalization of isolated pediatric femur fracture treatment: recent trends observed using the Kids’ inpatient database. J Pediatr Orthop. 2020;40:277-282.
- Jevsevar DS, Shea KG, Murray JN, et al. AAOS clinical practice guideline on the treatment of pediatric diaphyseal femur fractures. J Am Acad Orthop Surg. 2015;23(12):e101.
- Kocher MS, Sink EL, Blasier RD, et al. Treatment of pediatric diaphyseal femur fractures. J Am Acad Orthop Surg. 2009;17(11):718-725.
- McCabe SE, West BT, Veliz P, et al. Trends in medical and nonmedical use of prescription opioids among US adolescents: 1976-2015. Pediatrics. 2017;139(4).
- Hubbard EW, Riccio AI. Pediatric orthopedic trauma: an evidence-based approach. Orthop Clin North Am. 2018;49(2):195-210.
- Milligan D, Henderson L, Tucker A, et al. Elastic nail fixation versus plate fixation of paediatric femoral fractures in school age patients - a retrospective observational study. J Orthop. 2019;19:153-157.