
Original Research
Factors Associated with Presentation of Severe Adolescent Idiopathic Scoliosis
1Northwestern University Feinberg School of Medicine, Chicago, IL; 2Franciscan Physician Network Orthopedics & Podiatry, Olympia Fields, IL; 3Division of Orthopaedic Surgery and Sports Medicine, Ann & Robert H. Lurie Children’s Hospital of Chicago, IL
Correspondence: Jill E. Larson, MD, Division of Orthopaedic Surgery and Sports Medicine, Ann & Robert H. Lurie Children’s Hospital, 255 E. Chicago Ave., Box 69, Chicago, IL 60611. E-mail: [email protected]
Received: January 17, 2023; Accepted: June 22, 2023; Published: August 1, 2023
Volume 5, Number 3, August 2023
Abstract
Background: Adolescent idiopathic scoliosis (AIS) is a common referral to pediatric orthopaedic surgeons. Timely treatment with appropriate bracing decreases the risk of curve progression and need for surgical intervention. Despite pediatrician screening, patients still present to orthopaedic surgeons with curve magnitudes too large for nonoperative bracing to prevent progression to surgical curve magnitude. The aim of this study was to identify the sociodemographic differences between patients who are initially diagnosed with mild versus moderate/severe AIS.
Methods: This retrospective cross-sectional study included patients aged 10 to 18 years diagnosed with AIS between 2011-2021 at a major metropolitan tertiary care center. Scoliosis severity was classified based on initial radiographs. Sociodemographic factors were recorded including patient addresses, which were cross-referenced with the diversitydatakids.org Child Opportunity Index (COI) database, which analyzes the quality of resources in a geographic area.
Results: Gender, health insurance provider, race/ethnicity, and COI were all found to have a statistically significant relationship with Cobb angle (CA) and age at initial presentation. The odds of presenting with severe (versus mild and moderate) scoliosis were 2.3 times higher for patients who identified as Black/African American compared to those who identified as White. Additionally, the odds of initially presenting with severe scoliosis were almost 40% higher in females compared to males. Furthermore, each stepwise increase in COI was associated with a 17%-19% decrease in odds of presenting with severe scoliosis, depending on standardization.
Conclusions: There are sociodemographic disparities in the identification and initiation of treatment for AIS. Specifically, the odds of presenting with severe scoliosis are increased in patients who identify as Black/African American or female and/or come from areas with lower access to resources (as defined by COI). Appropriate and timely referral to a pediatric orthopaedic surgeon for AIS treatment thus requires 1) educating primary care providers, pediatricians, and scoliosis screeners on how to appropriately identify scoliosis and the risks associated with late identification/referral and 2) public health initiatives, such as universal school screenings or outreach mobile clinics, to address access to care for patients at risk for late scoliosis identification.
Level of Evidence: Level III (Retrospective cohort study)
Key Concepts
- At the time of diagnosis, a patient’s curve magnitude (calculated via Cobb angle) and future growth potential have significant implications in both curve progression and treatment planning.
- Avoiding spinal fusion by early curve identification and appropriate nonoperative (i.e., brace) treatment reduces patient risk and healthcare spending.
- There are sociodemographic disparities in the identification and initiation of treatment for adolescent idiopathic scoliosis.
- The odds of presenting with severe scoliosis are increased in patients who identify as Black/African American or female and/or come from areas with a lower access to resources (as defined by the Child Opportunity Index).
Introduction
Scoliosis is defined as coronal plane curvature of the spine greater than 10 degrees with accompanying vertebral rotation and can be classified by etiology and age of onset.1,2 Idiopathic scoliosis (IS) comprises roughly 80% of all scoliosis cases and is diagnosed when there is no clear anatomic anomaly or neurologic condition to explain curve etiology.2 Adolescent idiopathic scoliosis (AIS) presents between ages 10 to 18 years and makes up 85-90% of all IS cases, with an overall prevalence of 0.47-5.20%.3–5
At the time of AIS diagnosis, a patient’s curve magnitude, calculated via Cobb angle (CA), and future growth potential have significant implications in both curve progression and treatment planning (Figure 1).
Figure 1. Cobb angle calculation.
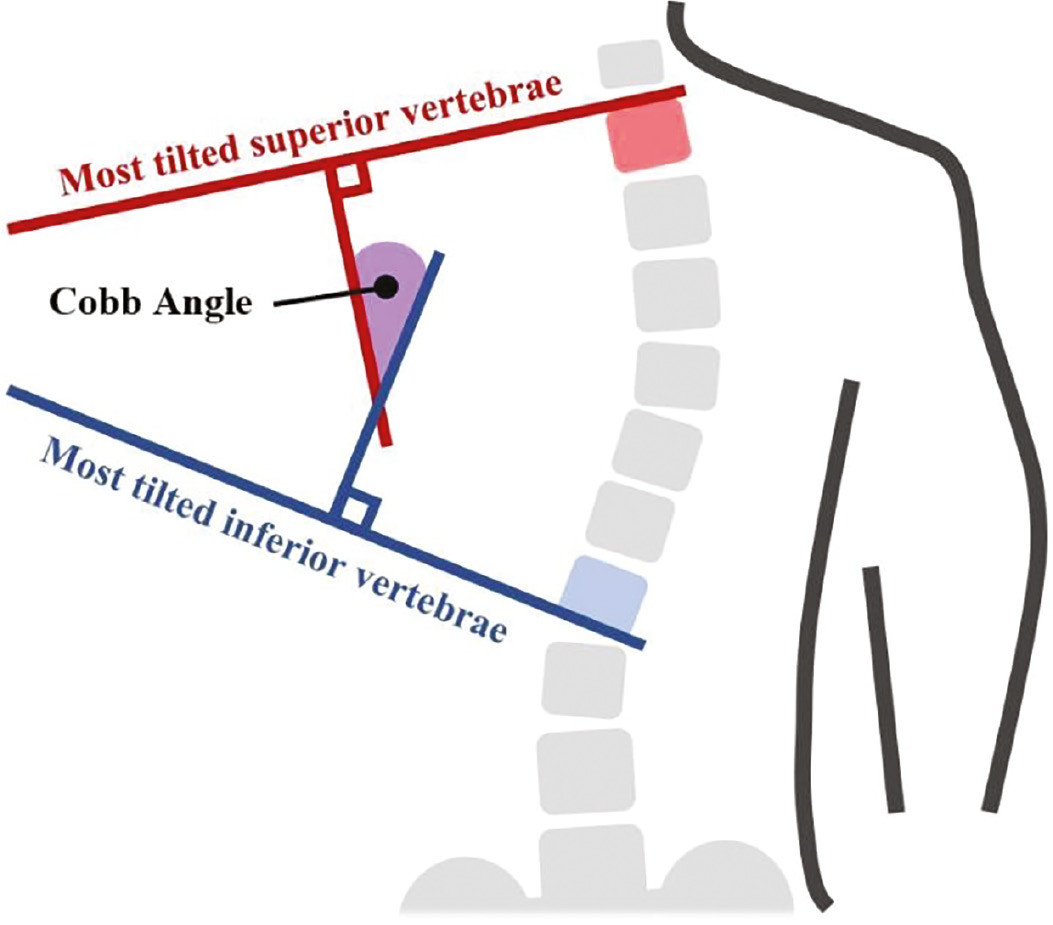
Specifically, a 25 degrees CA at initial presentation has been previously identified as an important threshold magnitude for long-term curve progression.6 Per the Scoliosis Research Society (SRS) guidelines, mild curves are monitored with serial imaging and generally do not require bracing or surgical intervention.7 When CA progresses past 25 degrees, a thoracic lumbar sacral orthosis (TLSO) brace may be indicated if Risser stage <3, which studies show can significantly slow mild to moderate curve progression and reduce the need for surgical intervention.1,7,8 Curves that progress beyond 40-50 degrees may require surgery to reduce current and future complications, as severe curves progress at approximately 1-2 degrees per year even after patients reach skeletal maturity.9–11 Moreover, studies demonstrate that bracing is unlikely to slow scoliosis progression in patients who initially present with severe curves, even when bracing is implemented as prescribed.12
Although spinal fusion surgery can maintain curve correction and prevent pain in patients with AIS, it comes with the inherent risks of surgery and specifically spinal fusion, including pseudoarthrosis and pulmonary, infectious, and neurologic complications (5%, 3.5%, 3-5%, and 1.5-1.75% incidence in the literature, respectively).11,13 Moreover, these surgeries can cost patients upwards of $200,000, and account for more than $1.1 billion annual collective healthcare spending in the United States alone.14–17 While the costs of TLSOs vary, even the most expensive (custom-made) braces typically cost less than $5,000, with lifetime costs of bracing treatment estimated to be less than $65,000, or roughly a third of the cost of surgery.18–20 Avoiding spinal fusion by early AIS identification and appropriate treatment with a TLSO brace is advantageous to both the patient and healthcare systems.
Family socioeconomic status (SES) and the environment in which a child is raised are also important contributors to adolescent health. Children in less-resourced neighborhoods have increased rates of injuries, malnutrition and associated comorbidities, and less access to healthcare resources, which can increase time to diagnoses and treatment.21,22 Consequently, we hypothesized that there are socioeconomic and demographic risk factors for delayed initial presentation to a pediatric orthopaedic surgeon for the treatment AIS. The aim of this study was to identify the sociodemographic differences between patients who are initially diagnosed with mild versus moderate/severe AIS.
Materials and Methods
This was a single-center, retrospective, cross-sectional study at a major metropolitan tertiary care center. The electronic medical records (EMR) of patients diagnosed with AIS between January 1st, 2011, and December 31st, 2021, at Ann & Robert Lurie Children’s Hospital of Chicago were examined with institutional review board approval (IRB 2021-4692). Patients were excluded if initial radiographs were unreadable or missing. Date of diagnosis was determined by date of ICD-9/10 code addition to the EMR, which could be added by any of the patient’s appropriately licensed providers (such as a pediatrician or primary care physician). Patients with documented comorbid congenital, neuromuscular, or musculoskeletal conditions that could classify their scoliosis as nonidiopathic were excluded as were those with missing sociodemographic data. Additionally, patients who received imaging more than 1 week after receiving an AIS diagnosis were excluded from this study to avoid systematically overestimating CA at initial presentation in certain groups. Evidence shows that untreated AIS can progress at a rate of over 1.3 degrees a month, and since patients with reduced access to healthcare are more likely to experience delays in receiving imaging, widening the cutoff window would likely increase the risk of inflating study results.23
The CAs used to evaluate scoliosis severity at initial presentation were obtained from interpretations of the earliest spinal imaging in the EMR. All interpretations were completed by a trained radiologist. Radiographic images that lacked interpretations in the EMR were read by a trained orthopaedic surgery resident. Curves were classified as mild (10°≤CA<25°), moderate (25°≤CA<40°), or severe (40°≥CA). CA less than 10 degrees are classified as spinal asymmetry, not scoliosis, and therefore were not included in this cohort.
In addition to CA, self-reported sociodemographic factors were recorded including patient date of birth, home address, race/ethnicity, sex, insurance provider, and preferred language. Aggregate “other” groups were created for both race/ethnicity and preferred language when sample sizes were too small for statistical analysis.
Addresses were geocoded and cross referenced with the database on diversitydatakids.org to assign a Child Opportunity Index (COI) score to each patient. COI is a validated, multidimensional, population-level surveillance tool that measures and maps the quality of resources and conditions for children in a geographic area.24,25 Overall, COI is a composite score based on the aggregate of the education, health and environment, and social and economic indices. Every index is rated on a scale of 0-100 and standardized to a local metropolitan (COI-M), state (COI-S), or national (COI-N) average. COI scores are classified categorically as very low, low, moderate, high, or very high, which each represent 20-point intervals on the numerical scale. COI-S was not used in this analysis because patients lived in different states and scores could not be standardized. Additionally, locations far from metropolitan areas do not have a COI-M score, thus the sample size for COI-N is greater than the COI-M in this study.
Odds ratios (OR) were calculated using the gologit2 statistical program, which fits partial proportional odds models for ordinal dependent variables.26 Because this program controls for all variables within the model, it enables calculation of ORs for each sociodemographic variable independent of the other variables’ possible confounding effects. Different ORs were therefore generated when using different COI standardizations. The significance for all analyses was set at p<0.05.
Results
The study cohort contained 2,413 patients and had a female:male ratio of 3:1 (Table 1).
Table 1. Summary of AIS Severity by Sociodemographic Factor
| Sociodemographic Factors | Scoliosis Severity | Totals | ||
|---|---|---|---|---|
| Mild (n=1259) | Moderate (n=649) | Severe (n=505) | ||
| Gender | ||||
| Female (n=1811) | 49.4% | 28.7% | 21.9% | 75.1% |
| Male (n=602) | 60.5% | 21.6% | 17.9% | 24.9% |
| Health Insurance Provider | ||||
| Private Insurance (n=1529) | 53.5% | 27.3% | 19.2% | 63.4% |
| Public Insurance (n=884) | 49.9% | 26.1% | 24.0% | 36.6% |
| Preferred Language | ||||
| English (n=2092) | 51.6% | 27.1% | 21.3% | 86.7% |
| Other (n=321) | 55.8% | 25.9% | 18.4% | 13.3% |
| Self-Reported Race/Ethnicity | ||||
| White (n=1295) | 55.2% | 27.5% | 17.3% | 53.7% |
| Hispanic/Latinx (n=625) | 56.0% | 24.5% | 19.5% | 25.9% |
| Black/African American (n=290) | 33.1% | 26.6% | 40.3% | 12.0% |
| Asian (n=121) | 50.4% | 32.2% | 17.4% | 5.0% |
| Other/2≤ Races (n=82) | 45.1% | 29.3% | 25.6% | 3.4% |
| COI (Nationally Standardized) | ||||
| Very Low (n=354) | 42.7% | 26.0% | 31.4% | 14.7% |
| Low (n=339) | 51.3% | 24.5% | 24.2% | 14.0% |
| Moderate (n=334) | 51.5% | 23.4% | 25.1% | 13.8% |
| High (n=521) | 50.9% | 28.4% | 20.7% | 21.6% |
| Very High (n=865) | 57.5% | 28.7% | 13.9% | 35.8% |
| 52.2% | 26.9% | 20.9% | n=2413 | |
| COI (Metro Standardized) | ||||
| Very Low (n=292) | 42.8% | 25.0% | 32.2% | 12.7% |
| Low (n=416) | 50.5% | 25.5% | 24.0% | 18.1% |
| Moderate (n=407) | 53.6% | 25.3% | 21.1% | 17.7% |
| High (n=473) | 52.0% | 29.0% | 19.0% | 20.6% |
| Very High (n=711) | 57.0% | 28.6% | 14.5% | 30.9% |
| 52.4% | 27.1% | 20.6% | n=2299 | |
Bold indicates summative total values.
Gender, health insurance provider, race/ethnicity, and COI-M/N were all found to have a statistically significant relationship with CA and age at initial presentation in patients with AIS (Table 2).
Table 2. Cobb Angle and Age at Initial Presentation by Sociodemographic Factor
| Sociodemographic Factors | Cobb Angle (°) (Avg ± SD) | p-value | Age (years) (Avg ± SD) | p-value |
|---|---|---|---|---|
| Curve Severity | ||||
| Mild | 13.4 ± 1.9 | |||
| Moderate | — | 13.6 ± 1.8 | p=0.083† | |
| Severe | 13.5 ± 1.9 | |||
| Gender | ||||
| Female | 28.7 ± 15.0 | p=0.009* | 13.2 ± 1.8 | p<0.001* |
| Male | 26.3 ± 16.4 | 14.3 ± 1.8 | ||
| Health Insurance Provider | ||||
| Private Insurance | 27.3 ± 14.6 | p=0.001* | 13.3 ± 1.8 | p=0.001* |
| Public Insurance | 29.5 ± 16.8 | 13.6 ± 1.9 | ||
| Preferred Language | ||||
| English | 28.4 ± 15.6 | p=0.052* | 13.4 ± 1.9 | p=0.077* |
| Other | 26.6 ± 14.3 | 13.6 ± 1.8 | ||
| Self-Identified Race/Ethnicity | ||||
| White | 26.6 ± 14.2 | 13.3 ± 1.8 | ||
| Asian | 27.0 ± 13.1 | 13.5 ± 1.9 | ||
| Hispanic/Latinx | 27.2 ± 14.6 | p<0.001† | 13.3 ± 1.9 | p=0.001† |
| Other/2≤ Races | 31.1 ± 18.5 | 13.6 ± 1.8 | ||
| Black/African American | 36.7 ± 19.3 | 13.8 ± 2.0 | ||
| COI (Metro Standardized) | ||||
| Very Low | 32.7 ± 19.1 | 13.8 ± 1.9 | ||
| Low | 29.3 ± 15.4 | 13.5 ± 1.9 | ||
| Moderate | 28.5 ± 15.9 | 13.5 ± 1.8 | ||
| High | 27.5 ± 14.5 | p<0.001† | 13.4 ± 1.8 | p=0.003† |
| Very High | 25.3 ± 12.7 | 13.3 ± 1.8 | ||
| COI (Nationally Standardized) | ||||
| Very Low | 32.6 ± 18.9 | 13.8 ± 1.9 | ||
| Low | 29.1 ± 15.1 | 13.5 ± 1.9 | ||
| Moderate | 29.9 ± 17.2 | p<0.001† | 13.4 ± 1.8 | p=0.007† |
| High | 28.3 ± 15.4 | 13.4 ± 1.8 | ||
| Very High | 25.2 ± 12.5 | 13.4 ± 1.8 |
†One-way ANOVA, *Unpaired T-test.
Bold indicates statistically significant values.
Specifically, the odds of presenting with severe versus mild and moderate scoliosis were 2.3 times higher for patients who identified as Black/African American compared to those who identified as White (Table 3).
Table 3. Odds Ratios of Presenting with Severe Versus Mild and Moderate AIS by Sociodemographic Factor
| Sociodemographic Factors | Metro Standardized | Nationally Standardized |
|---|---|---|
| Odds Ratio (95% CI) | Odds Ratio (95% CI) | |
| COI | 0.83 (0.76–0.91) | 0.81 (0.74–0.88) |
| Female: Male | 1.38 (1.08–1.77) | 1.36 (1.07–1.73) |
| Public Insurance: Private Insurance | 1.06 (0.73–1.21) | 1.04 (0.81–1.32) |
| Prefer English: Prefer Other Language | 1.28 (0.87–1.89) | 1.34 (0.92–1.95) |
| Hispanic/Latinx: White* | 0.93 (0.66–1.29) | 0.88 (0.63–1.21) |
| Black/African American: White | 2.34 (1.66–3.29) | 2.11 (1.51–2.95) |
| Asian: White | 1.04 (0.63–1.73) | 0.96 (0.58–1.58) |
| Other/2≤ Races: White | 1.49 (0.87–2.53) | 1.42 (0.84–2.41) |
*Largest “n” of race/ethnicities (white) selected for reference group.
Bold indicates statistical significance (p<.05).
Additionally, the odds of presenting with severe versus mild and moderate scoliosis was almost 40% higher in females compared to males. Each stepwise increase in COI-M and COI-N was associated with a 17% and 19% decrease in odds of presenting with severe versus mild and moderate scoliosis, respectively. While the magnitude of ORs varied slightly, there was no difference in statistical significance when using COI-M versus COI-N.
Scoliosis severity was not significantly associated with age at initial presentation. Additionally, a patient’s preferred language was not found to be significantly associated with age or CA at initial presentation. There was found to be a statistically significant association between self-reported race/ethnicity and COI-N/M, with over five times as many Black and Hispanic patients presenting from areas with a very low COI compared to White and Asian patients (Table 4).
Table 4. COI-N/M by Self-Identified Race/Ethnicity in Patients Presenting with AIS
| Self-Identified Race/Ethnicity | COI (Metro Standardized) | p-value | ||||
|---|---|---|---|---|---|---|
| Very Low | Low | Moderate | High | Very High | ||
| Asian | 4 | 15 | 20 | 32 | 47 | |
| Black/African American | 120 | 65 | 45 | 30 | 21 | |
| Hispanic/Latinx | 144 | 229 | 120 | 74 | 35 | p<.0001 |
| White | 15 | 94 | 207 | 317 | 583 | |
| Other/2≤ Races | 9 | 13 | 15 | 20 | 25 | |
| COI (Nationally Standardized) | ||||||
| Asian | 8 | 9 | 18 | 34 | 52 | |
| Black/African American | 131 | 55 | 37 | 40 | 27 | |
| Hispanic/Latinx | 182 | 182 | 123 | 86 | 52 | p<.0001 |
| White | 24 | 81 | 149 | 335 | 706 | |
| Other/2≤ Races | 9 | 12 | 7 | 26 | 28 | |
However, it is important to note that the gologit2 statistical program controls for this confounding effect in its analysis, thus the statistically significant ORs relating race/ethnicity to scoliosis severity are independent of COI’s effect, and vice versa.
Discussion
Previous literature has identified the impact of sociodemographic factors on scoliosis/CA and highlighted the relationship between COI and other pediatric pathologies; however, this study is the first to analyze the relationship between COI and scoliosis/CA at initial presentation.25,27,28 One possible explanation for why children from areas with a lower COI presented with more severe scoliosis is a decreased access to healthcare resources, which can increase time to diagnoses and treatment by a specialist like an orthopaedic surgeon.29 It is also possible that there are reduced screening rates in primary care clinics in lower versus higher COI areas, although this would require additional studies to further elucidate.
This study supports Zavatsky et al.’s results which found that African American patients are more likely to present with curves in the surgical curve magnitude range compared to their Caucasian counterparts.30 While causation cannot be determined from our data, one possible explanation for this discrepancy is decreased access to healthcare for African American patients compared to those of other races, which is further supported by the greater age of Black/African American patients at initial presentation.31 Moreover, evidence shows that African American girls enter pubertal development before Caucasian and Hispanic girls, which can further compound the effect of delayed presentation on increased scoliosis severity seen in African American patients.32
Patients with public health insurance were not found to have increased odds of presenting with severe scoliotic curves compared to patients with private health insurance. This aligns with the results reported by Russel, Zavatsky, and Goldstein et al. who found that publicly insured patients do not have significant clinical differences in CAs at initial presentation compared to privately insured patients.30,33,34 However, unlike Goldstein and Zavatsky, this study, along with Russell and Fletcher et al., identified a statistically significant difference in CA between the two groups.35 This difference can potentially be explained by the fact that children with public insurance have more limited access to both primary care or specialty (orthopaedic) care and thus increased times to diagnosis/referral compared to privately insured patients.36,37
Like many prior studies, our results demonstrate an AIS female to male prevalence ratio greater than 2:1.4,5 While it is still unknown why females have been found to be five times more likely to progress to a CA≥30°, this study found that females were more likely than males to initially present with severe scoliosis despite presenting at an earlier age, which may be a contributing factor.38,39 While most likely due to the natural history of pubertal growth spurts in females at a younger age than males, this study did not assess the stage of pubertal development or growth velocity metrics at presentation, so conclusions about causation cannot be drawn.
Despite the well-established risks and progression of AIS, the utility of screening continues to be debated. Since 1993, the U.S. Preventive Services Task Force (USPSTF) has adjusted its recommendation for routine AIS screening in asymptomatic adolescents three times, most recently to state there is insufficient evidence for or against it in 2018.40,41 One concern regarding screening is that over-referral is common, even when multiple diagnostic methods are used.42,43 Additionally, certain screening modalities, like the Adam’s forward-bending test, have been shown to have a low predictive value.44 Nevertheless, results from the Bracing in Adolescent Idiopathic Scoliosis Trial (BrAIST) showed that bracing significantly decreased progression of high-risk AIS curves to the surgery threshold for 72% of patients, which underscores the importance of early AIS identification and noninvasive treatment.45 To date, the American Academy of Orthopaedic Surgeons (AAOS), the Scoliosis Research Society (SRS), the Pediatric Orthopaedic Society of North America (POSNA), and the American Academy of Pediatrics (AAP) all recommend that females should be screened at ages 10 and 12 and boys at age 13 or 14.46 The results of this study provide a strong argument for targeted scoliosis screening in schools to reduce scoliosis severity at initial presentation, especially for adolescents from lower resourced areas (i.e., low COI).
A limitation of this cross-sectional study is a lack of longitudinal data, and thus an inability to correlate initial scoliosis severity with patient treatments or outcomes. Similarly, since any appropriately licensed care provider could first assign an AIS diagnosis to a patient, this study does not assess the time to evaluation by a specialist (orthopaedic surgeon) after AIS diagnosis by another care provider. To address these limitations, future prospective studies should examine the relationship between scoliosis severity at initial presentation and patient outcomes as well as sociodemographic factors and time from initial diagnosis/referral to specialist evaluation.
This study is also limited because it was conducted at a single center. Ann & Robert Lurie Children’s Hospital of Chicago is one of the largest children’s hospitals in its region, and the population of the surrounding city, while diverse, has one of the largest income wealth gaps in the U.S.47,48 Consequently, the results of this study may not be fully generalizable to other regions/institutions across the country.
Another limitation is that some patients received imaging at an outside hospital before being referred to our institution. To avoid systematically overcalculating the CA at initial consultation, viable outside radiographs uploaded to our institution’s EMR were used to determine initial CA. If no viable outside imaging from before the first visit was available, it was assumed that the radiographs taken at our institution were the first.
Finally, it is likely that the patients’ self-reported preferred language is an unreliable method for ascertaining potential language barriers in the healthcare setting, as the one-dimensional survey question does not address whether the patient was bilingual or to what extent they could speak and understand a language. Alternatively, providing adequate translation services in the hospital to facilitate care could explain why there was no significant difference in initial CA between patients who preferred speaking English and those who did not.
Conclusion
There are sociodemographic disparities in the identification and initiation of treatment for AIS. Specifically, the odds of presenting with severe scoliosis are increased in patients who identify as Black/African American, female, and/or come from areas with a lower access to resources (as defined by COI). Appropriate and timely referral to a pediatric orthopaedic surgeon for AIS treatment thus requires 1) educating primary care providers, pediatricians, and scoliosis screeners on how to appropriately identify scoliosis and the risks associated with late identification/referral and 2) public health initiatives, such as universal school screenings or outreach mobile clinics, to address access to care for patients at risk for late scoliosis identification, like those in geographic areas with low COI scores.
Additional Links
- POSNAcademy: Thoracoscopic Anterior Spinal Instrumentation and Fusion for Treatment of Adolescent Idiopathic Scoliosis
- POSNAcademy: Imaging of Pediatric Scoliosis
Disclaimer
No funding was received. The authors report no conflicts of interest related to this manuscript.
References
- Reamy BV, Slakey JB. Adolescent idiopathic scoliosis: review and current concepts. Am Fam Physician. 2001;64:111-116.
- Sung S, Chae HW, Lee HS, et al. Incidence and surgery rate of idiopathic scoliosis: a nationwide database study. Int J Environ Res Public Health. 2021;18:8152.
- Smith JR, Sciubba DM, Samdani AF. Scoliosis: a straightforward approach to diagnosis and management. JAAPA. 2008;21:40-45.
- Dunn J, Henrikson NB, Morrison CC, et al. Screening for adolescent idiopathic scoliosis: evidence report and systematic review for the US preventive services task force. JAMA. 2018;319:173-187.
- Konieczny MR, Senyurt H, Krauspe R. Epidemiology of adolescent idiopathic scoliosis. J Child Orthop. 2013;7:3-9.
- Tan KJ, Moe MM, Vaithinathan R, et al. Curve progression in idiopathic scoliosis: follow-up study to skeletal maturity. Spine (Phila Pa 1976). 2009;34:697-700.
- Richards BS, Bernstein RM, D’Amato CR, et al. Standardization of criteria for adolescent idiopathic scoliosis brace studies: SRS Committee on Bracing and Nonoperative Management. Spine (Phila Pa 1976). 2005;30:2068-2075.
- Kuznia AL, Hernandez AK, Lee LU. Adolescent idiopathic scoliosis: common questions and answers. Am Fam Physician. 2020;101:19-23.
- Weinstein SL, Ponseti IV. Curve progression in idiopathic scoliosis. J Bone Joint Surg Am. 1983;65:447-455.
- Weinstein SL, Zavala DC, Ponseti IV. Idiopathic scoliosis: long-term follow-up and prognosis in untreated patients. J Bone Joint Surg Am. 1981;63:702-712.
- Weiss HR, Goodall D. Rate of complications in scoliosis surgery - a systematic review of the Pub Med literature. Scoliosis. 2008;3:9.
- Hawary RE, Zaaroor-Regev D, Floman Y, et al. Brace treatment in adolescent idiopathic scoliosis: risk factors for failure-a literature review. Spine J. 2019;19:1917-1925.
- Coe JD, Arlet V, Donaldson W, et al. Complications in spinal fusion for adolescent idiopathic scoliosis in the new millennium. A report of the Scoliosis Research Society Morbidity and Mortality Committee. Spine (Phila Pa 1976). 2006;31:345-349.
- Shaw KA, Ange B, George V, et al. Continued increase in cost of care despite decrease in stay after posterior spinal fusion for adolescent idiopathic scoliosis. J Am Acad Orthop Surg Glob Res Rev. 2022;6:e21.00192.
- Vigneswaran HT, Grabel ZJ, Eberson CP, et al. Surgical treatment of adolescent idiopathic scoliosis in the United States from 1997 to 2012: an analysis of 20,346 patients. J Neurosurg Pediatr. 2015;16:322-328.
- Bozzio AE, Hu X, Lieberman IH. Cost and clinical outcome of adolescent idiopathic scoliosis surgeries-experience from a nonprofit community hospital. Int J Spine Surg. 2019;13:474-478.
- Raudenbush BL, Gurd DP, Goodwin RC, et al. Cost analysis of adolescent idiopathic scoliosis surgery: early discharge decreases hospital costs much less than intraoperative variables under the control of the surgeon. J Spine Surg. 2017;3:50-57.
- Ikwuezunma I, Wang K, Margalit A, et al. Cost-utility analysis comparing bracing versus observation for skeletally immature patients with thoracic scoliosis. Spine (Phila Pa 1976). 2021;46:1653-1659.
- Hanson G, Lyons KW, Fournier DA, et al. Reducing radiation and lowering costs with a standardized care pathway for nonoperative thoracolumbar fractures. Global Spine J. 2019;9:813-819.
- Roubal PJ, Freeman DC, Placzek JD. Costs and effectiveness of scoliosis screening. Physiotherapy. 1999;85:259-268.
- Sellström E, Bremberg S. The significance of neighbourhood context to child and adolescent health and well-being: a systematic review of multilevel studies. Scand J Public Health. 2006;34:544-554.
- Christian H, Zubrick SR, Foster S, et al. The influence of the neighborhood physical environment on early child health and development: a review and call for research. Health Place. 2015;33:25-36.
- Cheung JPY, Cheung PWH, Samartzis D, et al. Curve progression in adolescent idiopathic scoliosis does not match skeletal growth. Clin Orthop Relat Res. 2018;476:429-436.
- Child Opportunity Index (COI). [Diversitydatakids.org Website]. 2022. Available at: https://www.diversitydatakids.org/child-opportunity-index. Accessed June 8, 2022.
- Acevedo-Garcia D, McArdle N, Hardy EF, et al. The child opportunity index: improving collaboration between community development and public health. Health Aff (Millwood). 2014;33:1948-1957.
- Williams R. Understanding and interpreting generalized ordered logit models. J Math Sociol. 2016;40:7-20.
- Krager MK, Puls HT, Bettenhausen JL, et al. The child opportunity index 2.0 and hospitalizations for ambulatory care sensitive conditions. Pediatrics. 2021;148.
- Boozé ZL, Le H, Shelby M, et al. Socioeconomic and geographic disparities in pediatric scoliosis surgery. Spine Deform. 2022;10:1323-1329.
- Lueckmann SL, Hoebel J, Roick J, et al. Socioeconomic inequalities in primary-care and specialist physician visits: a systematic review. Int J Equity Health. 2021;20:58.
- Zavatsky JM, Peters AJ, Nahvi FA, et al. Disease severity and treatment in adolescent idiopathic scoliosis: the impact of race and economic status. Spine J. 2015;15:939-943.
- Manuel JI. Racial/Ethnic and gender disparities in health care use and access. Health Serv Res. 2018;53:1407-1429.
- Ramnitz MS, Lodish MB. Racial disparities in pubertal development. Semin Reprod Med. 2013;31:333-339.
- Russell T, Dharia A, Folsom R, et al. Healthcare disparities in adolescent idiopathic scoliosis: the impact of socioeconomic factors on Cobb angle. Spine Deform. 2020;8:605-611.
- Goldstein RY, Joiner ER, Skaggs DL. Insurance status does not predict curve magnitude in adolescent idiopathic scoliosis at first presentation to an orthopaedic surgeon. J Pediatr Orthop. 2015;35:39-42.
- Fletcher ND, Lazarus DE, Desai MJ, et al. Medicaid insurance is associated with larger curves in patients who require scoliosis surgery. Am J Orthop (Belle Mead NJ). 2015;44:E454-457.
- Skaggs DL, Clemens SM, Vitale MG, et al. Access to orthopedic care for children with medicaid versus private insurance in California. Pediatrics. 2001;107:1405-1408.
- Skaggs DL, Lehmann CL, Rice C, et al. Access to orthopaedic care for children with medicaid versus private insurance: results of a national survey. J Pediatr Orthop. 2006;26:400-404.
- Horne JP, Flannery R, Usman S. Adolescent idiopathic scoliosis: diagnosis and management. Am Fam Physician. 2014;89:193-198.
- Miller NH. Cause and natural history of adolescent idiopathic scoliosis. Orthop Clin North Am. 1999;30:343-352.
- US Preventive Services Task Force. Screening for adolescent idiopathic scoliosis. Policy statement. US Preventive Services Task Force. JAMA. 1993;269:2664-2666.
- Grossman DC, Curry SJ, Owens DK, et al. Screening for adolescent idiopathic scoliosis: US Preventive Services Task Force recommendation statement. JAMA. 2018;319:165-172.
- Yawn BP, Yawn RA, Hodge D, et al. A population-based study of school scoliosis screening. JAMA. 1999;282:1427-1432.
- Karachalios T, Sofianos J, Roidis N, et al. Ten-year follow-up evaluation of a school screening program for scoliosis. Is the forward-bending test an accurate diagnostic criterion for the screening of scoliosis? Spine (Phila Pa 1976). 1999;24:2318-2324.
- Fong DY, Lee CF, Cheung KM, et al. A meta-analysis of the clinical effectiveness of school scoliosis screening. Spine (Phila Pa 1976). 2010;35:1061-1071.
- Weinstein SL, Dolan LA, Wright JG, et al. Effects of bracing in adolescents with idiopathic scoliosis. N Engl J Med. 2013;369:1512-1521.
- Richards B, Vitale M. Screening for idiopathic scoliosis in adolescents. An information statement. J. Bone Jt Surg. 2008;90:195-198.
- Bach T. The 10 U.S. cities with the largest income inequality gaps. [U.S. News and World Report website]. September 21, 2020. Available at: https://www.usnews.com/news/cities/articles/2020-09-21/us-cities-with-the-biggest-income-inequality-gaps. Accessed May 2, 2023.
- McPhillips D. How racially and ethnically diverse is your city? [U.S. News and World Report website]. January 22, 2020. Available at: https://www.usnews.com/news/cities/articles/2020-01-22/measuring-racial-and-ethnic-diversity-in-americas-cities. Accessed May 2, 2023.