
Original Research
Variations in Duration of Clinical Follow-up After Spinal Fusion for Adolescent Idiopathic Scoliosis: A Survey of POSNA and SRS Membership
Department of Orthopaedic Surgery, Stanford University, Palo Alto, CA
Correspondence: John S. Vorhies, MD, Department of Pediatric Orthopaedic Surgery, 453 Quarry Rd., CAM Bldg., MC5658, Palo Alto, CA 94304. E-mail: [email protected]
Received: January 4, 2023; Accepted: May 19, 2023; Published: August 1, 2023
Volume 5, Number 3, August 2023
Abstract
Background: There are currently no evidence-based guidelines addressing the optimal duration of follow-up after posterior spinal fusion (PSF) for adolescent idiopathic scoliosis (AIS). Despite the safety and efficacy of PSF for AIS, long-term complications exist, including infection, pseudoarthrosis, adjacent segment disease, deformity progression, persistent pain, and junctional deformities. In this study, we describe practice variation existing among surgeons regarding duration and intervals of patient follow-up after surgical treatment of AIS in addition to factors influencing provider recommendations for duration of radiographic and clinical follow-up. This investigation of practice variation is important, as opportunities exist for both limiting unnecessary radiation exposure, while also identifying opportunities for timely intervention to help decrease the morbidity of late complications arising after spinal fusion.
Methods: An anonymous online survey was created and subsequently distributed to members of POSNA and SRS to assess practice demographics and surgeon opinions surrounding duration of surveillance following surgery for AIS. Only surgeons who treated at least five operative AIS cases within the past year were included. Descriptive statistics and comparative sub-analyses are presented.
Results: Forty-nine participants met inclusion criteria. Respondents were mainly pediatric orthopaedic surgeons (92%) in practice for 21-50 years (49%) who performed approximately 21-50 operative AIS cases per year (49%). Forty-eight percent of providers had an age limit in their practice, and 52% regularly followed operative AIS patients over 18 years of age. Sixty-two percent of surgeons followed operative AIS patients for 2-5 years postoperatively, whereas only 4% followed for more than 10 years. The most cited factors impacting follow-up recommendations were junctional deformities, adjacent segment disease, and symptomatic implants. There were no significant associations between years in practice, operative volume, and recommendations for duration of follow-up after routine operative AIS cases.
Conclusions: Significant variability in duration of follow-up after PSF for AIS exists. Although most patients are clinically followed for 2 years after surgery, only a small percentage of providers follow AIS patients for more than 10 years postoperatively. Numerous AIS revisions occur more than 5 years after the index surgery. Further investigations to determine the optimal duration of surveillance following PSF for AIS should be conducted.
Level of Evidence: V
Key Concepts
- Late complications following posterior spinal fusion (PSF) for adolescent idiopathic scoliosis (AIS) may occur 5-10 years after the index surgery and currently, there are no guidelines that outline the optimal duration of postoperative follow-up.
- Significant variability exists in pediatric orthopaedic provider recommendations for long-term follow-up after PSF for AIS and is not associated with surgeon experience or case volume.
- Most providers follow operative AIS patients for 1-2 years postoperatively, and only a small minority follow operative AIS patients for more than 10 years after the index surgery.
- Persistent back pain, junctional deformity, and symptomatic implants are the most common factors affecting provider recommendations for duration of follow-up.
- These survey findings may be useful for pediatric orthopaedic providers to operatively manage AIS patients in determining the need and frequency for routine radiographic and/or clinical follow-up.
Introduction
Posterior Spinal fusion (PSF) for adolescent idiopathic scoliosis (AIS) improves back pain, self-image, and health-related quality of life scores for patients with severe spinal deformity.1 Despite the safety and efficacy of PSF, a subset of patients will develop late-presenting complications including, but not limited to, degenerative disc disease (DDD), deformity progression, late infection, pain, pseudoarthrosis, and junctional kyphosis.3–13 The incidence and risk factors for these late complications are incompletely understood and as such, there are currently no evidence-based guidelines that address the optimal duration of follow-up after spinal fusion. A recent consensus paper argued that the optimal care of the postoperative AIS patient should include radiographs taken before discharge, and at 3, 12, and 24 months postoperatively.2 However, there is no reported consensus regarding if patients should be followed beyond this time frame, especially greater than 5-10 years following the index surgery.
Reported revision rates of instrumented PSF for AIS vary widely. Revision-free survivorship has been described to decline from index surgery with rates of 82-96% at 5 years, 77-92% at 10 years, and 87% at 15 years postoperatively.3,4,7 Though late complications and subsequent revisions for AIS continue to occur more than 5 years after spinal fusion for AIS, there is no established literature describing how surveillance may decrease morbidity. In the absence of evidence-based guidelines regarding optimal follow-up for operative AIS patients, the purpose of this study was to 1) describe current practice variation that exists among surgeons for duration of follow-up after surgical treatment of AIS and 2) identify what factors influence provider clinical decision-making about duration of follow-up after PSF for AIS.
Materials and Methods
After institutional review board approval, a survey was developed and approved by the Pediatric Orthopaedic Society of North America (POSNA) Evidence Based Practice Committee and the SRS leadership. It was simultaneously disseminated to all members of POSNA and SRS via email in accordance with the policies of those two organizations. There were no incentives for survey participation. The target study population included fellowship-trained orthopaedic surgeons who routinely manage AIS patients with spinal fusion. Respondents were first asked if they surgically treated at least five (5) patients diagnosed with AIS with spinal fusion using a predominantly pedicle screw-based construct within the past year. Those who answered “Yes” were invited to complete the remainder of the survey. If declined, the survey was automatically terminated. Respondents were then asked if they were active members of POSNA and SRS; providers that answered “No” were excluded from participating in the remainder of the survey. Responses were collected in Redcap database.
The anonymous online 10-minute survey consisted of 14 items, which included binary questions (yes/no), single and multiple choice (select all that apply) answers, and optional open text boxes. Provider demographic data such as fellowship training, years of experience, operative volume, and affiliation with a university health system and/or teaching hospital were collected. Follow-up preferences, including duration of follow-up, were collected. In addition, we asked each survey responder to provide a selection of clinical, radiographic, and/or patient factors that influenced the frequency and/or duration of follow-up after spinal fusion for AIS. The survey can be found in the supplemental data.
Data was collected and described qualitatively and quantitatively. Frequencies of provider demographics, clinical, or radiographic factors, were evaluated for associations with recommendations for duration of follow-up using Pearson χ2 analysis or Fisher exact test where appropriate. All statistical analyses were performed using commercially available software (RStudio version 1.1.456, Boston, MA), and the level of significance was set at p < 0.05.
Results
Provider Demographics
The survey was distributed to all POSNA and SRS members; 60 providers elected to participate in the survey, 48 met inclusion criteria. To prevent duplicate responses, respondents were asked to participate in the survey only once, both in the email correspondence which contained a link to the survey and in the survey instructions. Eleven participants were excluded from the study because they selected “No” to surgically treating at least five (5) AIS patients with a predominantly pedicle-based construct within the past year. One participant was excluded from the study, as they reported not being a member of POSNA or SRS. Most respondents were both SRS and POSNA members at 58%, whereas 29% were exclusively POSNA members and 13% were exclusively SRS members. 92% of respondents were fellowship-trained pediatric orthopaedic surgeons and the remaining 8% were fellowship-trained orthopaedic spine surgeons. There were no neurosurgeons that participated in this study. Regarding operative volume, 13% performed 5-10 operative AIS cases per year, 21% performed 11-20 cases per year, 44% performed 21-50 operative AIS cases per year, and lastly 23% reported performing more than 50 operative AIS cases per year (Figure 1). Fifty percent of providers reported a clinical experience of 21-50 years, whereas 27% reported 11-20 years of experience, and 23% reported 0-10 years of clinical experience (Figure 2). Most providers (83.3%) were associated with a university health system and/or teaching hospital.
Figure 1. Approximate total operative AIS cases per year reported by survey respondents.
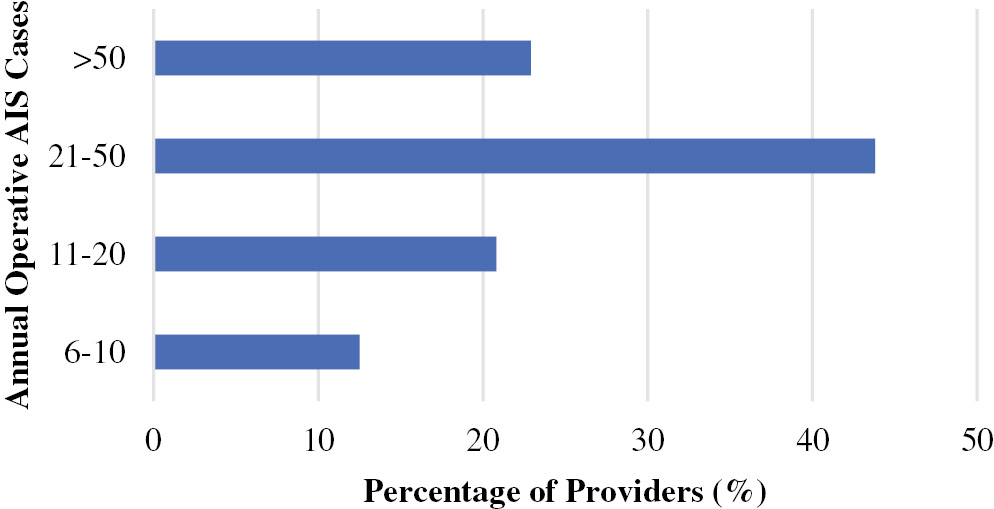
Figure 2. Clinical experience of survey respondents.

Duration and Frequency of Follow-up
Most providers at 62%, routinely followed AIS patients for 2-5 years postoperatively, 19% routinely followed for 1-2 years postoperatively, and 15% for 5-10 years. Only 4% reported following AIS patients routinely for more than 10 years postoperatively (Figure 3). A total of 52% of surgeons reported regularly treating patients over 18 years of age. Fifty-two percent did not have an age limit in their clinical practice, compared to 48% who reported an age limit. When assessing provider protocols for referring patients to an adult spine surgeon if patients ever aged out of their practice, 15% of providers reported officially referring asymptomatic patients to an adult spine surgeon, whereas 47% of surgeons reported that they only provide verbal recommendations for continued follow-up.
Figure 3. Provider preference for duration of follow-up following spinal fusion for AIS.

For asymptomatic AIS patients who were more than 5 years from the index surgery who were deemed to have an acceptable radiographic and clinical outcome at their most recent clinical visit, 40% of surgeons would recommend routine clinical and/or radiographic follow-up beyond 5 years compared to 56% who would not recommend additional follow-up. The remaining 4% of respondents reported that their recommendation for follow-up beyond 5 years, depends on 1) skeletal maturity and age of the patient and 2) the behavior of the compensatory curve and whether it was included in the fusion construct. There were no statistically significant associations between provider demographics and duration of follow-up and recommendation for duration of follow-up.
Factors Affecting Decision-Making
Factors affecting decision-making for frequency and duration of postoperative follow-up are detailed in Figure 4. The most common cited factors providers considered for determining duration and frequency of follow-up included persistent back pain (68% of respondents), junctional deformity (66%), symptomatic implants (61%), and infectious-related complications (49%). The least common cited factors were location of the upper instrumented vertebrae (10% of respondents) and patient activity level (15%). For the 10% (n=4) of providers that selected the “other” category, one provider mentioned “skeletal maturity” as an important factor in determining follow-up, and the remainder of providers reported they always follow patients into adulthood, and therefore, none of the listed factors impacted their decision-making for duration of follow-up. There was an association between provider experience and clinical factors affecting follow-up, as providers with more than 20 years in clinical practice were the least likely to select patient activity level (p=0.008) or fusion length (p=0.033) as being a factor in their clinical decision-making.
Figure 4. Factors affecting duration and frequency of follow-up after spinal fusion for AIS.

Of the eight providers who responded “Yes” to having specific indications for recommending long-term clinical follow-up postoperatively, all reported that subjective patient concerns and symptoms, such as persistent pain, infection, or noticeable deformity as influencing their decision-making with regards to duration of radiographic and/or clinical follow-up. When asked if providers have personally seen a post-operative complication arise in their practice 5-10 years following the index surgery, 21% (n=10) responded “Yes.” These specific complications listed included implant failure or broken implants (50% of responses), development of proximal and distal junctional deformity (40%), pseudoarthrosis (10%), progression of an unfused curve (10%), and disc herniation (10%).
Discussion
Revisions for AIS due to various postoperative complications can occur well beyond 2 years from the initial surgery with a significant number of reoperations occurring more than 5 years postoperatively.17–21,27 Despite the occurrence of late complications, data from a large prospective study group suggests that only 39% of patients are followed more than 5 years after the index surgery.3 In the survey we administered, while 40% of providers recommended routine postoperative follow-up after 5 years in a patient deemed to have an acceptable radiographic or clinical outcome, only 19% reported seeing operative AIS patients in their practice more than 5 years from the index surgery. In addition, for the providers who had specific indications for long-term clinical follow-up, these indications were all related to persistent symptoms or concerns in the symptomatic patient.
Reported revision rates following spinal fusion for AIS range from 5-20% and continue well after 5-10 years postoperatively.3–7 The indications for revision remain widespread with long-term studies documenting common etiologies such as pseudoarthrosis and implant failure (0.4%-17%), persistent back pain (0.8%-4.5%), infection (1.4%-9.1%), symptomatic implants (1.4-12%), and adjacent segment disease and deformity progression (0.5-7%).4,6–21 A large prospective study of AIS patients with a minimum 10-year follow-up documented a 10% complication and 6% reoperation rate with revisions occurring for infection, adjacent segment disease, and proximal junctional kyphosis throughout the entire 10-year period.22 The most common need for late revisions appears to be related to implant failure, pseudoarthrosis, junctional deformity, and late infection.3,26 This finding is partly reflected in our survey responses as implant failure and junctional deformity were the two most common complications cited in the 10% of providers who reported personally seeing complications arise 5-10 years postoperatively from the index surgery in operative AIS patients.
Even in the absence of revisions, the incidence of radiographic evidence consistent with adjacent segment disease has been documented to increase with increasing duration of follow-up. A retrospective cohort of AIS patients with a minimum of 5 years of follow-up demonstrated a 26% incidence of PJK at an average of 7 years postoperatively, and the proximal junctional angle in these patients progressively increased until the final year of follow-up.14 Furthermore, when assessing the prevalence of DDD, a recent cross-sectional study found 7% of operative AIS patients developed significant radiographic evidence of disc degeneration up to 10 years after surgery.15 Despite this, the benefit of surveillance to detect these findings has not been established. Although technological advances have resulted in overall decreased radiation exposure, the risks of long-term radiation and excessive costs to patients and their families to detect late radiographic changes with varying degrees of clinical significance, especially in the asymptomatic patient, are not negligible and likely influence both surgeon and patient preferences for routine radiographic follow-up postoperatively.
There is no clear evidence that early detection through surveillance could prevent morbidity associated with the later complications described in the literature. Some studies suggest that routine radiographic follow-up after 5 years offers little to no benefit in AIS patients who received PSF with third-generation implants, as continued surveillance may not ultimately affect revisions rates, quality of life scores, or changes in therapy.23,24 A large study of 265 patients treated with PSF for scoliosis found that postoperative radiography was rarely useful, with only 0.6% of postoperative radiographs demonstrating an implant-related complication, none of which occurred in asymptomatic patients.25 Similarly, Mens et al. argued that even routine 2-year radiographic follow-up added no value to the postoperative care of AIS patients, demonstrating in a cohort of 63 AIS patients that no significant changes to any radiographic parameters were observed from 1-2 years postoperatively.26 It should be noted that the focus of these papers was specifically on the utility of radiographic, not clinical follow-up. These reports emphasize radiographic findings significant enough to change management are exceedingly rare in the asymptomatic AIS patient.
A recent study in 80 operative AIS cases found that patients with late presenting complications needing reoperation between 2 and 5 years postoperatively presented during unplanned visits rather than routine follow-up appointments.23 This suggests that not only are symptomatic patients likely to present on an as-needed basis in the long term but patient-reported outcome measures (PROMs), a validated tool in surgically treated AIS patients, may be more useful for identifying patients at risk for reoperation. Ghandari et al. found a positive correlation between Oswestry Disability Index (ODI) scores and follow-up periods, indicating that patients with inferior scores tended to present in long-term follow-up settings more often compared to those with superior scores.15 Given this, perhaps collecting PROMs at follow-up intervals beyond 5-10 years may be helpful in identifying patients at risk for complications and could facilitate follow-up for those with clinical concerns who would otherwise not present without prompting.
Though the clinical benefits of and definitions of long-term follow-up are not clear, there is a consensus that long-term follow-up is critical in the research setting to establish the safety and efficacy of interventions for AIS. As such, the SRS requires at least 2 years of follow-up on clinical studies being submitted for presentation at its annual meeting and publication in its official journal.28 Given incidence of late complications and the rise in popularity of non-fusion treatments for scoliosis, 2-year follow-up may not be sufficient to adequately differentiate outcomes between novel and established interventions.
This study has several inherent limitations found in similar studies reporting survey results. Firstly, only a small percentage of members who received the survey fully completed it. This finding was not unexpected, although survey studies have become a popular design method of research over the last decade, response rates continue to downtrend possibly reflecting respondent fatigue.29 In addition, given inclusion criteria for the study was described in email correspondence during initial distribution of the survey, it is possible that responders self-excluded from participating in the survey preventing us from obtaining a more accurate response rate. Those who responded were disproportionately from academic practice settings and thus these results may not be representative of non-academic practice patterns. Lastly, because this study focused on recommendations for duration of follow-up given by surgeons who treat AIS, we did not include spine surgeons who exclusively treat adult patients. Completion of follow-up recommendations into adulthood may be largely dependent on patient decision-making and adult providers, neither of which were surveyed here. Despite these limitations, this is the first study that attempts to understand the practice pattern variation that exists among surgeons regarding long-term follow-up after spinal fusion for AIS.
Conclusion
In this survey study, we demonstrate that significant variability exists in recommendations for long-term follow-up after PSF for AIS and is not associated with surgeon experience or case volume. Although most patients are clinically followed up to 2 years postoperatively, only a small percentage of providers follow operative AIS patients for more than 5-10 years after the index surgery. To date, there are currently no evidence-based guidelines for optimal duration of follow-up and the benefit of long-term surveillance after spinal fusion for AIS is unclear. Given that late complications frequently arise more than 5 years after the index surgery, further investigation would be needed to establish the benefits of long-term radiographic surveillance following spinal fusion in operative AIS patients. In addition, given the hazards of long-term radiation exposure remain pertinent, further studies should also focus on the use of PROMs at 5- and 10-year intervals as a method of long-term surveillance to trigger clinical and if needed, radiographic follow-up for the symptomatic operative AIS patient.
Acknowledgement
Data access for this project was provided through a survey of POSNA and SRS membership. The content is solely the responsibility of the authors and does not necessarily represent the official views of POSNA or SRS.
Additional Links
- POSNAcademy: Posterior Spinal Instrumentation and Fusion for Treatment of Adolescent Idiopathic Scoliosis
- POSNA Position Statement on Screening for the Early Detection of Idiopathic Scoliosis in Adolescents
Disclaimer
Funding was received from the Scoliosis Research Society (SRS), Pediatric Orthopaedic Society of North America (POSNA), and Stanford University. The authors report no conflicts of interest related to this manuscript.
References
- Helenius L, Diarbakerli E, Grauers A, et al. Back pain and quality of life after surgical treatment for adolescent idiopathic scoliosis at 5-year follow-up: comparison with healthy controls and patients with untreated idiopathic scoliosis. J Bone Joint Surg Am. 2019;101(16):1460-1466.
- de Kleuver M, Lewis SJ, Germscheid NM, et al. Optimal surgical care for adolescent idiopathic scoliosis: an international consensus. Eur Spine J. 2014;23:2603-2618.
- Ahmed SI, Bastrom TP, Yaszay B, et al. 5-year reoperation risk and causes for revision after idiopathic scoliosis surgery. Spine (Phila Pa 1976). 2017;42(13):999-1005.
- Asher MA, Lai SM, Burton DC. Analysis of instrumentation/fusion survivorship without reoperation after primary posterior multiple anchor instrumentation and arthrodesis for idiopathic scoliosis. Spine J. 2010;10(1):5-15.
- Campos M, Dolan L, Weinstein S. Unanticipated revision surgery in adolescent idiopathic scoliosis. Spine (Phila Pa 1976). 2012;37(12):1048-1053.
- Ramo BA, Richards BS. Repeat surgical interventions following ‘‘definitive’’ instrumentation and fusion for idiopathic scoliosis. Spine (Phila Pa 1976). 2012;37:1211-1217.
- Bago J, Ramirez M, Pellise F, et al. Survivorship analysis of Cotrel-Dubousset instrumentation in idiopathic scoliosis. Eur Spine J. 2003;12:435-439.
- Westrick ER, Ward WT. Adolescent idiopathic scoliosis: 5-year to 20-year evidence-based surgical results. J Pediatr Orthop. 2011;31:S61-S68.
- Cook S, Asher M, Lai S-M, et al. Reoperation after primary posterior instrumentation and fusion for idiopathic scoliosis. Toward defining late operative site pain of unknown cause. Spine (Phila Pa 1976). 2000;25:463-468.
- Connolly P, Von Schroeder H, Johnson G, et al. Adolescent idiopathic scoliosis long-term effect of instrumentation extending to the lumbar spine. J Bone Joint Surg Am. 1995;77:1210-1216.
- Aurori B, Weierman R, Lowell H, et al. Pseudarthrosis after spinal fusion for scoliosis. Clin Orthop Rel Res. 1985;199:153-158.
- Dickson JH, Erwin WD, Rossi D. Harrington instrumentation and arthrodesis for idiopathic scoliosis. J Bone Joint Surg Am. 1990;72:678-683.
- Silvestre M, Bakaloudis G, Lolli F, et al. Late-developing infection following posterior fusion for adolescent idiopathic scoliosis. Eur Spine J. 2011;20:1-7.
- Kim YJ, Bridwell KH, Lenke LG, et al. Proximal junctional kyphosis in adolescent idiopathic scoliosis following segmental posterior spinal instrumentation and fusion: minimum 5-year follow-up. Spine (Phila Pa 1976). 2005;30:2045-2050.
- Ghandhari H, Ameri E, Nikouei F, et al. Long-term outcome of posterior spinal fusion for the correction of adolescent idiopathic scoliosis. Scoliosis Spinal Disord. 2018;13:14.
- Weiss H-R, Goodall D. Rate of complications in scoliosis surgery: a systematic review of the Pub Med literature. Scoliosis. 2008;3:9.
- Ho C, Sucato DJ, Richards BS. Risk factors for the development of delayed infections following posterior spinal fusion an instrumentation in adolescent idiopathic scoliosis patients. Spine (PhilaPa 1976). 2007;32:2272-2277.
- Richards BS, Hasley BP, Casey VF. Repeat surgical interventions following ‘‘definitive’’ instrumentation and fusion for idiopathic scoliosis. Spine (Phila Pa 1976). 2006;31:3018-3026.
- Kuklo TR, Potter BK, Lenke LG, et al. Surgical revision rates of hooks versus hybrid versus screws versus combined anteroposterior spinal fusion for adolescent idiopathic scoliosis. Spine (Phila Pa 1976). 2007;32:2258-2264.
- Mcmaster MJ. Luque rod instrumentation in the treatment of adolescent idiopathic scoliosis a comparative study with Harrington instrumentation. J Bone Joint Surg Br. 1991;73:982-989.
- Mielke CH, Lonstein JE, Denis F, et al. Surgical treatment of adolescent idiopathic scoliosis: a comparative analysis. J Bone Joint Surg Am. 1989;71:1170-1177.
- Hariharan AR, Shah SA, Petfield J, et al. Complications following surgical treatment of adolescent idiopathic scoliosis: a 10-year prospective follow-up study. Spine Deform. 2022;10(5):1097-1105.
- Mac-Thiong JM, Remondino R, Joncas J, et al. Long-term follow-up after surgical treatment of adolescent idiopathic scoliosis using high-density pedicle screw constructs: is 5-year routine visit required? Eur Spine J. 2019;28:1296-1300.
- Vila-Casademunt A, Pellisé F, Domingo-Sàbat M, et al. Is routine postoperative radiologic follow-up justified in adolescent idiopathic scoliosis? Spine Deform. 2013;1(3):223-228.
- Garcia GH, Park MJ, Baldwin K, et al. Do routine radiographs within the first two years following pediatric posterior spinal fusion prompt revision surgery? Spine (Phila Pa 1976). 2013;38(25):2216-2220.
- Mens RH, van Hooff ML, Geuze RE, et al. No added value of 2-year radiographic follow-up of fusion surgery for adolescent idiopathic scoliosis. Eur Spine J. 2021;30(3):759-767.
- Aghdasi B, Bachmann KR, Clark D, et al. Patient-reported outcomes following surgical intervention for adolescent idiopathic scoliosis: a systematic review and meta-analysis. Clin Spine Surg. 2020;33(1):24-34.
- Bettany-Saltikov J, Weiss HR, Chockalingam N, et al. A comparison of patient-reported outcome measures following different treatment approaches for adolescents with severe idiopathic scoliosis: a systematic review. Asian Spine J. 2016;10(6):1170-1194.
- Williams BA, Guerrero A, Blakemore LC, et al. Surveying the POSNA landscape: what can we learn from society survey studies? J Pediatr Orthop. 2020;40(1):e63-e67.