
Original Research
The Impact of Pelvic Osteotomies on Birth Canal Anatomy and Cesarean Section Rates: A Systematic Review
1Department of Orthopaedic Surgery, Hospital for Special Surgery, New York, NY; 2Division of Orthopaedics, Children’s Hospital of Philadelphia, Philadelphia, PA
Correspondence: Joshua T. Bram, MD, Department of Orthopaedic Surgery, Hospital for Special Surgery, 535 E 70th St., New York, NY. E-mail: [email protected]
Received: December 28, 2022; Accepted: March 7, 2023; Published: May 1, 2023
Volume 5, Number 2, May 2023
Abstract
Background: Various pelvic osteotomies can be performed to improve femoral head coverage for patients with hip dysplasia and other childhood hip disorders with the goal of delaying or preventing osteoarthritis. During preoperative discussions, female patients and their parents often ask about the influence of these osteotomies on future pregnancy. The literature on this topic is varied with no consensus on the appropriateness of elective cesarean section (C-section) for such patients. Therefore, this study sought to review and summarize the literature regarding the impact of different pelvic osteotomies on birth canal anatomy and C-section rates.
Methods: All studies assessing the impact of pelvic osteotomies on birth canal anatomy or pregnancy outcomes for patients were identified through a systematic search of four online databases (PubMed, Embase, CINAHL, and Cochrane Library). PRISMA guidelines were then used to evaluate all identified studies for appropriateness, leading to the final inclusion of 17 articles evaluating five general types of pelvic osteotomies.
Results: The Salter, double, and triple osteotomies were found to decrease the size of the pelvic outlet in model-based and radiographic studies. The Chiari osteotomy decreased the dimensions of the pelvic inlet/mid-pelvis and was associated with higher reported C-section rates. The Bernese periacetabular osteotomy was not associated with any changes in pelvic diameters, with reported increased rates of C-section noted to result from obstetrician preference. For osteotomies performed prior to skeletal maturity, resulting pelvic deformities largely remodeled with growth.
Discussion: Pelvic osteotomies can alter normal pelvic parameters and may influence the ability for vaginal delivery. Obstetricians may recommend C-section for patients undergoing non-PAO osteotomies depending on skeletal maturity status at the time of their osteotomy and other obstetric-related factors such as fetal size and natural pelvic relaxation. The literature on this subject, however, remains limited.
Levels of Evidence: Level IV
Key Concepts
- Pelvic osteotomies for residual hip dysplasia or other childhood hip disorders alter normal pelvic parameters that may preclude the possibility of vaginal birth, particularly when performed after skeletal maturity.
- The Chiari osteotomy primarily alters the dimensions of the pelvic inlet and mid-pelvis, while the Salter, double, and triple osteotomies decrease the size of the pelvic outlet.
- The Bernese periacetabular osteotomy does not influence bony birth canal anatomy.
- Pelvic deformities resulting from pelvic osteotomies performed before skeletal maturity often remodel with growth.
- Obstetricians may recommend cesarean section after pelvic osteotomy, particularly when performed bilaterally, dependent on obstetric-specific factors.
Introduction
Hip dysplasia is a common pathology that may result in pain and eventual arthrosis.1 If diagnosed early, nonoperative treatment is often successful. In many cases, radiographic evidence of dysplasia is only identified in adolescence/young adulthood after experiencing hip discomfort. Regardless of age, various pelvic osteotomies can be performed to improve femoral head coverage with the goal of delaying/preventing future hip replacement.2 For female patients and their families, a common question is the impact of these osteotomies on future pregnancy.
Sutherland raised concerns regarding the possibility of vaginal birth after double osteotomy, but this was not addressed in the original descriptions of several other commonly performed osteotomies.3–6 The potential impact on pregnancy was mentioned by Ganz in his original description of the Bernese periacetabular osteotomy (PAO), as he noted no change in the pelvic birth canal.7
Unfortunately, the literature on this topic is varied and wide-ranging. This study was designed to understand the impact of pelvic osteotomy on birth canal anatomy by systematically reviewing the current literature to help guide counseling among orthopaedic surgeons and their patients/families as well as obstetricians.
Methods
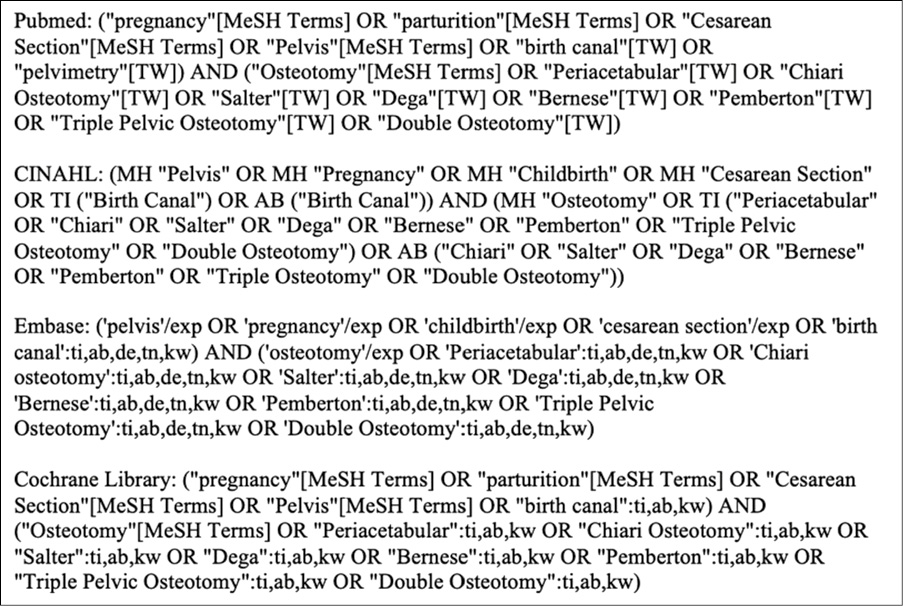
Four online databases (PubMed, Embase, CINAHL, and Cochrane Library) were used to search for studies assessing the impact of pelvic osteotomies on birth canal anatomy or cesarean section (C-section) rates. This search was performed on 12/15/2021, and generally included the terms “pregnancy,” “birth canal,” “pelvis,” “cesarean section,” and various pelvic osteotomies in an attempt to broadly capture the available literature on this subject based on preliminary review of these topics. The detailed methodology can be found in Figure 1.
Figure 1. Search strategy.
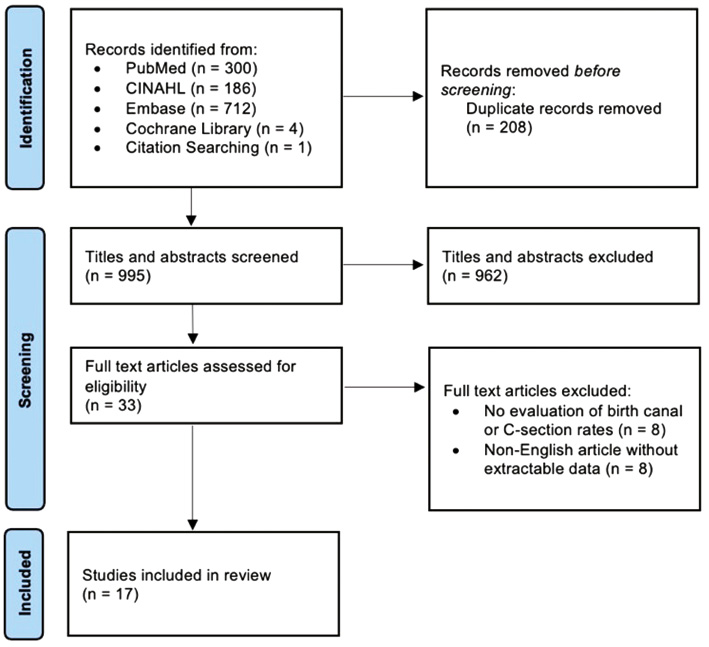
This strategy generated 1,202 studies, which were imported into Covidence, a systematic review management platform (Veritas Health Innovation, Melbourne, Australia). Covidence removed 208 articles as duplicates. PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines were then used to assess the 995 available studies (Figure 2). Titles/abstracts were screened by two authors (JTB and BKE) to eliminate those that were clearly irrelevant (e.g., animal studies, no evaluation of pelvic anatomy/pregnancy). The 32 titles/abstracts receiving ≥1 “yes” vote underwent full-text review. Similar methodology was used for screening articles, with conflicts resolved through discussion. Last, a thorough review of the bibliographies of included studies revealed one additional article missed during the initial search.8
Figure 2. PRISMA diagram.
This led to the final inclusion of 17 articles evaluating five types of pelvic osteotomies. All studies evaluated cadaveric/model, clinical, or radiographic pelvises (Figure 3 and Table 1) of neuro-typical patients (e.g., hip dysplasia, Legg-Calve-Perthes disease, or post-traumatic arthritis) and largely excluded pathology arising from bladder exstrophy and neuromuscular/chromosomal disorders. Also excluded were non-English articles. Three articles were included despite the main text being non-English as their abstracts and detailed relevant results/conclusions were in English.9–11 Results are broken down by osteotomy in the approximate chronologic age at which they are performed. Clinical results and radiographic outcomes are reported in the manuscript text, while anatomic changes in cadavers/models are reported in tables.
Figure 3. Obstetric pelvic planes. Three-dimensional reconstructions of a female pelvis are used here to illustrate the different pelvic planes commonly referenced in obstetrics. Panel 3A shows the transverse diameter of the pelvic inlet at the superior margin of the true pelvis. Panel 3B illustrates the interspinous or transverse diameter of the mid-pelvis, which is typically described as the most critical location of the birth canal for fetal passage. In panel 3C, line 1 represents the anatomic or true conjugate (pelvic inlet) and line 2 shows the obstetric conjugate. Lines 3 and 4 in panel 3C demonstrate the obstetric and anatomic diameters of the pelvic outlet, respectively

Table 1. Pelvic Plane Definitions
| Pelvic Inlet |
|
| Mid-Pelvis |
|
| Pelvic Outlet |
|
Results
Salter
Four studies evaluated the Salter osteotomy and its influence on the birth canal in both cadavers/models and human patients, including at follow-up after skeletal maturity (Table 2).18–21 No studies evaluated C-section rates.
Table 2. Common Childhood Osteotomies
| Osteotomy | Study | Year | Type | Findings |
|---|---|---|---|---|
| Salter | Loder18 | 1993 | Model |
|
| Küsswetter20 | 1985 | Cadaver |
|
|
| Winkelmann21 | 1984 | Model, Cadaver |
|
|
| Chiari | Høgh8 | 1987 | Cadaver |
|
| Küsswetter20 | 1985 | Cadaver |
|
|
| Loder18 | 1993 | Model |
|
|
| Winkelmann21 | 1984 | Model, Cadaver |
|
Loder et al. reported on five patients who underwent unilateral Salter, with average decreases of 9% and 14% in the transverse mid-pelvis and outlet, respectively.18 For one patient with follow-up at skeletal maturity, there was substantial remodeling of the transverse mid-pelvis from -4% postoperatively (from pre-surgical dimensions) to +13% at follow-up and of the outlet from -9% to 0%. Loder et al. later evaluated 21 patients who underwent unilateral Salter with mean 9.7-year follow-up. They found narrowing of the outlet of -8.6% after surgery, secondary in magnitude only to the triple osteotomy.19 After skeletal maturity, the transverse mid-pelvis was below a pre-determined 9.5 cm threshold in 14% of patients, while the transverse outlet was below normal thresholds in 10%.
Chiari
Eight studies evaluated the Chiari osteotomy in models/cadavers and patients (Table 2). Seven studies evaluated radiographic characteristics,8,10,11,18–21 while four studies evaluated its impact on C-section rates.8,10,11,22
Rejholec et al. reported that 22/61 births (36%) after Chiari were via C-section, which was significantly greater than a mean 10% rate for the city of Prague.18,22 Kotz et al. similarly studied 37 patients who went on to pregnancy after Chiari, noting significant radiographic deformation of the pelvic inlet. Eighteen- and fifty-percent who had unilateral and bilateral procedures, respectively, went on to C-sections.10 Smakhtina et al. evaluated 26 patients who became pregnant after unilateral Chiari, observing that 15% underwent C-section secondary to the osteotomy (the exact indication for this decision not being specified) while another 15% received elective C-section. They noted that despite significant deformation of the inlet, this largely remodeled 2-2.5 years postosteotomy.11
Høgh et al. studied 30 patients who experienced pregnancy after Chiari, advising C-section for 25% of unilateral and 100% of bilateral osteotomies, reflecting an author-specific policy decision. However, they noted considerable inlet remodeling at follow-up of 10 years and felt vaginal birth was feasible for most cases.8
For one patient who underwent Chiari before puberty by Loder et al., the transverse inlet increased from -14% postoperatively (from pre-surgery) to +4% at 2.5 year follow-up, while the mid-pelvis remodeled from -16% to +2%.18 For two patients who underwent osteotomy at skeletal maturity, there was minimal remodeling of the pelvic inlet/mid-pelvis at mean 5.5-year follow-up. They later evaluated two patients at skeletal maturity who had undergone Chiari, reporting that one had a transverse mid-pelvis diameter <9.5 cm.19 The postoperative transverse mid-pelvis measurements were also smaller (mean 9.8 cm) than any other osteotomy performed (10.2 cm). Conversely, there was overall milder narrowing of pelvic parameters in comparison to their earlier model-based studies. Winkelmann et al. performed Chiari in 15 patients, and despite some remodeling after surgery, there remained substantial narrowing of the birth canal 1-4 years postoperatively, particularly when performed bilaterally.21
Triple Innominate
Four studies evaluated variations of the triple osteotomy and its influence on the birth canal, while no study evaluated C-section rates (Table 3).18,19,21,23 Loder et al. evaluated pelvic dimensions for two patients who underwent the Steel triple osteotomy.18 They observed substantial remodeling after puberty, including an increase in the transverse outlet from -15% postoperatively (compared to the pre-surgery) to -2% at follow-up.
Table 3. Pelvic Osteotomies Performed Around Skeletal Maturity
| Osteotomy | Study | Year | Type | Findings |
|---|---|---|---|---|
| Steel, Tönnis | Loder18 | 1993 | Model |
|
| Modified Steel | Schwarz23 | 2014 | Cadaver |
|
| Steel (and modifications by Carlioz/Tönnis) | Winkelmann21 | 1984 | Model, Cadaver |
|
| Sutherland (Double Osteotomy) | Loder18 | 1993 | Model |
|
| Winkelmann21 | 1984 | Model, Cadaver |
|
|
| Bernese (Ganz) | Loder18 | 1993 | Model |
|
They later radiographically reported on five patients who underwent Steel’s osteotomy and were ≥14 years at follow-up.19 They found that the transverse outlet decreased by 12% after surgery, with little change in the mid-pelvis. However, at follow-up, 40% were below traditional transverse mid-pelvis thresholds (<9.5 cm), and 40% were below reported thresholds for the pelvic outlet. Winkelmann et al. performed the triple osteotomy in 10 patients between 14-34 years, with CT revealing up to 3.3 cm of mid-pelvis narrowing.21
Double Innominate
Only two studies evaluated Sutherland’s double osteotomy, focusing on its radiographic impact on the birth canal in cadavers/models and a single patient (Table 3).18,21 For the skeletally immature patient, there was significant pelvic remodeling during puberty with a reported increase in the transverse outlet from -26% postoperatively (from pre-surgical measures) to -12% at skeletal maturity.18
Periacetabular
Seven studies assessed the Bernese PAO (Table 3). Three studies assessed its clinical influence on pregnancy/C-section rates.9,24,25 Four studies evaluated its radiographic impact on the birth canal, while one study evaluated pelvic models.9,18,19,26,27 Last, two studies evaluated less commonly performed variants of the PAO.28,29
Bartiosiak et al. retrospectively surveyed patients with pregnancies after PAO and reported a C-section rate of 53% in 31 women, significantly higher than the reported population average of 32% (Table 4).24 However, they reported that for 55%, the obstetrician was concerned over the impact of PAO on delivery, and 30% of C-sections were specifically scheduled due to this concern. They additionally found no differences in infant characteristics (e.g., birth weight) compared to national averages. Flückiger et al. similarly reported a higher C-section rate of 36% (10/28 pregnancies) after PAO, nearly twice their national average.9 In 50%, this were attributed to the obstetrician anticipating challenges during delivery, and they again found no differences in birth weight. Valenzuela et al. studied sexual activity and pain after PAO, reporting that 8/23 (35%) children born after PAO were delivered via C-section, with similar birth weights compared to population averages.25
Table 4. Cesarean Section Rates by Pelvic Osteotomy
| Osteotomy Type | Unilateral Osteotomy | Bilateral Osteotomy |
|---|---|---|
| Salter | - | - |
| Chiari | 18-36%8,10,11,22 | 50-100%8,10 |
| Triple | - | - |
| Double | - | - |
| Periacetabular | 35-53%9,24,25 | - |
Loder et al. radiographically evaluated two patients after PAO, with all birth canal measures above normative thresholds.19 Using more contemporary pelvimetry methodology, Trousdale et al. evaluated AP/transverse diameters of the pelvic inlet/mid-pelvis using MRI for seven women undergoing PAO.26 They observed no decrease in birth canal measures 2-3 months after surgery but noted excessive acetabular fragment retroversion could lead to pelvic ring narrowing from a poorly positioned medial wall. They also reported the medial wall was the narrowest diameter of the bony birth canal for all patients rather than the mid-pelvis as has been traditionally taught. Similarly, Shao et al. evaluated the pelvises of 31 patients before/after PAO using 3D-CT and determined no change in the narrowest point of the birth canal.27
Though the Bernese PAO is more common, several other variants, including the curved PAO (CPAO) and eccentric rotational PAO (EPAO), have been described. Ishimatsu et al. evaluated 29 patients who underwent bilateral CPAO, noting no change in the pelvic inlet, contraction (interspinous diameter), or outlet.29 However, the narrowest diameter of the birth canal for all patients was, similar to Trousdale, the transverse diameter between the pelvic teardrops. This measure was significantly decreased after bilateral PAO and below the 9.5 cm threshold for safe delivery in 5/29 cases, leading the authors to suggest consideration of C-section. Masui et al. evaluated the EPAO and noted no change in pelvimetry measures for 21 women who underwent childbirth after surgery.28 Additionally, 23% and 25% of patients who had unilateral and bilateral osteotomies, respectively, gave birth via C-section.
Discussion
Overall, the literature assessing the influence of pelvic osteotomy on birth canal anatomy and the necessity for C-section is of low quality/quantity. The limitations of this study are largely a result of these studies being conducted in a small number of patients or in models/cadaveric specimens, limiting performance of a meta-analysis. Further, cesarean section rates were not available for several osteotomy types, limiting comparison by procedure. Many studies also did not account for pelvic remodeling that may occur after osteotomy in skeletally immature patients. These articles also had variable inclusion criteria for each osteotomy and excluded several commonly performed infantile osteotomies such as the Dega or Pemberton.
Loder et al. discussed that a 9.5 cm transverse mid-pelvis value was selected as the relevant low-normal threshold for C-section because in obstetric studies, it was both the average interspinous distance for patients undergoing C-section and was two standard deviations below mean interspinous distances for vaginal deliveries.19,30 Subsequently, they recommended informing patients with interspinous diameters <9.5 cm on AP pelvis X-rays that they may require C-section.
There appears to be significant pelvic remodeling potential when osteotomies are performed before puberty. Loder et al. found that patients whose transverse mid-pelvis was <9.5 cm at follow-up were 4.8 years older at osteotomy (closer to skeletal maturity) and therefore did not experience substantial remodeling.19 Though far from conclusive, this suggests that for osteotomies such as the Salter, typically performed at a young age, it is likely that pelvic deformities precluding vaginal delivery will remodel over time.
Additionally, while the Chiari osteotomy appears to primarily influence the pelvic inlet/mid-pelvis, the Salter, double, and triple osteotomies decrease the pelvic outlet. There is, unfortunately, little literature discussing the impact of a narrow outlet on vaginal birth as any pathology affecting the outlet also narrows the mid-pelvis.19,31 Despite recommendations for elective C-section from several studies after pelvic osteotomy, it is unknown whether decreased outlet radiographic measures are clinically relevant as the mid-pelvis is the most common/best understood site of dystocia.14
Perhaps most important, the pelvic dimensions that preclude vaginal delivery are not entirely understood and were not consistent across studies. For many in the obstetrics and orthopaedic communities, pelvimetry and evaluation of pelvic dimensions are relatively outdated methods of determining vaginal delivery feasibility32 since the pelvis relaxes/expands during pregnancy, which may make static measures of pelvic dimensions less important. Hormonal changes (specifically relaxin) lead to ligamentous laxity of the sacroiliac/sacrococcygeal joints and increased width of the pubic symphysis to expand the pelvis for childbirth.33,34 Studies have also shown maternal positioning can significantly increase pelvic dimensions up to 2 cm.35–37
There are other factors outside of bony parameters that impact vaginal delivery, including those of the uterus/cervix and fetus (namely size and positioning). Radiographic pelvimetry has also been shown to increase the rate of C-section, likely due to identification of “sub-normal” dimensions.38 Static measures of pelvic morphology, therefore, not only differ from dynamic changes in pelvic capacity that allow for vaginal birth but likely offer limited clinical prognostication for vaginal delivery in many older studies on pelvic osteotomies. Conversely, MRIs can provide additional soft tissue pelvic parameters in pregnant patients with a history of pelvic osteotomy without concern over the effects of ionizing radiation on the developing fetus. Surgeons may thus, with caution, consider use of modern radiographic parameters to guide decision-making regarding cesarean delivery after osteotomy. Given all these limitations, we attempted to interpret the feasibility of vaginal delivery for each osteotomy.
Salter
One of the earliest re-directional osteotomies described, the Salter involves a transverse cut of the ilium between the ASIS/AIIS.3 The mobile acetabular fragment is hinged through the symphysis to improve anterolateral coverage.2 Typically performed in patients with congenital dislocation/subluxation of the hip between 1.5-6 years old, this osteotomy predominantly reduced the AP/transverse diameters of the outlet and marginally of the mid-pelvis.18–21 This was apparently due to medial translation of the ischial tuberosity resulting from acetabular rotation through the symphysis.
As there was no C-section data available, it is unknown how this osteotomy influences C-section rates, though the outlet is rarely the site of dystocia, which instead occurs at the mid-pelvis.14 There is also more potential for remodeling after a Salter osteotomy as this is frequently performed in younger children,39 with almost full remodeling to normal parameters observed.18 As Loder et al. reported 14% of patients below a 9.5 cm mid-pelvis threshold after surgery, the Salter may require C-section when performed bilaterally,19 though the impact of pelvic relaxion may make vaginal delivery possible.20
Chiari
The Chiari osteotomy is a salvage procedure described for adolescent/adult patients with dysplastic hips in whom a re-direction/re-orientation osteotomy is not viable. It utilizes a supra-acetabular iliac osteotomy below the AIIS, through the sciatic notch, to allow for medial acetabular displacement.6 Hinging through the symphysis, this increases coverage via exposure of cancellous bone and interposed capsule laterally.2
Through medial acetabular displacement, 5/6 radiographic studies demonstrated a marked reduction in the transverse inlet/mid-pelvis to dimensions smaller than for any other osteotomy.19 This deformation largely remodeled when performed prior to puberty,8,11,18 but persisted when performed at skeletal maturity.18,19,21 Based on existing clinical data, the Chiari does not appear to increase C-section rates when performed unilaterally (18-36%), though Rejholec et al. reported a nearly 26% higher C-section rate after osteotomy.8,10,11,22 This may be due to remodeling when performed in prepubertal children. When performed bilaterally, the osteotomy is associated with C-section rates of 50-100%.8,10 For skeletally mature individuals, C-section may be indicated in both unilateral and bilateral cases dependent on the ability of natural pelvic relaxation to accommodate delivery.
Triple Innominate
Unlike the posterior column-preserving PAO, the triple osteotomy utilizes complete cuts of the ilium, ischium, and pubis to reorient the acetabulum in children with open triradiate cartilage. This allows for both complete acetabular mobility, unlike the Salter osteotomy, and improved lateral coverage with cartilage, unlike the Chiari osteotomy.2
Steel’s triple osteotomy4 was shown to significantly reduce the pelvic outlet, which partially remodeled with maturation.18,19,21,23 Additionally, Loder et al. reported that postmenarchal transverse diameters at the mid-pelvis and outlet were under threshold in 40% of patients after unilateral procedures.19 No articles specifically described pregnancy outcomes after triple osteotomy and therefore it is not known how C-section rates are impacted, though the included studies reported relatively high rates of residual pelvic deformation at skeletal maturity. Other factors, including pelvic relaxation, may further allow for vaginal delivery, and C-section decisions should be based on individual anatomy.23
The Tönnis triple osteotomy5 is less common due to the creation of a potentially unstable pelvis with higher ischial nonunion risk.40 Further, the limited data available on its impact on pregnancy/pelvic anatomy is inconsistent, with two studies reporting only possible mid-pelvis narrowing.18 There is consequently not enough information regarding C-section after Tönnis osteotomy.
Double Innominate
Sutherland designed the double osteotomy to avoid the separate ischial/pubic cuts in the triple osteotomy.41 It involves a similar Salter-type supra-acetabular iliac osteotomy with a single pubic osteotomy, medial to the obturator foramen/close to the symphysis. The pubic osteotomy involves removal of a ~1 cm bone wedge, allowing for acetabular medialization as seen in the Chiari to improve coverage (but with articular cartilage). The acetabular fragment, including the ischial spine/tuberosity, is then rotated anterolaterally. Sutherland recommended its application in patients aged >6 years with a reducible dislocated/subluxated hip, similar to the demographic application of the triple.
Understanding the anatomic changes occurring during this procedure, it is unsurprising that this osteotomy significantly reduces the AP/transverse diameters of outlet and marginally of the mid-pelvis.18,21 Though no studies evaluated its impact on pregnancy, Sutherland specifically recommended that female patients be wary of the possibility of C-section after a double osteotomy because of its intentional medial displacement and decrease in the transverse outlet.41
Periacetabular
The standard Bernese PAO is used for dysplasia in skeletally mature individuals (closed triradiate cartilage) without significant osteoarthritis. It involves complete iliac/pubic cuts with an incomplete ischial cut that maintains the posterior column, allowing for early weight-bearing. As Ganz noted, the PAO does not change the diameter of the true pelvis and allows for tremendous acetabular re-orientation.7
Across all cadaveric/radiographic studies, there were no changes in pelvic parameters after PAO. While some studies reported higher C-section rates compared to population norms, many noted this was likely reflective of obstetrician preference rather than anatomic requirement. Obstetricians should therefore feel comfortable proceeding with vaginal delivery after unilateral or bilateral PAO.
Conclusions
Based on the literature available, the Bernese PAO does not influence the bony birth canal and patients should be counseled that a vaginal delivery should not be hindered by this hip surgery. However, for patients undergoing Chiari osteotomy and other re-orientational (non-PAO) and redirectional osteotomies after skeletal maturity, we recommend a discussion regarding the potential requirement for cesarean section. Physicians may, with caution, consider use of more modern radiographic parameters to guide decision-making regarding cesarean after unilateral osteotomy. MRI specifically can provide pelvic parameters in pregnant patients with a history of non-PAO pelvic osteotomy without concern over the effects of ionizing radiation on the developing fetus. Based on the available literature, aside from the Bernese PAO, obstetricians may consider cesarean section when a patient has a history of bilateral pelvic osteotomy procedures while accounting for other factors such as fetal size and natural pelvic relaxation at the time of delivery.
Additional Links
- POSNAcademy, Pelvis Osteotomies for Developmental Dysplasia of the Hip
- Association of Professors of Gynecology and Obstetrics, Pelvic Anatomy/Diameters
Disclaimer
No funding was received. The authors have no conflicts of interest to report related to this manuscript.
References
- Pollet V, Percy V, Prior HJ. Relative risk and incidence for developmental dysplasia of the hip. J Pediatr. 2017;181:202-207.
- Selberg CM, Chidsey B, Skelton A, et al. Pelvic osteotomies in the child and young adult hip: indications and surgical technique. J Am Acad Orthop Surg. 2020;28(6):e230-e237.
- Salter RB, Dubos JP. The first fifteen year’s personal experience with innominate osteotomy in the treatment of congenital dislocation and subluxation of the hip. Clin Orthop Relat Res. 1974;(98):72-103.
- Steel HH. Triple osteotomy of the innominate bone. J Bone Joint Surg Am. 1973;55(2):343-350.
- Tönnis D, Behrens K, Tscharani F. A modified technique of the triple pelvic osteotomy: early results. J Pediatr Orthop. 1981;1(3):241-249.
- Chiari K. Medial displacement osteotomy of the pelvis. Clin Orthop Relat Res. 1974;(98):55-71.
- Ganz R, Klaue K, Vinh TS, et al. A new periacetabular osteotomy for the treatment of hip dysplasias. Technique and preliminary results. Clin Orthop Relat Res. 1988;(232):26-36.
- Høgh J, Macnicol MF. The Chiari pelvic osteotomy. A long-term review of clinical and radiographic results. J Bone Joint Surg Br. 1987;69(3):365-373.
- Flückiger G, Eggli S, Kosina J, et al. Birth after peri-acetabular osteotomy. Orthopade. 2000;29(1):63-67.
- Kotz R, Wagenbichler P. Influence of a Chiari pelvic osteotomy on subsequent labor and delivery. Geburtshilfe Frauenheilkd. 1973;33(6):471-477.
- Smakhtina KA. Anatomic characteristics of the female pelvis following ostectomy of the iliac bone by Chiari’s method. Akush Ginekol. 1979;(6):12-14.
- Bull HC. Pelvimetry in obstetrics. Postgrad Med J. 1949;25(285):310-318.
- Siccardi MA, Imonugo O, Valle C. Anatomy, Abdomen and Pelvis, Pelvic Inlet. In: StatPearls. StatPearls Publishing; 2021.
- Hacker NF, Gambone JC, Hobel CJ. Hacker & Moore’s Essentials of Obstetrics and Gynecology, 5th Edition. Saunders; 2009.
- Dashe JS, Bloom SL, Spong CY, et al. Williams Obstetrics, 25th Edition. McGraw Hill Professional; 2018.
- Eggleton JS, Cunha B. Anatomy, Abdomen and Pelvis, Pelvic Outlet. In: StatPearls. StatPearls Publishing; 2021.
- Russell JG, Richards B. A review of pelvimetry data. Br J Radiol. 1971;44(526):780-784.
- Loder RT, Karol LA, Johnson S. Influence of pelvic osteotomy on birth canal size. Arch Orthop Trauma Surg. 1993;112(5):210-214.
- Loder RT. The long-term effect of pelvic osteotomy on birth canal size. Arch Orthop Trauma Surg. 2002;122(1):29-34.
- Küsswetter W, Magers H, Hirasawa Y. Pelvic deformity after simple pelvic osteotomy. Nihon Geka Hokan. 1985;54(2):67-74.
- Winkelmann W. The narrowing of the bony pelvic cavity (birth canal) by the different osteotomies of the pelvis. Arch Orthop Trauma Surg. 1984;102(3):159-162.
- Rejholec M, Stryhal F, Rybka V, et al. Chiari osteotomy of the pelvis: a long-term study. J Pediatr Orthop. 1990;10(1):21-27.
- Schwarz O, Chomiak J, Dungl P, et al. The influence of triple pelvic osteotomy on birth canal size. Hip Int. 2014;24(1):32-38.
- Bartosiak K, Stockburger C, Stockburger J, et al. Is previous periacetabular osteotomy associated with pregnancy, delivery, and peripartum complications? Clin Orthop Relat Res. 2020;478(1):68-76.
- Valenzuela RG, Cabanela ME, Trousdale RT. Sexual activity, pregnancy, and childbirth after periacetabular osteotomy. Clin Orthop Relat Res. 2004;(418):146-152.
- Trousdale RT, Cabanela ME, Berry DJ, et al. Magnetic resonance imaging pelvimetry before and after a periacetabular osteotomy. J Bone Joint Surg Am. 2002;84(4):552-556.
- Shao L, Li H, Liu X, et al. Quantitative analysis of bony birth canal for periacetabular osteotomy patient by template fitting. Phys Med Biol. 2021;66(2):025007.
- Masui T, Hasegawa Y, Yamaguchi J, et al. Childbirth and sexual activity after eccentric rotational acetabular osteotomy. Clin Orthop Relat Res. 2007;459:195-199.
- Ishimatsu T, Naito M, Kinoshita K, et al. Three-dimensional computed tomography analysis on bony birth canal after bilateral periacetabular osteotomy. J Orthop Sci. 2017;22(3):531-535.
- Abitbol MM, Taylor UB, Castillo I, et al. The cephalopelvic disproportion index. Combined fetal sonography and x-ray pelvimetry for early detection of cephalopelvic disproportion. J Reprod Med. 1991;36(5):369-373.
- Mengert WF. Estimation of pelvic capacity. J Am Med Assoc. 1948;138(3):169-174.
- VanSickle C, Liese KL, Rutherford JN. Textbook typologies: challenging the myth of the perfect obstetric pelvis. Anat Rec. 2022;305(4):952-967.
- Heckman JD, Sassard R. Musculoskeletal considerations in pregnancy. J Bone Joint Surg Am. 1994;76(11):1720-1730.
- Aldabe D, Ribeiro DC, Milosavljevic S, et al. Pregnancy-related pelvic girdle pain and its relationship with relaxin levels during pregnancy: a systematic review. Eur Spine J. 2012;21(9):1769-1776.
- Siccardi M, Valle C, Di Matteo F. Dynamic external pelvimetry test in third trimester pregnant women: shifting positions affect pelvic biomechanics and create more room in obstetric diameters. Cureus. 2021;13(3):e13631.
- Hemmerich A, Bandrowska T, Dumas GA. The effects of squatting while pregnant on pelvic dimensions: A computational simulation to understand childbirth. J Biomech. 2019;87:64-74.
- Reitter A, Daviss BA, Bisits A, et al. Does pregnancy and/or shifting positions create more room in a woman’s pelvis? Am J Obstet Gynecol. 2014;211(6):662.e1-9.
- Pattinson RC, Cuthbert A, Vannevel V. Pelvimetry for fetal cephalic presentations at or near term for deciding on mode of delivery. Cochrane Database Syst Rev. 2017;3:CD000161.
- El-Sayed M, Ahmed T, Fathy S, et al. The effect of Dega acetabuloplasty and Salter innominate osteotomy on acetabular remodeling monitored by the acetabular index in walking DDH patients between 2 and 6 years of age: short- to middle-term follow-up. J Child Orthop. 2012;6(6):471-477.
- Tschauner C, Sylkin A, Hofmann S, et al. Painful nonunion after triple pelvic osteotomy. Report of five cases. J Bone Joint Surg Br. 2003;85(7):953-955.
- Sutherland DH, Greenfield R. Double innominate osteotomy. J Bone Joint Surg Am. 1977;59(8):1082-1091.