
Quality, Safety and Value (QSVI)
Accuracy of Non-Invasive Hemoglobin (nHgb) Monitoring in an AIS Population
Scottish Rite for Children, Dallas, TX
Correspondence: Amy L. McIntosh, MD, Scottish Rite for Children, 2222 Welborn St., Dallas, TX 75219. E-mail: [email protected]
Received: October 3, 2022; Accepted: April 5, 2023; Published: May 1, 2023
Volume 5, Number 2, May 2023
Abstract
Local Problem: Needle phobia and fear of blood draws are very common in children and adolescents. Noninvasive hemoglobin (nHgb) monitoring in children was first introduced in the Intensive Care Unit (ICU) setting. Later, our total joint arthroplasty colleagues demonstrated that nHgB monitoring was more efficient, less expensive, and preferred by patients compared to invasive hemoglobin (iHgb) monitoring.
Specific Aims: The goal of this Quality Initiative (QI) project is to compare the accuracy and reliability when comparing nHgb monitoring and iHgb (blood draw) in an Adolescent Idiopathic Scoliosis (AIS) population. The purpose was to evaluate the correlation between nHgb and iHgb monitoring and develop a nHgb threshold above which a patient would no longer require a blood draw, thus minimizing resource utilization as well as blood draw-related anxiety and pain during the postoperative period.
Intervention: We enrolled 60 consecutive patients undergoing posterior spine fusion/instrumentation (PSFI) for AIS. Average estimated blood loss (EBL) was 415cc, and 189 cc was returned via cell saver. 2/60 (3.3%) patients required an allogenic blood transfusion perioperatively.
nHgb and iHgb values were obtained within 60 minutes of each other at three separate time points (preoperative, in Post-Anesthesia Care Unit (PACU), and postoperative day (POD 1) at 0700) iHgb and nHgb values were recorded. The results were retrospectively reviewed and analyzed. Paired t tests were utilized to compare mean (n/i) Hgb values. Pearson correlation coefficients were calculated at all three time points. Receiver Operating Characteristic (ROC) curve analysis was performed on the postoperative values to determine a threshold.
Results: There was a moderate positive correlation at all three time points (0.4, 0.59, 0.6) (p= 0.005, <0.001, <0.001).
At all three time points, the mean nHgb value was 1-2 g/dL higher than the mean iHgb value, and this was statistically significant.
Guidelines for an Allogenic Blood Transfusion (ABT) at our institution were developed through consensus between the surgical and anesthesia teams. Indications for a postoperative ABT include iHgb 7.0 – 8.0 g/dL along with clinical signs of anemia such as persistent hypotension, tachycardia, dyspnea, lethargy, confusion, postural dizziness not responsive to a fluid challenge, or iHgb <7.0 g/dL, regardless of signs/symptoms of anemia.
There were not enough data points to correlate nHgb measurements with a patient’s need to receive an ABT due to the low occurrence rate (3.3%). Therefore, we focused on a nHgb threshold at which a postoperative venous blood draw would not be necessary.
54/60 patients had a lab value of iHgb ≥ 9.0g/dL at 0700 on POD 1 and only 6 of the 60 patients had an iHgb ≤ 8.0 g/dL. Thus, we chose iHgb ≥ 9.0g/dL as the threshold. Based on data from the ROC curve analysis, a patient with a nHgb value of ≥10.8 g/dL had an iHgb value of ≥9.0 g/dL with 87% sensitivity.
Based on the ABT guidelines stated above, no patient with a nHgb ≥ 10.8 g/dl would require an ABT, therefore a venipuncture would be unnecessary.
Conclusions: Noninvasive Hgb monitoring was found to correlate with iHgb in pediatric AIS patients undergoing PSFI. Surgeons could consider screening AIS patients postoperatively with nHgb monitoring and only order iHgb measurement if the nHgb value is <10.8 g/dL resulting in improvement in the patient experience.
Introduction
Needle phobia and fear of blood draws is very common in children and adolescents.1 Noninvasive hemoglobin (nHgb) monitoring in children was introduced in the Intensive Care Unit (ICU) setting to rapidly assess Hgb values without having to perform a blood draw. A 2014 study in pediatric ICU patients demonstrated that nHgb monitoring and invasive Hgb (iHgb) monitoring in children with normal Hgb and mild anemia were positively correlated.2
Literature from our total joint arthroplasty colleagues has demonstrated that noninvasive hemoglobin (nHgb) monitoring is more efficient, less expensive, and preferred by patients compared to invasive hemoglobin (iHgb) monitoring. In their report, 100% of patients with a nHgb value ≥10.5 g/dL had a iHgb >8.0 g/dL.3
However, this information was gathered on an adult patient population that underwent joint replacement surgery (hip or knee). It is unclear how this data translates to our pediatric adolescent idiopathic scoliosis (AIS) patient population that is undergoing posterior spinal fusion with instrumentation (PSFI) surgery.
Local Problem
From 2015-2017, our allogenic blood transfusion (ABT) rate for AIS patients undergoing PSFI was 18.2% in the perioperative period. Non-modifiable risk factors for ABT were younger age, lower BMI, lower preop Hgb and Hct, larger preop Cobb angle, greater number of levels fused, and the use of osteotomies. Receiver Operating Curve (ROC) analysis using POD 1 hemoglobin levels showed a protective cutoff value of 9.1 g/dL. Patients that had a POD 1 Hgb ≥ 9.1g/dL were extremely unlikely to require a transfusion. The sensitivity and specificity of this test were 0.78 and 0.75, respectively, and the Area Under the Curve (AUC) was 0.834. The rate of transfusion in patients with a POD 1 hemoglobin greater than or equal to 9.1 g/dL was 2.2% (negative predictive value of 97.8%) while the rate of transfusion in patients with hemoglobin below 9.1 g/dL was 19.1%.4
Based on this data, in 2018 we initiated a quality improvement (QI) project to standardize preoperative patient optimization and perioperative indications for ABT. Consensus-based guidelines were developed with the surgical and anesthesia teams which resulted in a decreased ABT rate from 18.2% to 8.9% (a greater than 50% reduction) (Table 1).4 The ABT rate continued to decrease slightly to 7.63% from 2019-2020. However, these guidelines all required iHgb monitoring.
Table 1. Consensus Based Guidelines for ABT
| • Preoperative guidelines |
| A complete blood count was obtained 8 to 12 weeks prior to surgery. Oral iron therapy was initiated for Hgb <12 g/dL and Mean Corpuscular Volume (MCV) was low. |
| • Intraoperative guidelines |
| Allogenic transfusion for Hgb of <8.0 g/dL along with clinical signs of anemia such as persistent hypotension despite fluid and vasopressors, tachycardia, persistently decreased urine output, or continued blood loss. |
| Goal mean arterial pressure <70 mm Hg during dissection and screw placement. With increase to >80 mmHg during reduction maneuvers. |
| • Postoperative guidelines |
| Transfusion for Hgb 7.0 – 8.0 g/dL along with clinical signs of anemia such as persistent hypotension, tachycardia, dyspnea, lethargy, confusion, postural dizziness not responsive to a fluid challenge. |
| Allogenic transfusion for Hgb <7.0 g/dL, regardless of signs/symptoms of anemia. |
Specific Aims
The goal of this QI project is to compare the accuracy and reliability when comparing nHgb monitoring and iHgb (blood draw) in an AIS population. The purpose is to identify the correlation between nHgb and iHgb monitoring which would allow a nHgb threshold to be determined. Patients with a nHgb level above that threshold would no longer require a blood draw postoperatively, thus minimizing resource utilization as well as blood draw related anxiety and pain during the postoperative period.
Intervention
Patients aged 10 to 21 years with the diagnosis of AIS who underwent PSFI were prospectively included. IRB approval was not necessary for this QI project. Baseline Hgb was be obtained within a week of the scheduled PSFI surgery. During this visit, venipuncture was performed to obtain an iHgb measurement and a nHgb measurement was performed by a registered nurse (RN) within 1 hour prior to venipuncture. The nHgb was measured using the Pronto® Pulse CO-Oximeter® (Masimo Corp., Irvine, CA). Similarly, in the PACU immediately following surgery, a nHgb measurement was obtained by a RN just prior to blood being drawn off an arterial line for iHgb measurement. We obtained nHgb measures as part of the routine vital assessments on POD 1 at the same time as morning lab draw.
Measures and Analysis
Continuous variables between iHgb and nHgb were compared using paired t tests. To determine the strength of agreement between the two groups, the concordance correlation coefficient (CCC) was calculated. Receiver operating characteristics (ROC) curves were used to determine the optimal cutoff values for nHgb and need for ABT.
Results
We enrolled 60 consecutive patients undergoing PSFI for AIS over a 6-month period. Average EBL was 415 cc (100-1200 cc), and average 189 cc (56-509 cc) was returned via cell saver. 2/60 (3.3%) patients required an allogenic blood transfusion perioperatively.
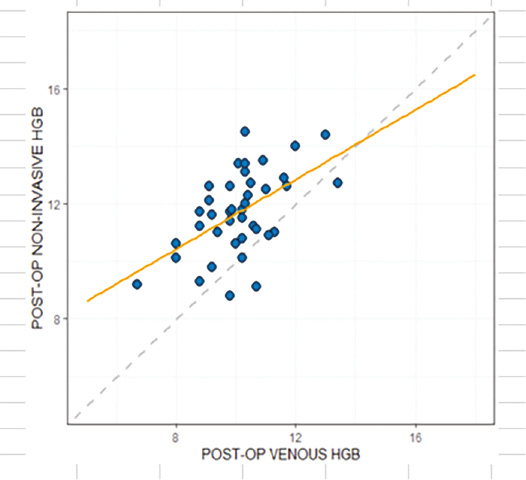
There was a moderate positive Pearson’s correlation at all three time points (0.4, 0.59, 0.6) (p= 0.005, <0.001, <0.001) (Figures 1–3; Scatter plots with agreement line and best fit line).
Figure 1. Pre-op correlation between iHgb and nHgb.

Figure 2. PACU correlation between iHgb and nHgb.
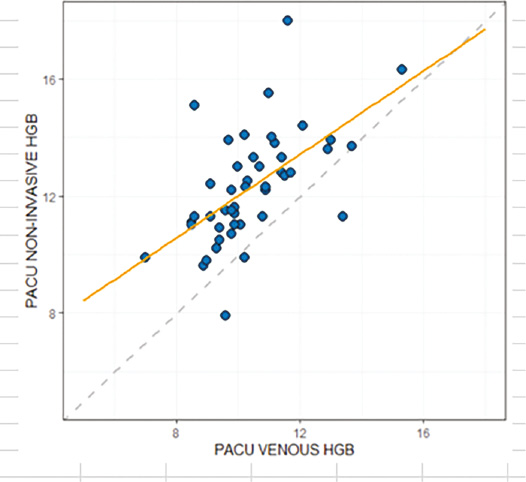
Figure 3. POD 1 correlation between iHgb and nHgb.
At all three time points, the mean nHgb value was 1-2 g/dL higher than the mean iHgb value, and this was statistically significant (Table 2).
Table 2. Mean Invasive and Noninvasive Hgb Values at Collection Time Points
| N | Mean | SD | P-value | ||
|---|---|---|---|---|---|
| Pre | PRE-OP VENOUS HGB | 60 | 13.527 | 1.1235 | <0.0001 |
| PRE-OP NON-INVASIVE HGB | 60 | 14.284 | 1.3656 | ||
| PACU | PACU VENOUS HGB | 60 | 10.500 | 1.4833 | <0.0001 |
| PACU NON-INVASIVE HGB | 60 | 12.571 | 1.7257 | ||
| Post-Op | POST-OP VENOUS HGB | 60 | 10.105 | 1.3560 | <0.0001 |
| POST-OP NON-INVASIVE HGB | 60 | 11.902 | 1.4790 |
Guidelines for an Allogenic Blood Transfusion (ABT) at our institution were developed by consensus between the surgical and anesthesia teams. Indications for a postoperative ABT include: iHgb 7.0 – 8.0 g/dL along with clinical signs of anemia such as persistent hypotension, tachycardia, dyspnea, lethargy, confusion, postural dizziness not responsive to a fluid challenge, or iHgb <7.0 g/dL, regardless of signs/symptoms of anemia.
At 0700 on POD 1, a patient with a nHgb value of ≥10.8 g/dL had an iHgb value of ≥9.0 g/dL with 87% sensitivity (Figure 4).
Figure 4. nHgb value of ≥10.8 g/dL had an iHgb value of >9.0 g/dL with 87% sensitivity.

We chose iHgb ≥9.0g/dL as the threshold because 54/60 had a lab value within that range at 0700 on POD 1, whereas only 6 of the 60 patients had an iHgb ≤8.0 g/dL.
We have performed PSFI on 66 additional AIS patients since implementing the nHgb threshold of 10.8g/dL. Because of the 10.8 g/dL threshold, only 10/66 (15%) of these AIS surgical patients required a venipuncture during their postoperative recovery. The average postoperative hgb on these 10 patients was 9.75 g/dL (8.3-12.8) g/dL. None required an allogenic blood transfusion.
Discussion
Many standardized postoperative care pathways for patients undergoing posterior spinal fusion (PSF) for adolescent idiopathic scoliosis (AIS) have been published.5–8 A key feature of these pathways is a multimodal approach to pain control. The fear of needles is a challenging and common condition among children and adolescents.1 Blood draw-related anxiety and pain associated with the venipuncture has not been addressed by these previously published standardized postoperative AIS care pathways.
Literature from our total joint arthroplasty colleagues has demonstrated that noninvasive hemoglobin (nHgb) monitoring is more efficient, less expensive, and preferred by patients compared to invasive hemoglobin (iHgb) monitoring. In their report, 100% of patients with a nHgb value ≥10.5 g/dL had a iHgb >8.0 g/dL3.
This is the first project to address the use of nHgb monitoring in an AIS population. Previous articles have been published on its use in pediatric neurosurgical patients and congenital heart disease patients.9,10 Unfortunately, in those surgical pediatric populations, nHgb was not reliable and could not guide ABT decision-making. Those studies focused on much younger patient populations (average ages 6.34 and 1.5 years) and more medically complex patients.
The surgical AIS patient population is older and more homogenous in nature. Also, the patients tend to have no underlying medical conditions, making it an advantageous population to investigate the reliability of nHgb measurement. Our project demonstrated a moderate correlation between nHgb and venous Hgb at all three measurement time points.
Only 2/60 (3.3%) patients required a perioperative allogenic blood transfusion (ABT). Mange et al. previously reported that our institutions’ post-surgical AIS patients with a POD 1 venous Hgb ≥9.1g/dL were extremely unlikely to require a transfusion.4 Using this data, guidelines for an ABT were developed by consensus between our surgical and anesthesia teams. Postoperative ABT indication is an iHgb 7.0 – 8.0 g/dL along with clinical signs of anemia such as persistent hypotension, tachycardia, dyspnea, lethargy, confusion, postural dizziness not responsive to a fluid challenge, or iHgb <7.0 g/dL, regardless of signs/symptoms of anemia.
A limitation of this QI project was that there were not enough data points to correlate nHgb measurements with a patient receiving an ABT. Therefore, we focused on a nHgb threshold at which a postoperative blood draw would not be necessary. We chose venous Hgb (iHgb) of >9.0 g/dl based on the work from Mange et al. Therefore, at 0700 on POD 1, a patient with a nHgb value of ≥10.8 g/dL had an iHgb (venous) value of >9.0 g/dL with 87% sensitivity. This nHgb value would never require an ABT, therefore a venipuncture is unnecessary.
All spine surgeons and anesthesia staff agreed that new indication (trigger) for obtaining a postoperative venous Hgb would be an nHgb measurement of <10.8 g/dL. We performed PSFI on 66 additional AIS patients since implementing the nHgb threshold. Only 10/66 (15%) of these AIS surgical patients were below the 10.8 g/dL threshold on their nHgb and required a venipuncture during their postoperative recovery. The average postoperative venous Hgb on those 10 patients was 9.75 g/dL (8.3-12.8) g/dL. None of these patients required an ABT.
This study is confounded by evolution of our institutions’ indications for ABT in AIS patients after PSFI. Prior to the Mange at al. study,4 the decision and indications for ABT in postoperative AIS patients was driven by the attending surgeon. Following the Mange study, the consensus-based guidelines were developed. These guidelines have lowered our institutions ABT transfusion rate from 18.2% to its current rate of 2/126 (1.6%). A goal of “zero” ABT in this patient population is desirable and possibly obtainable. However, until that “zero” goal of is reached, then postoperative measurement of the patient’s Hgb is necessary.
Our standardized postoperative care pathway for AIS patients now includes the routine postoperative assessment of nHgb instead of routine blood draws.
Conclusions
Noninvasive Hgb monitoring was found to positively correlate with iHgb in AIS patients undergoing PSFI. At all three time points, a moderate correlation existed, and the mean nHgb value was 1-2 g/dL higher than the mean iHgb value. Surgeons could consider screening AIS patients postoperatively with nHgb monitoring and only order iHgb measurement if the nHgb value is <10.8 g/dL. Six months after instituting this nHgb threshold, only 15% (10/66) of our post-surgical AIS patients received a venipuncture.
Disclaimer
The authors report no conflicts of interest related to this manuscript.
References
- Orenius T, LicPsych, Säilä H, et al. Fear of injections and needle phobia among children and adolescents: an overview of psychological, behavioral, and contextual factors. SAGE Open Nurs. 2018;4.
- Patino M, Schultz L, Hossain M, et al. Trending and accuracy of noninvasive hemoglobin monitoring in pediatric perioperative patients. Anesth Analg. 2014;119(4):920-925.
- Martin JR, Camp CL, Stitz A, et al. Noninvasive hemoglobin monitoring: a rapid, reliable, and cost-effective method following total joint replacement. J Bone Joint Surg Am. 2016;98(5):349-355.
- Mange TR, Sucato DJ, Poppino KF, et al. The incidence and risk factors for perioperative allogeneic blood transfusion in primary idiopathic scoliosis surgery. Spine Deform. 2020;8(4):695-702.
- Oetgen ME, Martin BD, Gordish-Dressman H, et al. Effectiveness and sustainability of a standardized care pathway developed with use of lean processmapping for the treatment of patients undergoing posterior spinal fusion for adolescent idiopathic scoliosis. J Bone Joint Surg Am. 2018;100(21):1864-1870.
- Gornitzky AL, Flynn JM, Muhly WT, et al. A rapid recovery pathway for adolescent idiopathic scoliosis that improves pain control and reduces time to inpatient recovery after posterior spinal fusion. Spine Deform. 2016;4(4):288-295.
- Sanders AE, Andras LM, Sousa T, et al. Accelerated discharge protocol for posterior spinal fusion patients with adolescent idiopathic scoliosis decreases hospital postoperative charges. Spine (Phila Pa 1976). 2017;15(42):92-97.
- Yang J, Skaggs DL, Chan P, et al. High satisfaction in adolescent idiopathic scoliosis patients on enhanced discharge pathway. J Pediatr Orthop. 2020;40(3):e166-e170.
- Kamel MM, Hasanin A, Nawar B, et al. Evaluation of noninvasive hemoglobin monitoring in children with congenital heart diseases. Paediatr Anaesth. 2020;30(5):571-576.
- Park YH, Lee JH, Song HG, et al. The accuracy of noninvasive hemoglobin monitoring using the radical-7 pulse CO-Oximeter in children undergoing neurosurgery. Anesth Analg. 2012;115(6):1302-1307.