
Quality, Safety and Value (QSVI)
More Than Just Medication: Exploring the Potential of a Perioperative Psychosocial Intervention Following Major Pediatric Orthopaedic Surgery
1Department of Orthopaedic Surgery, University of Michigan, Ann Arbor, MI; 2Department of Orthopaedic Surgery, University of California, San Francisco, San Francisco, CA
Correspondence: Alex Gornitzky, MD, C.S. Mott Children’s Hospital, 1540 E. Hospital Dr., SPC 4241, Ann Arbor, MI 48109-4241. Email: [email protected]
Received: September 27, 2022; Accepted: February 13, 2023; Published: May 1, 2023
Volume 5, Number 2, May 2023
Abstract
Background: Although psychosocial factors such as anxiety, catastrophizing, and self-efficacy have been documented to affect postoperative pain, interventions to address these variables have been limited. Instead, most surgical care pathways only turn to alternative psychosocial strategies once traditional medication management has failed.
Local Problem: There is a strong family desire for a pain-related psychosocial intervention prior to major pediatric surgery. However, a variety of barriers including cost and accessibility have prevented the wider adoption of such protocols at many institutions.
Specific Aims: Using idiopathic scoliosis as a model, the purpose of this study was to assess the feasibility of a novel, web-based, perioperative psychosocial intervention focused on teaching healthy coping skills and improving pain self-efficacy.
Interventions: We built a comprehensive digital-health intervention consisting of 21 educational and coping skills videos delivered daily via smartphone for approximately 3 weeks throughout the perioperative period.
Measures and Analysis: The intervention was administered as part of a randomized, controlled trial to all patients undergoing spine surgery for idiopathic scoliosis at a single academic institution. Eligible procedures included posterior spinal instrumented fusion (PSIF) and anterior vertebral body tethering (AVBT). Families completed questionnaires focused on pain intensity, opioid consumption, pain-related disability, and patient-reported outcomes for the first 6 weeks after surgery.
Results: Forty patients were enrolled and randomized, of which 30 completed the questionnaires. The intervention did not have any quantitative effect on mean daily pain scores, opioid consumption, or patient-reported outcomes. Nevertheless, the majority of families rated the coping skills videos as helpful, and 100% of respondents were likely or very likely to recommend practicing these skills to future patients. Qualitative feedback suggested that participants perceived the intervention as a simple and effective way to practice guided alternative pain management tactics that they would not otherwise have access to.
Conclusion: Psychosocial interventions targeting pain following scoliosis surgery are both feasible and well-received. Additional research is needed to further develop these pathways and rigorously assess their impact on patient outcomes.
Level of Evidence: Therapeutic Level II
Introduction
For children undergoing major pediatric orthopaedic surgery, postoperative pain can have a substantial deleterious impact on functional, psychological, and social well-being.1–7 From a psychosocial perspective, children’s confidence in their ability to control pain predicts a more rapid postoperative improvement, while perceived helplessness may lead to reduced pain tolerance, higher pain intensity, and greater pain-related disability.1,5,8–15 Parents’ actions around the time of surgery can also influence their child’s opioid consumption and long-term pain intensity.5,16–20
A major limitation in the field of pediatric orthopaedic surgery is a paucity of data on methods to address the psychosocial elements of pain. In particular, qualitative studies have documented a strong family desire for a pain-related psychosocial intervention prior to major pediatric surgery.13 Nevertheless, such psychosocial tactics have not been widely integrated into most modern perioperative pathways. Instead, they are typically utilized only when traditional medication management has failed.21
Available Knowledge
Early studies have demonstrated the potential impact of brief education and coping skills interventions on pain control and patient satisfaction following pediatric orthopaedic surgery. In-person evaluation and treatment with a psychologist led to improved outcomes and earlier return to function in adolescents undergoing hip preservation surgery.22 Considering a more widely accessible solution, LaMontange and colleagues found that a combined informational and coping skills intervention delivered one time via videotape was effective for limiting anxiety and reducing pain in adolescents undergoing spine surgery.7,23,24 Similarly, a combined video intervention consisting of information and guided imagery/relaxation exercises screened three times around the time of surgery improved pain and reduced interference of pain with daily activities in a Canadian spinal fusion cohort.25 Highlighting the value of this combined approach, Rhodes et al. found that education alone without concomitant coping skills might actually increase post-operative anxiety and distress without affecting length of stay or opioid consumption.6 Putting this all together, a recent web-based comprehensive psychosocial intervention in spinal fusion patients was shown to be both feasible and well-received by families.26
Looking beyond pediatric orthopaedics, web-based interventions across other subspecialties are effective at reducing perioperative anxiety.27 For children with chronic pain, a structured, skills-based group intervention resulted in both parent and adolescent improvements in function and pain management.28 Similarly, a web-based psychological intervention improved outcomes for children with chronic pain, although efficacy was strongly correlated with engagement.29 Finally, a recent meta-analysis looking at children’s pain after surgery showed distraction and imagery techniques to be the most effective tools for reducing short-term, self-reported pain.30
Local Problem & Rationale
Consistent with best practice,31–33 our institution utilizes a standardized multimodal analgesic platform as part of a multidisciplinary enhanced recovery pathway following pediatric spinal surgery. In order to address the unmet psychosocial needs of our patients, we began exploring alternative strategies to augment perioperative education and pain management. Although our institution had a successful and well-established pain psychology program, they unfortunately did not have the bandwidth to expand resources to elective orthopaedic procedures. At the same time, our orthopaedic staff had neither the time nor the psychological expertise to take on these additional responsibilities themselves. Therefore, with guidance from our psychology colleagues, we began exploring alternative strategies to address this deficit. A digital health tool was desired to maximize access, manage costs, and minimize additional resource burden.
Specific Aim
Using idiopathic scoliosis as a model, this study evaluated a novel, internet-based perioperative psychosocial intervention focused on coping skills and expanded family education. Our goals were to 1) determine feasibility of the intervention in a representative patient cohort; 2) collect qualitative feedback on families’ perceptions surrounding the intervention; and 3) measure the intervention’s impact on pain, opioid consumption, and patient-reported outcomes for the first 6 weeks following surgery.
Methods
Context
Consistent with best practice, all patients treated with spinal fusion for idiopathic scoliosis at our institution are enrolled in a standardized recovery pathway. This includes routine preoperative surgical education and a comprehensive multimodal analgesic platform starting preoperatively and proceeding until discharge. The acute pain service co-manages all patients until their patient-controlled analgesia device is discontinued. Physical therapy begins immediately and proceeds through a defined series of time-based goals. Child life and music therapists are also available, but these services are a general hospital-wide resource, and there is no specific pathway for spinal fusion patients. No additional psychosocial resources, including coping skills training, are available or provided either in the preoperative or postoperative period. Even if a child or family is subjectively identified by the provider team as being high-risk for poorly controlled pain, our institution did not have a clear set of resources to connect these patients with.
Intervention
First, a systematic review of the literature was completed to construct a checklist for the ideal psychosocial intervention (Figure 1).34 The intervention was then designed through a multidisciplinary collaboration between orthopaedics, anesthesia, pain psychology, child life therapy, physical therapy, music therapy, and advanced practice providers. Former patient feedback was solicited and incorporated.
Figure 1. Psychosocial intervention checklist for children & adolescents. Adapted from Gornitzky et al., JPOSNA® Feb 2021.

Next, the intervention was built in a structured manner. First, a topic was selected for each video in the series. There were 21 videos included in the final intervention (Table 1). Next, a script was developed for each video with input from relevant members of the multidisciplinary team. Input from the pain psychology and child life therapy teams were prioritized in terms of maximizing potential efficacy of each video. Additionally, each script and the intervention as a whole were then cross-checked against our original checklist in order to ensure the intervention remained true to our initial goals. There were four videos of former patients/parents offering unscripted advice following generic prompts (e.g., What was the most challenging part of recovery?). Each segment was then filmed using a setup consisting of a smartphone, tripod, and portable microphone (total cost less than $50, excluding the smartphone). All videos were filmed and edited in-house by the primary author using widely available consumer software (iMovie). Goal length for each video was approximately 5 minutes. This author had no prior video recording/editing experience, which was consistent with our goals to create a process that could be easily replicated at other institutions with limited available budgets.
Table 1. List of Video Topics for Perioperative Psychosocial Intervention
| Order | Title | Type | Delivery Timeline |
|---|---|---|---|
| 1 | Hospital Tour | Education | Pre |
| 2 | Getting Ready for Surgery: What to Expect # | Education | Pre |
| 3 | Patient Stories: Getting Ready for Surgery ⊕ | Education | Pre |
| 4 | Getting Ready for Surgery: Talking About Pain # | Education | Pre |
| 5 | Introduction to Coping Skills * | Coping | Pre |
| 6 | Patient Stories: Staying in the Hospital ⊕ | Education | Pre |
| 7 | Parent-to-Parent Advice ⊕ | Education | Pre |
| 8 | Physical Therapy | Education | Post |
| 9 | Breathing Techniques #1: Belly Breathing * | Coping | Post |
| 10 | Guided Imagery #1: Beach Visualization * | Coping | Post |
| 11 | Getting Ready for Discharge # | Education | Post |
| 12 | Breathing Techniques #2: Guided Breathing * | Coping | Post |
| 13 | Patient Stories: Recovery from Surgery at Home ⊕ | Education | Post |
| 14 | Progressive Muscle Relaxation #1 * | Coping | Post |
| 15 | Music Therapy * | Coping | Post |
| 16 | Guided Imagery #2 * | Coping | Post |
| 17 | Breathing Techniques #3: Mindful Breathing * | Coping | Post |
| 18 | Guided Imagery #3: Pain Reduction Visualization * | Coping | Post |
| 19 | Progressive Muscle Relaxation #2 * | Coping | Post |
| 20 | Breathing Techniques #4: Breathing to Sound * | Coping | Post |
| 21 | Guided Imagery #4: Waterfall Visualization * | Coping | Post |
# = Provider-based educational video.
⊕ = Subseries featuring unscripted peer advice and stories from former patients and their parents.
* = Core coping skills videos.
The videos were primarily educational before surgery (n=7) and skill-focused after surgery (n=14).23,24 The Redcap research platform was selected for patient interface to ensure compliance with all institutional research and privacy standards. Additionally, the integrated automated survey invitation capabilities facilitated easy text messaging of surveys and video links directly to patients, which achieved our goal of maximizing access without needing a custom-built smartphone app. This approach was chosen to ensure a cheap and accessible methodology that could easily be replicated at other institutions without a significant financial investment. The entire process, from video planning through final editing, took approximately 1 year to complete. Financial support was only utilized to incentivize survey completion.
The length of each video was approximately 5 minutes. A link was delivered daily via text message to the participant’s (or their parent’s) cell phone. As a result, participants always had a readily available description to previous videos directly accessible in their chat thread to facilitate additional practice as needed. Videos were hosted on a familiar internet platform (YouTube) to maximize relatability and utility. Each was hosted on a private channel (videos could only be accessed via shared link and are not visible on search).
By providing comprehensive and detailed preparatory information on what to expect through the entirety of the perioperative period, the educational videos were intended to set expectations, ease anxiety, and prevent catastrophizing. This section included both provider-guided videos and unscripted advice from former patients. The skill-based videos were designed to encourage the child’s confidence around self-directed coping strategies. Each video demonstrated a specific coping skill (e.g., deep breathing, progressive muscle relaxation, guided imagery). There was repetition of each skill to reinforce the technique and promote further skill development. Participants were encouraged to focus their practice on those skills that resonated most strongly with them.
Study of the Intervention
The intervention was then delivered as part of a randomized, controlled trial (NCT04063670) at a single academic institution. Consecutive children aged 11 to 18 treated with primary multilevel spinal surgery for idiopathic scoliosis by the senior author from May 2019 through April 2021 were eligible. Eligible procedures included posterior spinal instrumented fusion (PSIF) and anterior vertebral body tethering (AVBT). Exclusion criteria included non-idiopathic scoliosis, history of chronic pain/opioid use, active psychotherapy, and non-English speaking (English-only surveys and videos), and unplanned re-admission or return to the operating room within 6 weeks of their index procedure. Participants were randomized at the time of enrollment based upon an a priori computer-generated random number chart. The first seven videos were delivered en-bloc approximately 1–2 weeks prior to operation (Table 1). A single reminder was sent 24 hours after the initial delivery to remind families to watch the videos. The remaining 14 postoperative videos were delivered one per day, beginning on the morning after the procedure (new video received each day POD 1-14). All videos remained open and accessible throughout the study period so participants were free go back and watch previous videos as often as they would like.
The initial power analysis suggested approximately 50 patients per group. The trial was ended early due to logistical reasons. Specifically, the first author graduated from residency, and there was no further research coordinator support for ongoing study recruitment and administration. COVID-19-related decreases in patient volume also adversely affected potential enrollment during this time. Therefore, the initial goal sample size was not met. The intervention was not changed or modified in any way throughout the course of the trial.
Measures
Clinical outcomes were assessed for the first 6 weeks after operation. Daily pain scores were collected once per day for the first 4 weeks and weekly thereafter. Opioid consumption and pain self-efficacy were queried weekly. The NIH’s Patient Reported Outcomes Measurement Information System (PROMIS®) pain-related tools (Pain Behavior and Pain Interference) were measured at 1, 2, and 6 weeks. These scales are well-validated across a variety of orthopaedic populations, compare well with legacy measures, and have a mean score of 50 with a minimum clinically significant difference of 3.35,36 Global satisfaction with pain management and overall treatment was gauged at 2 and 6 weeks. Time to key milestone completion (such as independent completion of activities of daily living [ADL] without assistance and sleeping through the night without waking for analgesics) was evaluated weekly. Ambulatory capacity (PROMIS Mobility) was assessed at 1, 2, and 6 weeks. Psychosocial health (PROMIS Anxiety, PROMIS Positive Affect) and health-related quality-of-life (PROMIS Global) were measured at 2 and 6 weeks after operation. Each PROMIS measure was also collected before operation to provide an individual baseline. All PROMIS scores were measured by computer adaptive testing. Participants randomized to the intervention were asked whether they had watched (and practiced) the previous day’s coping skills video. These patients also completed an optional qualitative survey at the end of the study asking which coping skills they found helpful and which they would recommend to future patients.
Analysis
The primary study objective was to determine the intervention’s impact on pain intensity and pain interference at 2 and 6 weeks postoperatively. Secondary objectives included a qualitative assessment of how families appreciated the intervention. Statistical analysis was completed through an intention-to-treat model. There was insufficient power for an as-treated analysis (accounting for those in the video group who did not watch the videos). Descriptive statistics were generated for demographic variables. Continuous variables were then analyzed using the Student t-test or the Mann-Whitney U test. Paired analyses were completed to compare change in outcome measures over time. Categorical variables were compared using the chi-square tests. Categorical variables are reported as frequency and percentage; continuous variables are presented with a measure of central tendency (mean or median) and spread (SD or range). All comparative analyses were 2-tailed with alpha set at 0.05.
Ethical Considerations
Institutional review board approval was obtained prior to commencement. All patients in both study arms were treated with the same standardized clinical pathway, and all clinical providers were blinded to study participation at all times. Study enrollment, randomization, and survey distribution/collection were completed by the primary author, who was not directly involved in the clinical care of any patients. Therefore, as the primary intervention was a supplementary, unproven video series, the authors do not feel there were any significant ethical implications of study participation.
Results
There were 31 patients in the final analysis, including 16 in the intervention group (Figure 2). The mean age was 13.7 years old, and 90% (37/41) were females (Table 2). There was no difference between the cohorts in type of surgery (p=0.80) or number of levels treated (p=0.13).
Figure 2. Flow chart for evaluation, exclusion, randomization, and final enrollment of patients.

Table 2. Demographics
| Category | Total Cohort | Control Group | Video Intervention | p-value |
|---|---|---|---|---|
| Number | 31 | 15 | 16 | |
| Age, years | 13.7 | 13.7 | 13.8 | 0.89 |
| Gender, % female | 90 | 93 | 88 | 0.60 |
| Grade in school | 8.6 | 8.4 | 8.9 | 0.43 |
| Race, % Caucasian | 61 | 47 | 75 | 0.11 |
| Ethnicity, % non-Hispanic | 77 | 73 | 81 | 0.70 |
| Levels fused | 9 | 10 | 8 | 0.13 |
| • Most common UIV | T3 (n=8) | T3 (n=7) | ||
| • Most common LIV | L4 (n=6) | L4 (n=7) | ||
| Type of surgery | 0.80 | |||
| • Fusion, % | 71 | 73 | 69 | |
| • Tether, % | 29 | 27 | 31 |
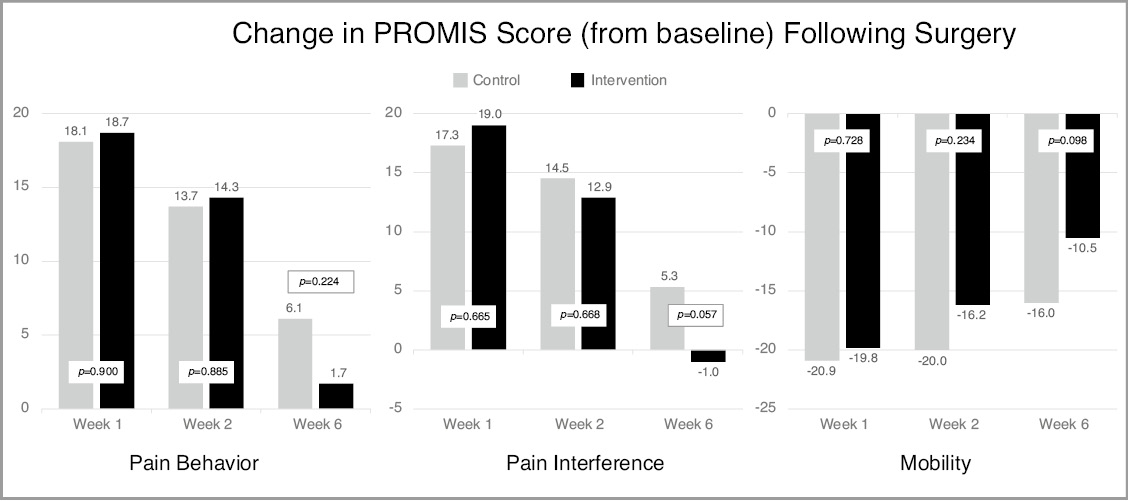
The intervention did not have a measurable effect on postoperative pain. Average daily pain scores in the intervention group mirrored those of the control group (Figure 3). There was no change in either opioid consumption or pain self-efficacy. Finally, there was no statistically significant differences in terms of time-to-milestone completion (e.g., independent completion of ADLs) or patient-reported outcomes as measured via change in PROMIS pain behavior, pain interference, mobility, or global health (all p>0.05; Figure 4). Additional PROMIS domains that were not significantly affected by the intervention included anxiety, positive affect, physical activity, and strength impact. Both groups were equally satisfied with their care 6 weeks after operation (79% very satisfied).
Figure 3. Average daily pain score following surgery. Patient’s response to the prompt: “On a scale of 0 to 10, with 0 being no pain and 10 being the worst pain imaginable, which one of the following best describes the average amount of pain you have experienced over the past day while doing activity (for example walking)?” Pain scores were collected once per day for the first 4 weeks (and averaged) and then weekly thereafter.

Figure 4. Change in PROMIS score from baseline until surgery. Higher PROMIS scores represent more of the category being measured. As such, positive change between two timepoints indicates an increase in that variable (i.e., more pain interference), while negative change between two timepoints indicates a decrease in that variable (i.e., less mobility). Values closer to zero represent a smaller change from baseline in response to surgery. Each bar is depicted with the specific PROMIS score as well as the p-value for the associated comparative analysis between groups. Comparative analyses demonstrated no statistically significant differences between groups at any timepoint.
Of those assigned to the video intervention, 56% (9/16) completed the optional qualitative survey at the end. Representative feedback is included in Table 3. Of the five queried coping skills, 100% of participants found at least one skill helpful, and all of the participants said they were either likely or very likely to recommend at least two of the coping skills to future patients. In terms of helpfulness, the most highly rated skills were belly breathing (100%), distraction (67%), and music therapy (56%). Patients found the pain visualization and progressive muscle relaxation exercises to be the least helpful (33% each). Mirroring these findings, the most recommended skills were belly breathing (100%), distraction (78%), music therapy (67%), and pain visualization exercises (56%).
Table 3. Representative Qualitative Feedback on Psychosocial Intervention
| Prompt: What did you like about the intervention? |
|---|
| • “It was helpful to remind me that I should keep trying to tolerate pain and it worked” |
| • “I enjoyed the visuals” |
| • “I liked how I was guided on how to focus on things other than my pain” |
| • “It was a great way to keep focused on controlling pain” |
| • “I enjoyed the step-by-step nature the video was presented in since it helped me follow along” |
| • “It was calming and easy to go through the steps” |
| • “It gave me a lot of different methods to choose from that I wouldn't typically know to use” |
Discussion
Driven by the opioid epidemic, there has been an increased focus on pain management and opioid prescribing practices in the pediatric orthopaedic population.37–39 Much effort has focused on the development of enhanced recovery pathways31,32,40,41 and/or limiting the number of opioids prescribed at discharge.42–45 Other work has highlighted the value of expanded patient and family education.33 In recognition of pain as a complex biopsychosocial condition, a more comprehensive approach to pain management would include psychosocial strategies from the outset to equip patients with the skills to better control their pain experience.21,46 The goal of this study was to design and test a novel perioperative psychosocial intervention in kids focused on building resiliency and teaching healthy coping skills. By developing a web-based intervention, we sought to create an accessible solution that could be easily expanded to other procedures and institutions in the future.
In this pilot study, the video intervention did not have any statistically significant effect on pain-related outcomes, including change in PROMIS scores from preoperative baselines (pain interference and pain behavior), opioid consumption, or pain self-efficacy. There was also no difference in overall satisfaction with treatment. Nevertheless, qualitative comments suggested that the families found the intervention to be helpful, and all of the patients were either likely or very likely to recommend practicing the demonstrated coping skills to future patients.
Interpretation
Overall, these findings highlight the value of these psychosocial interventions to families. While further work needs to be done to optimize the quantitative impact of such interventions, it is less likely that subjective feedback would be so universally positive if the intervention was not fulfilling an unmet need. More likely, as discussed further below, this study was limited by low numbers and inconsistent engagement with the video intervention. Further work will be needed to assess this intervention across larger patient cohorts and develop improved methodology to enhance patient engagement.
One challenge in creating psychosocial interventions is to design a resource that is both relevant and useful. This is particularly true for many orthopaedic surgeons who may have limited knowledge and experience with the biopsychosocial model of pain control. Using the work of Rabbitts and colleagues as a roadmap,13 a checklist was created in order to guide construction of this psychosocial intervention.16,34,38 Novel elements included both a parental-focused segment and a video subseries featuring unscripted peer advice. Building upon previous interventions that included only a single skill delivered a limited number of times in the immediate perioperative period, we designed this intervention to include many different skills delivered multiple times each. Issues of access were addressed by sending the videos in a familiar and age-appropriate fashion. Delivery was spread over the first 2 weeks after operation as families had noted the at-home recovery period to be among the most challenging in terms of regaining physical function and returning to normal activities. These innovations were intended to improve engagement and reinforce skill development through repetition in the home environment. Future modifications to this protocol should include earlier implementation, as recent work has identified psychological treatment beginning at least 2 months prior to surgery to be more effective than efforts begun closer to the procedure.15
Patient engagement was a significant challenge throughout the study, and future work in this space would likely benefit from improved methodology. Specifically, we were unable to account for those patients randomized to the intervention group who did not reliably watch the videos and practice the skills. On one hand, families were directly queried in the daily survey (for the first 14 days postoperatively) whether they had watched (and practiced) the previous day’s coping skills video. The majority (>75%) typically responded “Yes.” On the other hand, video tracking software embedded into YouTube suggested that many videos were not being watched consistently (or at all) during the time-period that families were answering “Yes.” However, this data is only available in aggregate and only for those videos directly created by the authors (all of the preoperative videos; 50% of the postoperative videos). Given these significant discrepancies between self-reported engagement and viewership metrics provided by the content platform, it is challenging to accurately determine true engagement. Looking at broader trends, engagement was highest for the preoperative videos. Links to the preoperative videos were sent en-bloc, and for each patient enrolled, there was a large and consistent spike in viewership for the first 24-48 hours after enrollment. Engagement for the postoperative videos was highest around days 3-5 after surgery but was otherwise quite limited throughout the post-operative period. In the setting of limited power, the authors felt that performing an as-treated analysis would not be statistically appropriate. There were likely many contributing factors to this engagement challenge. First, there were a lot of videos. Second, many families elected for the daily links and surveys to be sent to the parent’s cell phone. While this significantly improved the rate of survey completion, it may have compromised adolescent viewership. Future iterations would likely benefit from an app-based delivery that allows simultaneous delivery to multiple phones while also accurately tracking video engagement at the individual level. Additional considerations would be decreasing the total number of videos (to focus engagement on a few high-yield videos) or sharing access to the entire library of videos all at once so that families can peruse at their leisure. Future work in this space will hopefully help to optimize these methodological challenges.
Given the positive reception by patients and families, we believe that such pathways warrant further investigation. As many institutions already have well-developed informational packets and/or preoperative educational pathways for their most common procedures, one avenue might be to supplement these pre-existing educational efforts with an additional coping skills module. The skill-based videos in this intervention were intentionally designed to be generic and applicable to any patient at any institution. Therefore, we have combined these videos into a generic coping skills intervention that can be provided to any family about to undergo major pediatric orthopaedic surgery (Figure 5). We hope this free and publicly available resource can serve as not only a valuable tool for families, but also the basis for future research. As shown in Table 2, this video series contains a single preoperative video (Introduction to Coping Skills) followed by 11 skill-focused videos. By forgoing surveys and sending the videos directly to the adolescent’s phone, we also hope that engagement will be improved.
Figure 5. QR code for free and easy-to-use coping skills intervention that can be provided to any patient at any institution undergoing major pediatric orthopaedic surgery.

The value of a broad, multidisciplinary team was also fundamental to the success of this study. Every provider offered a unique viewpoint and set of skills to offer the team. By having each subspecialty contribute their own videos, it drastically improved the relevance and relatability of the intervention and also helped to create an engaged provider community that could be leveraged for future quality-improvement projects. Given the dearth of established psychosocial support networks at many children’s hospitals, convening a team to evaluate available resources and develop such pathways could be a valuable first step towards enhancing surgical pathways.
Limitations
This study has many limitations. First, it was underpowered, as the study was ended early for logistical reasons prior to reaching target enrollment. Nevertheless, as proof-of-concept, we believe that this pilot study demonstrated that such an intervention was both feasible and well-received by patients and their families. Second, as described above, limited engagement likely effected efficacy of the video intervention. Third, per individual preference, a number of the families elected to have the videos and outcome surveys sent to the parent’s cell phone. This may have affected survey response accuracy, although multiple previous reports have confirmed the reliability of parent-proxy survey completion. It may have also limited adolescent access to the videos when they were not co-located with their parents. Our proposed generic intervention would forgo the surveys and send the videos directly to the adolescent’s phones, thus potentially improving patient engagement with the coping skills. Finally, the intervention was nonspecific and included both educational efforts and coping skills. Future efforts will be needed to determine which components are most effective for whom and for what procedure.
Conclusion
In conclusion, comprehensive psychosocial interventions like the one described in this study can serve as a framework for adoption and additional testing across other institutions and procedures. Such multidisciplinary pathways have the potential to significantly improve patient’s experiences following major surgery in children. By leveraging the experience of a multidisciplinary team, a widely available research database, and simple, consumer-friendly video editing software, we demonstrated that a perioperative psychosocial intervention is both feasible and well-received by families undergoing major pediatric orthopaedic surgery. Additional research is needed to optimize the intervention and assess its impact across a larger patient cohort.
Acknowledgement
The authors would like to thank Dr. Dennis Black and Benjamin Black for their help and guidance with statistical analysis. We would also like to thank Dr. Amber Borucki (Pediatric Anesthesia/Pain Medicine) and Dr. Cristina Benki (Pediatric Psychology) for their help and assistance with design and creation of the video intervention. Finally, we would like to thank Shannon Farrell (Orthopaedic PA-C), Tracy Curtis (Orthopaedic PA-C), Dede Cerutti (Orthopaedic RN), Jennifer Goldhammer (Music Therapist), Marc Kristensen (Physical Therapist), and Adrienne Smith (Child Life Specialist) for their assistance with creating and filming content for the intervention. Finally, we would like to extend our gratitude to Chelsea Pelayo for assistance with editing and producing the videos as well as to Carolyn Winslow and Helen Deming for voice-over work.
Additional Links
- The Role of Pain Psychology in Multidisciplinary Treatment of Children and Adolescents Suffering from Acute and/or Chronic Pain Conditions, Cristina Benki, PhD, Assistant Clinical Professor and Licensed Clinical Psychologist at UCSF Benioff Children’s Hospital. Child and Adolescent Psychiatry Grand Rounds, March 2021.
- Long-Term Pain and Recovery After Major Pediatric Surgery: A Qualitative Study with Teens, Parents, and Perioperative Care Providers. Rabbitts et al., The Journal of Pain, 2017;18(7): 778-786. Helps to establish the need for psychosocial interventions around major pediatric orthopaedic surgery.
- Coping Skills in Children, Gornitzky and Diab, 2021. JPOSNA® Current Concept Review, details the evidence behind coping skills interventions in children.
Disclaimer
This project was financially supported by a resident research fund from the Department of Orthopaedic Surgery at the University of California, San Francisco. The authors report no conflicts of interest related to this manuscript.
References
- Connelly M, Fulmer RD, Prohaska J, et al. Predictors of postoperative pain trajectories in adolescent idiopathic scoliosis. Spine. 2014;39(3):E174-E181.
- Landman Z, Oswald T, Sanders J, et al. Prevalence and predictors of pain in surgical treatment of adolescent idiopathic scoliosis. Spine. 2011;36(10):825-829.
- Wong GT, Yuen VM, Chow BF, et al. Persistent pain in patients following scoliosis surgery. Eur Spine J. 2007;16(10):1551-1556.
- Gauntlett-Gilbert J, Eccleston C. Disability in adolescents with chronic pain: patterns and predictors across different domains of functioning. Pain. 2007;131(1-2):132-141.
- Rabbitts JA, Zhou C, Groenewald CB, et al. Trajectories of postsurgical pain in children: risk factors and impact of late pain recovery on long-term health outcomes after major surgery. Pain. 2015;156(11):2383-2389.
- Rhodes L, Nash C, Moisan A, et al. Does preoperative orientation and education alleviate anxiety in posterior spinal fusion patients? A prospective, randomized study. J Pediatr Orthop. 2015;35(3):276-279.
- LaMontagne LL, Hepworth JT, Cohen F, et al. Adolescent scoliosis: effects of corrective surgery, cognitive-behavioral interventions, and age on activity outcomes. Appl Nurs Res. 2004;17(3):168-177.
- Chidambaran V, Ding L, Moore DL, et al. Predicting the pain continuum after adolescent idiopathic scoliosis surgery: a prospective cohort study. Eur J Pain (London, England). 2017;21(7):1252-1265.
- Page MG, Stinson J, Campbell F, et al. Identification of pain-related psychological risk factors for the development and maintenance of pediatric chronic postsurgical pain. J Pain Res. 2013;6:167-180.
- Lamontagne LL, Hepworth JT, Salisbury MH. Anxiety and postoperative pain in children who undergo major orthopedic surgery. Appl Nurs Res. 2001;14(3):119-124.
- Kain ZN, Mayes LC, Caldwell-Andrews AA, et al. Preoperative anxiety, postoperative pain, and behavioral recovery in young children undergoing surgery. Pediatrics. 2006;118(2):651-658.
- Vervoort T, Eccleston C, Goubert L, et al. Children’s catastrophic thinking about their pain predicts pain and disability 6 months later. Eur J Pain (London, England). 2010;14(1):90-96.
- Rabbitts JA, Aaron RV, Fisher E, et al. Long-term pain and recovery after major pediatric surgery: a qualitative study with teens, parents, and perioperative care providers. The journal of pain. 2017;18(7):778-786.
- Yang S, Werner BC. Risk factors for prolonged postoperative opioid use after spinal fusion for adolescent idiopathic scoliosis. J Pediatr Orthop. 2019;39(10):500-504.
- Richard HM, Cerza SP, De La Rocha A, et al. Preoperative mental health status is a significant predictor of postoperative outcomes in adolescents treated with hip preservation surgery. J Child.’s Orthop. 2020;14(4):259-265.
- Guite JW, McCue RL, Sherker JL, et al. Relationships among pain, protective parental responses, and disability for adolescents with chronic musculoskeletal pain: the mediating role of pain catastrophizing. Clin J Pain. 2011;27(9):775-781.
- Page MG, Campbell F, Isaac L, et al. Parental risk factors for the development of pediatric acute and chronic postsurgical pain: a longitudinal study. J Pain Res. 2013;6:727-741.
- Goubert L, Eccleston C, Vervoort T, et al. Parental catastrophizing about their child’s pain. The parent version of the Pain Catastrophizing Scale (PCS-P): a preliminary validation. Pain. 2006;123(3):254-263.
- Caes L, Vervoort T, Eccleston C, et al. Parental catastrophizing about child’s pain and its relationship with activity restriction: the mediating role of parental distress. Pain. 2011;152(1):212-222.
- Sarkisova N, Andras LM, Yang J, et al. High parental anxiety increases narcotic use in adolescent patients following spinal fusion. J Pediatr Orthop. 2020;40(9):e794-e797.
- Darnall B. To treat pain, study people in all their complexity. Nature. 2018;557(7703):7.
- Richard HM, Nguyen DC, Podeszwa DA, et al. Perioperative interdisciplinary intervention contributes to improved outcomes of adolescents treated with hip preservation surgery. J Pediatr Orthop. 2018;38(5):254-259.
- LaMontagne LL, Hepworth JT, Cohen F, et al. Cognitive-behavioral intervention effects on adolescents’ anxiety and pain following spinal fusion surgery. Nurs Res. 2003;52(3):183-190.
- LaMontagne L, Hepworth JT, Salisbury MH, et al. Effects of coping instruction in reducing young adolescents’ pain after major spinal surgery. Orthop Nurs. 2003;22(6):398-403.
- Charette S, Fiola JL, Charest MC, et al. Guided imagery for adolescent post-spinal fusion pain management: a pilot study. Pain Manag Nurs. 2015;16(3):211-220.
- Murray CB, Bartlett A, Meyyappan A, et al. A pilot feasibility and acceptability study of an Internet-delivered psychosocial intervention to reduce postoperative pain in adolescents undergoing spinal fusion. Can J Pain. 2022;6(1):12-23.
- Fortier MA, Bunzli E, Walthall J, et al. Web-based tailored intervention for preparation of parents and children for outpatient surgery (WebTIPS): formative evaluation and randomized controlled trial. Anesth Analg. 2015;120(4):915-922.
- Coakley R, Wihak T, Kossowsky J, et al. The comfort ability pain management workshop: a preliminary, nonrandomized investigation of a brief, cognitive, biobehavioral, and parent training intervention for pediatric chronic pain. J Pediatr Psychol. 2018;43(3):252-265.
- Palermo TM, de la Vega R, Murray C, et al. A digital health psychological intervention (WebMAP Mobile) for children and adolescents with chronic pain: results of a hybrid effectiveness-implementation stepped-wedge cluster randomized trial. Pain. 2020;161(12):2763-2774.
- Davidson F, Snow S, Hayden JA, et al. Psychological interventions in managing postoperative pain in children: a systematic review. Pain. 2016;157(9):1872-1886.
- Gornitzky AL, Flynn JM, Muhly WT, et al. A rapid recovery pathway for adolescent idiopathic scoliosis that improves pain control and reduces time to inpatient recovery after posterior spinal fusion. Spine Deform. 2016;4(4):288-295.
- Fletcher ND, Glotzbecker MP, Marks M, et al. Development of consensus-based best practice guidelines for postoperative care following posterior spinal fusion for adolescent idiopathic scoliosis. Spine. 2017;42(9):E547-E554.
- Rao RR, Hayes M, Lewis C, et al. Mapping the road to recovery: shorter stays and satisfied patients in posterior spinal fusion. J Pediatr Orthop. 2017;37(8):e536-e542.
- Gornitzky AL, Diab M. Coping skills in children. JPOSNA. 2021;3(1):1-14.
- Okoroafor UC, Gerull W, Wright M, et al. The impact of social deprivation on pediatric PROMIS health scores after upper extremity fracture. J Hand Surg Am. 2018;43(10):897-902.
- Evans S, Okoroafor UC, Calfee RP. Is social deprivation associated with PROMIS outcomes after upper extremity fractures in children? Clin Orthop Relat Res. 2021;479(4):826-834.
- Johnson MA, Andras LM, Andras LE, et al. What’s new in pain management for pediatric orthopaedic surgery. J Pediatr Orthop. 2021;41(10):e923-e928.
- Rabbitts JA, Kain Z. Perioperative care for adolescents undergoing major surgery: a biopsychosocial conceptual framework. Anesth Analg. 2019;129(4):1181-1184.
- Rosenbloom BN, McCartney CJL, Canzian S, et al. Predictors of prescription opioid use 4 months after traumatic musculoskeletal injury and corrective surgery: a prospective study. J Pain. 2017;18(8):956-963.
- Muhly WT, Sankar WN, Ryan K, et al. Rapid recovery pathway after spinal fusion for idiopathic scoliosis. Pediatrics. 2016;137(4):e1-9.
- Fletcher ND, Andras LM, Lazarus DE, et al. Use of a novel pathway for early discharge was associated with a 48% shorter length of stay after posterior spinal fusion for adolescent idiopathic scoliosis. J Pediatr Orthop. 2017;37(2):92-97.
- Fang FY, Weir TB, Codd CM, et al. Discharge opioid prescribing patterns in an academic orthopaedic setting: level of training and subspecialty patterns. J Am Acad Orthop Surg. 2021;30(3):e361-e370.
- Nelson SE, Adams AJ, Buczek MJ, et al. Postoperative pain and opioid use in children with supracondylar humeral fractures: balancing analgesia and opioid stewardship. J Bone Joint Surg Am. 2019;101(2):119-126.
- Tepolt FA, Bido J, Burgess S, et al. Opioid overprescription after knee arthroscopy and related surgery in adolescents and young adults. Arthroscopy. 2018;34(12):3236-3243.
- Stillwagon MR, Feinstein S, Nichols B, et al. Pain control and medication use in children following closed reduction and percutaneous pinning of supracondylar humerus fractures: are we still overprescribing opioids? J Pediatr Orthop. 2020;40(10):543-548.
- Helmerhorst GT, Teunis T, Janssen SJ, et al. An epidemic of the use, misuse and overdose of opioids and deaths due to overdose, in the United States and Canada: is Europe next? Bone Joint J. 2017;99-B(7):856-864.