
Original Research
Single-Shot Versus Continuous Nerve Blocks for Pediatric Anterior Cruciate Ligament Reconstruction: Analgesic Efficacy and Postoperative Outcomes
1Division of Orthopaedics, Children’s Hospital of Philadelphia, Philadelphia, PA; 2Perelman School of Medicine at the University of Pennsylvania, Philadelphia, PA
Correspondence: Theodore J. Ganley, MD, Department of Orthopaedics, The Children’s Hospital of Philadelphia, 3401 Civic Center Blvd., Philadelphia, PA 19104. E-mail: [email protected]
Received: August 2, 2022; Accepted: January 12, 2023; Published: May 1, 2023
Volume 5, Number 2, May 2023
Abstract
Background: Regional anesthesia is often used to minimize postoperative pain, enable early mobilization, and improve patient/family satisfaction after ACL reconstruction. Little is known about the effects of nerve blocks on patient-reported outcomes and functional outcomes in pediatric ACL reconstruction. This study was performed to compare analgesic efficacy, isokinetic strength testing, and Patient-Reported Outcomes Measurement Information System (PROMIS) scores between single-shot femoral nerve block (SSNB) and femoral nerve catheter (FNC).
Methods: Pediatric patients (≤18 years old) who underwent primary ACL reconstruction at a tertiary care children’s hospital between January 2018 and August 2019 were included. Patients were grouped based on their anesthesia technique (SSNB or FNC) and compared to identify differences in the occurrence of uncontrolled postoperative pain and opioid refills. PROMIS domain scores, active range of motion (AROM), and isokinetic strength testing at multiple timepoints up to 6 months postoperatively were also collected. Linear regression multiple imputation analysis was performed to account for variable outcome measure availability.
Results: A total of 78 patients were included (SSNB:42; FNC:36). The groups had similar pain medication needs and pain scores at 1 week postoperatively. The FNC group had significantly longer in-room to incision times (P<0.001), were less likely to return to school by 1 week after surgery (P=0.03), and had lower mobility scores at the 1-week postoperative visit. Patients in the SSNB group had significantly weaker quadriceps function at 3 months (P=0.02), although this difference resolved by the 6-month visit. There were no cases of infection or neuropathy in either group.
Conclusion: Our findings indicate that both FNC and SSNB are viable options with similar efficacy for postoperative pain management in pediatric ACL reconstruction. However, we did not find any evidence of superior analgesia with FNC. Additionally, FNC was associated with lower PROMIS mobility scores at 1 week, delayed return to school, and 30 minutes of additional time spent in the operating room. There were no significant differences between groups in terms of function and PROMIS scores at 6 months postoperatively.
Level of Evidence: Level III, retrospective cohort study
Key Concepts
- Femoral nerve catheter and single-shot femoral blocks are both viable management options for post-ACL reconstruction pain in children and adolescents.
- We found that patients who received a femoral nerve block were less likely to return to school and had lower mobility scores at 1 week postoperatively and spent an additional 30 minutes in the operating room.
- Both regional anesthesia techniques had similar PROMIS scores and functional outcomes at 6 months postoperatively.
Introduction
The incidence of anterior cruciate ligament (ACL) injuries in the pediatric population has been steadily increasing.1,2 Despite the high incidence, there is still controversy regarding some aspects of treatment of ACL tears in children, especially in younger age groups. While injury prevention programs are effective in reducing the risk of ACL injury, patients under the age of 20 years currently comprise the largest subset of patients undergoing ACL reconstruction in the United States.2
Past work has shown that pediatric patients generally report higher levels of pain and anxiety postoperatively.3,4 Since nearly all ACL reconstructions in the United States are performed as outpatient procedures,2 adequate postoperative pain management is more challenging, especially in children and adolescents. Current rehabilitation protocols emphasize early range of motion (ROM) and mobilization to minimize complications and optimize long-term function, making postoperative pain control critical.
Regional anesthesia techniques are often used to provide postoperative pain management after ACL reconstruction. While several techniques exist, femoral nerve blocks, administered as either a single injection or with an indwelling catheter that provides continuous analgesia, are the most common postoperative pain control techniques reported in the literature.5,6 Although both techniques have proven to be safe and effective, there are drawbacks to each procedure. Femoral nerve catheters provide continuous pain control, but may restrict patients’ mobility, and there is also the risk of catheter-site leakage and infection. On the other hand, single-shot femoral nerve blocks are faster to administer but provide a shorter analgesic duration. Both techniques have also been associated with a measurable quadriceps motor deficit.7–11 Because of this, the use of adductor canal block, which has not been associated with significant quadriceps weakness, has been increasingly reported.7 Most studies of femoral nerve blocks have focused on adult patients, and the data on pediatric post-ACL reconstruction pain management is limited.
At our institution, the standard of care for perioperative pain management in pediatric patients undergoing ambulatory ACL reconstruction includes either femoral single-shot nerve blocks (SSNB) or femoral nerve catheters (FNC) at the discretion of the anesthesia team, each paired with a single-shot sciatic block. The purpose of this study was to evaluate the efficacy of pain control and muscle strength at follow-up for SSNB and FNC. We also sought to compare and report patient-reported outcomes for each modality at various intervals of postoperative follow-up. We hypothesized that both techniques will show comparable efficacy in pain management, but patients with FNC will have a longer time in the operating room.
Materials and Methods
This study was approved by our Institutional Review Board (IRB) and performed in compliance with Health Insurance Portability and Accountability Act (HIPAA) regulations. A retrospective review was conducted of all patients who underwent ACL reconstruction at our tertiary care children’s hospital and an associated satellite surgical center between January 2018 and August 2019. Individuals were identified using the current procedural terminology (CPT) code 29888. Patients ≤18 years old at the time of surgery who received any combination of regional anesthesia were selected from this database. Patients that underwent revision ACL surgery or had concomitant multi-ligamentous reconstruction (i.e., posterior cruciate ligament, medial collateral ligament, lateral collateral ligament) were excluded. We also excluded patients with missing isokinetic strength or patient-reported outcome scores at 3 and 6 months.
Patients receive a single-shot sciatic nerve block plus either femoral SSNB or FNC as dictated by the anesthesia service. However, at our institution, procedures performed at the main hospital campus typically receive an FNC, while patients at the satellite centers receive a SSNB. All operations were performed by five fellowship-trained pediatric sports medicine surgeons. Demographic data, including age at surgery, sex, and body mass index (BMI) were collected. In-room to incision time, graft type, reconstruction technique, as well as any meniscal injuries requiring concomitant treatment (i.e., meniscectomy or meniscus repair) were recorded from operative notes.12
Patients were contacted by the anesthesiology team on postoperative day 1 to follow-up on the pain levels and the status of the catheter (when applicable) and were provided with instructions on catheter removal. At the 1-week visit, patients were asked if they had returned to school, whether they had uncontrolled pain (as defined by the need for a phone call with the surgical team, opioid refill, or visiting an emergency department for pain). Opioid prescribing was at the discretion of the treating provider with roughly 3 days’ worth prescribed based on patient age and weight. All patients were routinely prescribed acetaminophen and ibuprofen unless there was a medical contraindication
Active knee range of motion (AROM) and isokinetic strength testing were recorded at 3 and 6 months postoperatively; the former was collected from the clinic visits with the attending surgeon and the latter from physical therapy appointment records. Strength testing consisted of five maximum effort repetitions at 180 degrees per second with gravity correction for limb weight. Isokinetic strength data was used to calculate the hamstrings to quadriceps (H/Q) ratio, defined as the ratio of the respective peak torque values normalized to body weight. Peak torque of the involved limb divided by the uninvolved limb was calculated and defined as the limb symmetry index (LSI).
Patient-reported outcomes were assessed using Patient-Reported Outcomes Measurement Information System (PROMIS) scores which had been collected as the standard of care at our institution for all ACL-injured patients throughout postoperative follow-up. PROMIS measures were recorded at 1 week, 6 weeks, 3 months, and 6 months after surgery. Given our study aims, we focused on the PROMIS domains of Physical Function – Mobility and Pain Interference. Operative complications, including postoperative wound issues, superficial skin infections, and arthrofibrosis requiring operative treatment within the first 6 months after surgery were recorded. Visit ranges for each time point were grouped based on the following cutoffs: 6 weeks = 30-59 days, 3 months = 60-120 days, and 6 months = 150-210 days.
We employed linear regression multiple imputation using age, gender, and graft type as predictors to minimize any bias in outcome variables from missed follow-up appointments.13 Five imputed datasets were created, and pooled estimates were calculated using Rubin’s rule.14 An a priori power analysis (G*Power 3.1) was done using a significance level of 0.05, power of 0.8, and standard deviation=15, which showed that a sample size of 36 patients in each group was required to detect a difference in PROMIS scores of 9.0 points at 3 or 6 months. Although there are no papers in the literature regarding PROMIS minimum clinically important difference (MCID) values in pediatric patients undergoing ACL reconstruction, similar studies in adults, as well as fracture studies, have suggested an MCID of 3.9 to 8.0, which was used for our power analysis.15–17 Continuous variables were then compared utilizing independent t-tests and Mann-Whitney U tests depending on normality of data, and categorical variables compared using Chi-squared and Fisher’s exact tests. All statistical analyses, assuming a significance threshold of p<0.05, were conducted using IBM SPSS Statistics for Windows, Version 24.0 (IBM Corp, Armonk, NY).
Results
A total of 78 patients met the inclusion criteria, with a mean age of 15.2 ± 2.2 years. Forty-two patients (54%) received SSNB and 36 received FNC (Figure 1). No differences were observed between groups in age (p=0.45), sex (p=0.52), BMI (p=0.11), delay to surgery (p=0.74), presence of a meniscus tear (p=0.34), or insurance type (p=0.36) (Table 1).
Figure 1. STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) diagram illustrating the patient selection process.
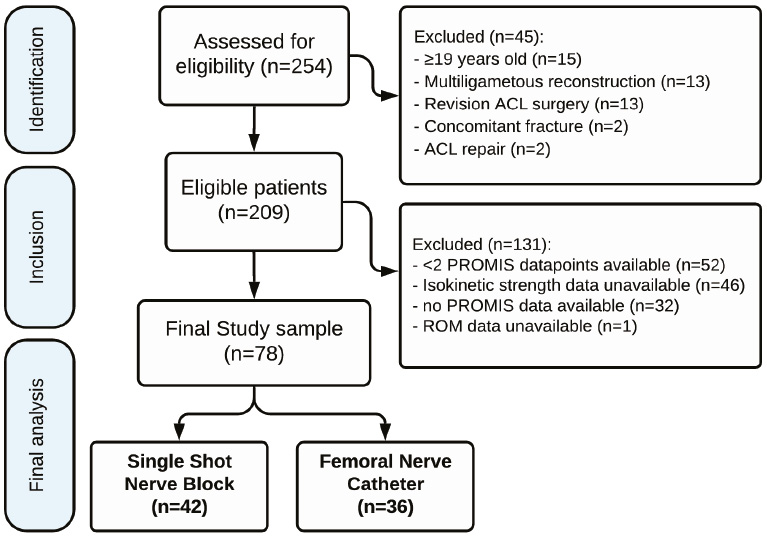
Table 1. Demographic and Injury Characteristics
| Variable | SSNB (N=42) | FNC (N=36) | P value |
|---|---|---|---|
| Age at Surgery (years) | 15.1 ± 2.4 | 15.4 ± 2.1 | 0.45 |
| Sex (M:F) | 18:24 | 18:18 | 0.52 |
| Body mass index (kg/m2) | 21.9 ± 3.7 | 24.2 ± 5.8 | 0.11 |
| Delay to Surgery (days) | 80.6 ± 88.4 | 93.6 ± 107.4 | 0.74 |
| Insurance Status | 0.36 | ||
| Private | 6 (14%) | 8 (22%) | |
| Public or Uninsured | 36 (86%) | 28 (78%) |
Values are presented as number (%) or mean ± SD. SSNB: single-shot nerve block, FNC: femoral nerve catheter.
Perioperative Period
The time from patients’ entry to the operating room to skin incision was significantly shorter in those undergoing SSNB by more than 30 minutes (P<0.001). In all patients, quadriceps autograft was the most common graft source for ACL reconstruction as was a transphyseal ACL reconstruction technique (Table 2). At the 1-week postoperative clinic visit, both groups had similar pain medication usage, including NSAIDs and opioids (p=0.31). No differences were observed in the rate of uncontrolled pain between groups which was measured by unplanned ED or clinic visits for pain, calls to provider for pain, and required opioid refills. Significantly fewer FNC patients returned to school at 1 week (11% vs 31% for SSNB) (P=0.03). No case of surgical site infection was recorded; however, three patients in each group experienced serosanguinous drainage from the surgical incisions during the first postoperative week, all of which resolved spontaneously (p=1). No cases of anesthesia-related complications were recorded, either intraoperative, postoperative, or catheter-related.
Table 2. Operative Variables and 1-Week Outcomes
| SSNB (N=42) | FNC (N=36) | P value | |
|---|---|---|---|
| Operative Times | |||
| In-Room to Skin Incision (min) | 50.1 ± 9.3 | 83.1 ± 13.5 | <0.001 |
| Surgical setting | <0.001 | ||
| Main hospital | 0 (0) | 35 (97) | |
| ASC | 42 (100) | 1 (3) | |
| Graft type | 0.78 | ||
| Quadriceps | 20 (48) | 19 (53) | |
| Hamstrings | 18 (43) | 15 (42) | |
| Other | 4 (9) | 2 (5) | |
| Meniscus Tear | 30 (71%) | 29 (81%) | 0.34 |
| Reconstruction technique | 0.43 | ||
| Transphyseal | 34 (81) | 32 (89) | |
| Partial Transphyseal | 4 (9.5) | 2 (5) | |
| All-Epiphyseal | 0 (0) | 1 (3) | |
| Extra/Intra-articular non-anatomic | 4 (9.5) | 1 (3) | |
| 1 week follow-up | |||
| Returned to school | 0.03 | ||
| Yes | 13 (31) | 4 (11) | |
| No | 16 (38) | 21 (58) | |
| Summer Month | 13 (31) | 11 (31) | |
| Taking any pain medication | 38 (91) | 32 (89) | 0.31 |
| NSAIDs/Acetaminophen | 28 (74) | 20 (62) | |
| Opioid | 10 (26) | 12 (38) | |
| Uncontrolled Pain | 4 (9.5) | 4 (11.1) | 1.0 |
| ED/Clinic Visit | 0 (0) | 1 (2.8) | 0.46 |
| Call | 4 (9.5) | 3 (8.3) | 1.0 |
| Required Opioid Refill | 2 (4.8) | 1 (2.8) | 1.0 |
| Wound drainage | 3 (7) | 3 (8) | 1.0 |
Values are presented as number (%) or mean ± SD. SSNB: Single-shot nerve block, FNC: femoral nerve catheter, NSAID: non-steroidal anti-inflammatory drug, ED: emergency department, ASC: Ambulatory surgery center. Significant comparisons are indicated in bold.
Outcomes
Patients with FNC had a significantly lower PROMIS physical function – mobility score at 1 week postoperatively compared to patients who received SSNB (p=0.009), while no differences were found at 6 weeks (P=0.13), 3 months (P=0.99), and 6 months (P=0.59). The PROMIS pain interference scores were similar at all timepoints (Table 3). Isokinetic strength data revealed a significantly higher hamstring to quadriceps ratio (H/Q) in the operative limb at 3 months postoperative (P=0.02), indicating a weaker quadriceps on the operated side. However, this comparison was not significant at 6 months (P=0.83). Other isokinetic strength comparisons, as well as active range of motion data, were similar between groups at all time points (Table 3). None of the patients required operative treatment for arthrofibrosis during the study period.
Table 3. Patient-Reported Outcomes, Isokinetic Strength, and Range of Motion Outcomes
| SSNB (N=42) | FNC (N=36) | P value | |
|---|---|---|---|
| PROMIS Scores | |||
| 1 week | |||
| Physical Function Mobility | 25.5 ± 5.6 | 22.1 ± 4.9 | 0.009 |
| Pain Interference | 54.5 ± 15.2 | 60.0 ± 10.0 | 0.17 |
| 6 weeks | |||
| Physical Function Mobility | 31.9 ± 4.5 | 29.6 ± 5.0 | 0.13 |
| Pain Interference | 50.9 ± 11.8 | 54.4 ± 11.7 | 0.38 |
| 3 months | |||
| Physical Function Mobility | 36.0 ± 7.0 | 36.0 ± 7.2 | 0.99 |
| Pain Interference | 39.9 ± 9.9 | 42.4 ± 11.3 | 0.44 |
| 6 months | |||
| Physical Function Mobility | 42.7 ± 8.7 | 41.4 ± 8.6 | 0.59 |
| Pain Interference | 41.2 ± 9.6 | 41.6 ± 11.9 | 0.90 |
| Isokinetic Strength (180 degrees/sec) | |||
| 3 months | |||
| Hamstring/Quadriceps Ratio (Involved Limb) | 77.4 ± 23.8 | 66.2 ± 18.0 | 0.02 |
| Hamstring/Quadriceps Ratio (Uninvolved Limb) | 57.3 ± 10.8 | 53.6 ± 9.9 | 0.12 |
| Limb symmetry index (Flexion) | 89.1 ± 19.0 | 87.2 ± 18.6 | 0.67 |
| Limb symmetry index (Extension) | 69.9 ± 21.7 | 72.5 ± 14.4 | 0.59 |
| 6 months | |||
| Hamstring/Quadriceps Ratio (Involved Limb) | 66.7 ± 17.3 | 68.0 ± 31.0 | 0.83 |
| Hamstring/Quadriceps Ratio (Uninvolved Limb) | 57.8 ± 12.6 | 52.7 ± 9.8 | 0.06 |
| Limb symmetry index (Flexion) | 97.0 ± 13.9 | 99.8 ± 21.3 | 0.54 |
| Limb symmetry index (Extension) | 84.6 ± 19.9 | 82.4 ± 18.3 | 0.64 |
| Active Range of Motion | |||
| 6 weeks | |||
| Extension | 0.8 ± 1.7 | 1.7 ± 2.9 | 0.11 |
| Flexion | 107.5 ± 19.1 | 105.5 ± 16.8 | 0.62 |
| 3 months | |||
| Extension | 0.5 ± 1.4 | 0.5 ± 1.3 | 0.78 |
| Flexion | 130.6 ± 9.6 | 128.2 ± 12.3 | 0.33 |
| 6 months | |||
| Extension | 0.3 ± 1.2 | 0.3 ± 0.8 | 0.76 |
| Flexion | 134.5 ± 5.8 | 132.8 ± 7.8 | 0.34 |
Values are presented as mean ± SD. PROMIS: patient-reported outcomes measurement information system. Significant comparisons are indicated in bold.
Discussion
Arthroscopic ACL reconstruction is increasingly performed in children and adolescents due to increased incidence and awareness, a better understanding of the long-term complications of a torn ACL, and the advent of safe, growth-friendly surgical techniques.18 An important challenge in outpatient ACL reconstruction is pain management. Regional anesthesia is a common strategy for postoperative pain management and is associated with a decreased need for opioid medications and emergency department visits, while also facilitating immediate postoperative mobilization and physical therapy.19–23 The purpose of this study was to compare two common methods of regional anesthesia in pediatric ACL reconstruction: single-shot femoral nerve block and continuous femoral nerve catheter. To the authors’ knowledge, this is the first study to report isokinetic strength data as well as pediatric PROMIS scores after ACL reconstruction in the pediatric population comparing these techniques.
We found that despite increasing in-room to incision time by 30 minutes, FNC demonstrated no superiority to SSNB in all studied measures of postoperative analgesia and proxies of adequate pain in cohorts of similar demographic and surgical characteristics. Patients with FNC also had a significantly lower rate of return to school at the 1-week follow-up visit compared to those who received SSNB. Although data in children and adolescents is lacking, studies on adult patients undergoing ACL reconstruction have similarly failed to find superior analgesia with the use of FNC compared to other forms of regional anesthesia.24,25
We additionally sought to determine patient-reported outcomes for each anesthesia technique. Although PROMIS has been shown to be a valid, reliable, and responsive patient-reported outcome measure in multiple patient populations, our study is the first report of PROMIS scores in pediatric ACL reconstruction.15,26 Although there are no papers in the literature regarding PROMIS minimum clinically important difference (MCID) values in pediatric patients undergoing ACL reconstruction, similar studies in adults, as well as fracture studies, have suggested an MCID of 3.9 to 8.0, which was used for our power analysis.15–17 Among our study population, patients who received an FNC had significantly lower mean PROMIS physical function – mobility scores at 1 week postoperative, although this difference was not observed in pain interference scores, and the groups were similar at other timepoints. We also found no differences in active range of motion during the follow-up period. While the reason for the delayed return to school and lower mobility scores in the FNC group is not clear, we postulate that the mere presence of a catheter makes the patient/family more conservative in their activities, despite the pain control it provides. Furthermore, leakage of fluid around the catheter is common and might be another reason for patients’ limited mobility.
Peripheral nerve blocks are effective postoperative pain control strategies that also allow immediate mobilization and provide high patient satisfaction. Despite their well-documented benefits,20,27–29 rare cases of femoral neuropathy have been reported.9,30 Furthermore, prolonged quadriceps weakness, increased risk of falls, and delayed rehabilitation milestones have been reported in the adult population.7 The literature is not conclusive on the long-term effects of femoral nerve blocks in children and adolescents. Holland et al. compared the efficacy and complications of continuous femoral nerve blocks with continuous adductor canal block in adolescents undergoing ACL reconstruction and found no differences in analgesic needs and quadriceps strength by 6 months after surgery.31 In contrast, Luo et al. compared FNB with no block in pediatric ACL reconstruction and found that patients with FNB had a significantly higher deficit in isokinetic extension strength, although there were no differences in functional tests, including vertical jump and single hop.8 Parikh et al. evaluated limb strength asymmetry at 6 months after ACL reconstruction in patients undergoing either FNC or FNB.32 In their study, FNB was associated with higher levels of symmetry on single-leg squat.
We found no differences in limb symmetry indices at 3- or 6-month follow-up, although patients who received SSNB had a higher hamstring/quadriceps ratio at 3 months postoperatively, which indicates greater quadriceps weakness at that timepoint. All isokinetic strength differences resolved by 6 months postoperatively. While the long-term effects of FNC is not clear, the impact on quadriceps strength seems to be temporary.11 In our practice, SSNB is the preferred choice for postoperative analgesia in children and adolescents undergoing ACL reconstruction for several reasons. First, early mobilization and initiation of formal physical therapy, which is imperative in preventing complications such as arthrofibrosis, requires a safe and efficient pain control strategy. Reflected in a reduced return-to-school rate and lower PROMIS mobility scores at 1 week, we found that FNCs limit activity for patients to a greater degree. Additionally, the benefits of reduced operating room utilization for patients receiving SSNB are not insignificant, considering the average cost of operating time use estimated to be $62 per minute.33 While this time cost may be less relevant in adult orthopaedics where regional anesthesia can be performed preoperatively, in many pediatric hospitals, regional procedures are completed in the operating room after patient induction. Finally, differences in hamstring/quadriceps ratio existed only at 3 months and disappeared by the 6-month visit. Our institutional protocol does not allow for return to sports until at least 9 months postoperative; thus, any strength differences in regional anesthetics had resolved by this time.
We must acknowledge limitations to our study, including those inherent in the retrospective design. First, approximately 10-25% of data points were missing for PROMIS, strength, and active ROM data. This was mitigated by employing multiple imputations, a well-established method of dealing with random missing data. We also had to exclude 131 patients from our final sample due to various reasons, which inevitably introduces selection bias in the study. Patients were excluded mainly for the lack of postoperative PROMIS and/or strength data. Although the a priori power analysis suggests that this sample size was sufficient to discern significant differences in our primary outcome measure of PROMIS scores, we might have been underpowered for AROM or strength data. Additionally, we included data from our main hospital and ASC, which introduces some heterogeneity, especially since surgical setting dictated the block technique.
In conclusion, our findings suggest that both SSNB and FNC are viable options with minimal complications in ambulatory ACL reconstruction in the pediatric population, providing comparable analgesia and functional outcomes. However, we did not find any evidence that the analgesia provided by the FNC is superior to SSNB in the postoperative period. Furthermore, patients receiving an FNC spent a significantly longer time in the operating room dedicated to the preparation and insertion of the catheter. They also tended to return to school later than patients with SSNB and had lower PROMIS mobility scores at 1 week postoperatively. There were no significant differences between groups in terms of function and PROMIS scores at 6 months postoperatively.
Disclaimer
No funding was received. The authors report no conflicts of interest related to this manuscript.
Acknowledgement
The authors would like to thank the Bisignano Family for their support of the Children’s Hospital of Philadelphia Sport Medicine and Performance Center research initiative.
References
- Beck NA, Lawrence JTR, Nordin JD, et al. Acl tears in school-aged children and adolescents over 20 years. Pediatrics. 2017;139(3):e20161877.
- Mall NA, Chalmers PN, Moric M, et al. Incidence and trends of anterior cruciate ligament reconstruction in the united states. Am J Sports Med. 2014;42(10):2363-2370.
- Chieng YJS, Chan WCS, Klainin-Yobas P, et al. Perioperative anxiety and postoperative pain in children and adolescents undergoing elective surgical procedures: a quantitative systematic review. J Adv Nurs. 2014;70(2):243-255.
- LaMontagne LL, Hepworth JT, Salisbury MH. Anxiety and postoperative pain in children who undergo major orthopedic surgery. Appl Nurs Res. 2001;14(3):119-124.
- Lakhal W, Chanthany K, Bund L, et al. Outpatient paediatric arthroscopy: a retrospective study in 216 patients. Orthop Traumatol Surg Res. 2018;104(7):1091-1094.
- Liu DV, Lin Y-C. Current evidence for acute pain management of musculoskeletal injuries and postoperative pain in pediatric and adolescent athletes. Clin J Sport Med. 2019;29(5):430-438.
- Edwards MD, Bethea JP, Hunnicutt JL, et al. Effect of adductor canal block versus femoral nerve block on quadriceps strength, function, and postoperative pain after anterior cruciate ligament reconstruction: a systematic review of level 1 studies. Am J Sports Med. 2020;48(9):2305-2313.
- Luo TD, Ashraf A, Dahm DL, et al. Femoral nerve block is associated with persistent strength deficits at 6 months after anterior cruciate ligament reconstruction in pediatric and adolescent patients. Am J Sports Med. 2015;43(2):331-336.
- Lynch J. Prolonged motor weakness after femoral nerve block with bupivacaine 0.5%. Anaesthesia. 1990;45(5):421.
- Okoroha KR, Khalil L, Jung EK, et al. Single-shot femoral nerve block does not cause long-term strength and functional deficits following anterior cruciate ligament reconstruction. Arthroscopy. 2018;34(1):205-212.
- Swank KR, DiBartola AC, Everhart JS, et al. The effect of femoral nerve block on quadriceps strength in anterior cruciate ligament reconstruction: a systematic review. Arthroscopy. 2017;33(5):1082-1091. e1.
- Baghdadi S, VanEenenaam Jr DP, Williams BA, et al. Quadriceps tendon autograft in pediatric ACL reconstruction: graft dimensions and prediction of size on preoperative MRI. Orthop J Sports Med. 2021;9(12):23259671211056678.
- White IR, Royston P, Wood AM. Multiple imputation using chained equations: Issues and guidance for practice. Stat Med. 2011;30(4):377-399.
- Rubin DB, Schenker N. Multiple imputation in health-are databases: an overview and some applications. Stat Med. 1991;10(4):585-598.
- Chen RE, Papuga MO, Voloshin I, et al. Preoperative promis scores predict postoperative outcomes after primary acl reconstruction. Orthop J Sports Med. 2018;6(5):2325967118771286.
- Hung M, Bounsanga J, Voss MW, et al. Establishing minimum clinically important difference values for the patient-reported outcomes measurement information system physical function, hip disability and osteoarthritis outcome score for joint reconstruction, and knee injury and osteoarthritis outcome score for joint reconstruction in orthopaedics. World J Orthop. 2018;9(3):41-49.
- Sandvall B, Okoroafor UC, Gerull W, et al. Minimal clinically important difference for promis physical function in patients with distal radius fractures. J Hand Surg. 2019;44(6):454-459.e1.
- Ganley TJ. Pediatric anterior cruciate ligament injury: advocating for the next generation. Am J Sports Med. 2020;48(8):1809-1811.
- Abdallah FW, Brull R, Joshi GP. Pain management for ambulatory arthroscopic anterior cruciate ligament reconstruction: evidence-based recommendations from the society for ambulatory anesthesia. Anesth Analg. 2019;128(4):631-640.
- Hall-Burton DM, Hudson ME, Grudziak JS, et al. Regional anesthesia is cost-effective in preventing unanticipated hospital admission in pediatric patients having anterior cruciate ligament reconstruction. Reg Anesth Pain Med. 2016;41(4):527-531.
- Jansson H, Narvy SJ, Mehran N. Perioperative pain management strategies for anterior cruciate ligament reconstruction. JBJS Rev. 2018;6(3):e3.
- Miller DJ, Nelson SE, Shah AS, et al. Outpatient pediatric orthopedic surgery. Orthop Clin North Am. 2018;49(1):55-62.
- Secrist ES, Freedman KB, Ciccotti MG, et al. Pain management after outpatient anterior cruciate ligament reconstruction: a systematic review of randomized controlled trials. Am J Sports Med. 2015;44(9):2435-2447.
- Faunø P, Lund B, Christiansen SE, et al. Analgesic effect of hamstring block after anterior cruciate ligament reconstruction compared with placebo: a prospective randomized trial. Arthroscopy. 2015;31(1):63-68.
- Woods GW, O’Connor DP, Calder CT. Continuous femoral nerve block versus intra-articular injection for pain control after anterior cruciate ligament reconstruction. Am J Sports Med. 2006;34(8):1328-1333.
- Scott EJ, Westermann R, Glass NA, et al. Performance of the promis in patients after anterior cruciate ligament reconstruction. Orthop J Sports Med. 2018;6(5):2325967118774509.
- Schloss B, Bhalla T, Klingele K, et al. A retrospective review of femoral nerve block for postoperative analgesia after knee surgery in the pediatric population. J Pediatr Orthop. 2014;34(4):459-461.
- Tran KM, Ganley TJ, Wells L, et al. Intraarticular bupivacaine-clonidine-morphine versus femoral-sciatic nerve block in pediatric patients undergoing anterior cruciate ligament reconstruction. Anesth Analg. 2005;101(5):1304-1310.
- Kirkham K, Grape S, Martin R, et al. Analgesic efficacy of local infiltration analgesia vs. Femoral nerve block after anterior cruciate ligament reconstruction: a systematic review and meta-analysis. Anaesthesia. 2017;72(12):1542-1553.
- Albrecht E, Niederhauser J, Gronchi F, et al. Transient femoral neuropathy after knee ligament reconstruction and nerve stimulator-guided continuous femoral nerve block: a case series. Anaesthesia. 2011;66(9):850-851.
- Holland EL, Robbins RE, Low DK, et al. Comparison of continuous adductor canal and femoral nerve blocks for analgesia and return of quadriceps function after anterior cruciate ligament reconstruction in adolescent patients. Arthrosc Sports Med Rehabil. 2020;2(2):e121-e128.
- Parikh HB, Gagliardi AG, Howell DR, et al. Femoral nerve catheters and limb strength asymmetry at 6 months after primary anterior cruciate ligament reconstruction in pediatric patients. Pediatr Anesth. 2020;30(10):1109-1115.
- Shippert RD. A study of time-dependent operating room fees and how to save $100 000 by using time-saving products. Am J Cosmet Surg. 2005;22(1):25-34.