
JPOSNA® Special Edition
Advances in Pediatric Orthopaedic Education and Technical Training
Integrating Simulation for Developing Slipped Capital Femoral Epiphysis Fixation Skills into an Orthopaedic Surgery Residency Program
1Department of Orthopedics and Rehabilitation, University of Iowa, Iowa City, IA; 2Department of Biomedical Engineering, University of Iowa, Iowa City, IA; 3Department of Industrial and Systems Engineering, University of Iowa, Iowa City, IA
Correspondence: Joshua B. Holt, MD, Department of Orthopedics and Rehabilitation, 200 Hawkins Drive, Iowa City, IA 52242. E-mail: [email protected]
Received: June 13, 2022; Accepted: July 11, 2022; Published: August 15, 2022
DOI: 10.55275/JPOSNA-2022-0087
Volume 4, Number S1, August 2022
Introduction
Slipped capital femoral epiphysis (SCFE) in pediatric and adolescent patients is a common hip injury treated at tertiary care centers and children’s hospitals. A SCFE is the result of unwanted motion through the capital femoral physis, and the resulting deformity most commonly includes extension, varus, and external rotation of the metaphysis in relation to the epiphysis. Although the acuity, severity, and stability of the “slip” vary from one patient to the next, the resulting deformity is reliable and reproducible. The predictable deformity, in conjunction with the relatively uncommon nature of these injuries, makes this an ideal model for using surgical simulation to help residents, fellows, and trainees gain proficiency with screw fixation.
SCFE In Situ Fixation
Typical treatment of low and moderate-grade stable SCFE consists of percutaneous fixation of the epiphysis. This common technique aims to limit further displacement and stabilize the proximal femur until the eventual closure of the capital physis.1 The ideal position of guidewire placement (and eventual screw fixation) is near the center of the neck, perpendicular to the physeal margin of the epiphysis. Wire placement into the epiphysis should be deep enough to allow for several threads of screw fixation while avoiding joint penetration. The reproducible posterior position of the epiphysis relative to the metaphysis results in the need for a more anterior starting point on the femoral neck than would be anticipated when fixing a non-displaced femoral neck fracture in a geriatric patient, for example. The balance between final screw placement and attempts required to obtain ideal positioning is purely an academic discussion. Multiple reports have suggested that increasing the number of attempts at guidewire placement and resulting fenestration of the proximal femur may increase the risk of postoperative fractures.2,3 However, incorrect screw placement can result in further slippage, screw loosening, joint penetration, chondrolysis, fractures, and avascular necrosis.4 This unique pathology contributes to much of the surgical difficulty and unfamiliarity when considering surgical treatment of SCFE. However, it also provides a great educational opportunity for orthopaedic residents and fellows to demonstrate a true understanding of the pathology, proficiency in wire placement techniques, and makes for an ideal simulation model to supplement orthopaedic training.
Thoughtful evolution of orthopaedic resident education and skills assessment has been a long-standing goal at the University of Iowa. The clinical faculty and research personnel have pioneered the creation and advancement of several novel surgical simulation models. These include pediatric supracondylar humeral fracture reduction and fixation models, a distal tibia fracture reduction and fixation model, a proximal femur fracture fixation model, and an in situ SCFE fixation model. Through state-of-the-art calibration techniques, these simulation models provide real-time training and immediate feedback regarding wire placement techniques. Through repeated exposure to the methods of “fluoroscopic” assessment of fracture morphology, wire navigation for proper placement of fixation or guidewires, and functional assessment of specific aims, the simulation models can provide feedback that cannot be obtained in a live operating room setting.
Simulator Overview
A novel video camera system was developed in conjunction with a sawbones adolescent SCFE model (Figure 1). The camera system allows radiation-free imaging to be obtained and mapped to the calibrated bony model at any time during simulation. An etched wire with calibrated bare coding, as seen in Figure 2, is used to allow the camera system to determine the exact position of the wire in space, thereby providing immediate feedback of where the wire is in relation to the proximal femur anatomy.
Figure 1. Novel video camera system with associated sawbones SCFE model and overlying soft tissue envelope.

Figure 2. Laser-etched bar-coding on guidewire allows cameras to determine the exact position and orientation of the wire in space. The wire location is correlated with the position of the sawbones model within the soft tissue envelope and allows for the simulation model to project a “fluoro” image on the computer screen at any point during the exercise.

The sawbones model of the SCFE with associated fabricated soft tissue envelope is aligned with previously obtained coordinating anterior/posterior (AP) and lateral fluoroscopic imaging on the computer screen (Figure 3). This allows for real-life feel and immediate tactile feedback of the wire entering the bony anatomy of the sawbones model while simultaneously providing the visual feedback of the wire entering the bony anatomy depicted on the radiation-free “fluoro” image projected on the computer screen.
Figure 3. Photo image of an orthopaedic resident working through the simulation model tasks. Participants have a foot pedal (not pictured) that allows them to obtain AP and lateral “fluoro” images at any point during the exercise.

Implementation of SCFE Pinning at Your Institution
Depending on the training program, the ideal timing of simulation training in SCFE management can be variable. At our institution, the second-year orthopaedic residents are expected to understand simple SCFE pathoanatomy and are developing their understanding of 3D spatial understanding of wire/drill placement and guidance. Additionally, we have a dedicated week of surgical skills development for the class, in which staff surgeons provide dedicated didactic education regarding operative techniques across all specialties of orthopaedic surgery. A large part of this skills week is the opportunity for each resident to develop and advance their skills through surgical simulation, including the SCFE simulation model.
Each participant is instructed as to the goals of guidewire placement including the goal position near the center of the neck and near perpendicular to the physis, without penetrating the joint space. Further, they are made aware of the overall metrics which they will be evaluated including procedure duration, the total number of “fluoroscopic” images obtained, number of wire redirections, and overall guidewire position relative to the “ideal” position on both AP and lateral imaging. Participants are free to obtain “fluoroscopic” AP and lateral imaging at any time and as often as necessary during their pre-assessment simulation. At the completion of the task, the participants are provided with immediate objective feedback regarding their performance as a combined simulator performance distribution measure (Figure 4).
Figure 4. Graphic demonstration of simulator performance. Overall participant performance (dashed blue line) as compared with proficiency benchmark (dashed green line).

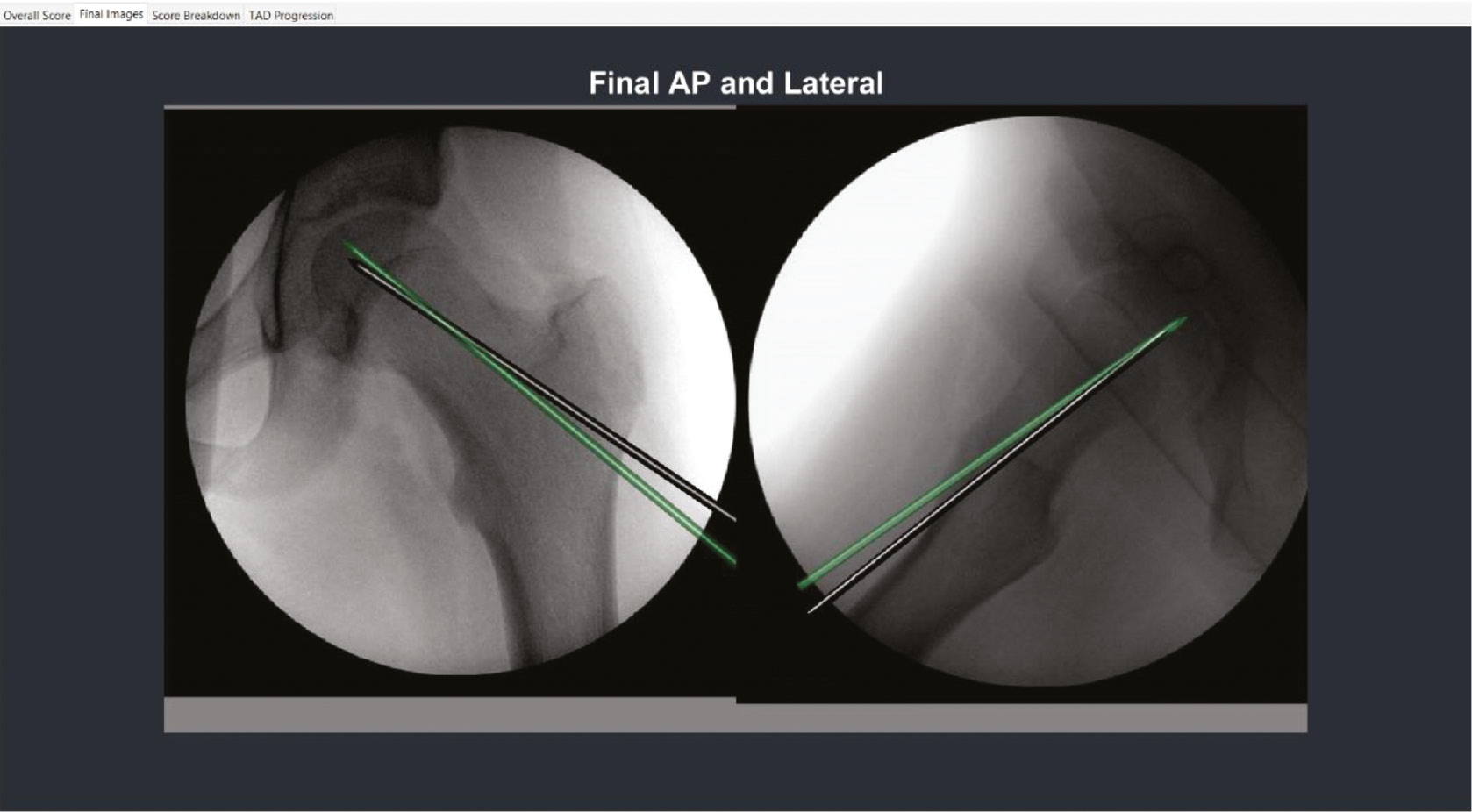
This is a combined measure of the metrics described above, displaying the participants simulation score with the proficiency benchmark in visual form. They are also able to view an overlay of their final guidewire position as compared with the ideal wire position as demonstrated in Figure 5.
Figure 5. Final “fluoro” imaging overlay of participant’s guidewire placement (black wire) as compared with ideal guidewire positioning (green wire).
Simulator Advancements
Continued advancement in the development of the simulation model is ongoing. Improvements in the soft tissue envelope will allow for a more realistic feel of guidewire navigation through soft tissue constraints. Production of bone models with moderate and high-grade SCFE will help participants to understand the required start point and changing guidewire trajectories that are required depending on slip severity. Finally, the establishment of a defined simulation training program in which pre-assessment performance measures are obtained, a structured educational course with defined objectives is provided, and a post-course assessment is completed will provide participants with improved feedback on overall performance and improvement. This will also allow for comparison of performance longitudinally through residency/fellowship training as well as comparison between participants by level of training.
Disclaimer
Funding: 2018 POSNA Directed Research Grant, Amount $50,000. S. Long, M. Tatum, G. Thomas, D. Anderson, M. Karam: Part owner, Iowa Simulation Solutions, LLC. J. Holt and H. Kowalski: No conflicts of interest to disclose.
References
- Loder RT, Dietz FR. What is the best evidence for the treatment of slipped capital femoral epiphysis? J Pediatr Orthop. 2012;32(Suppl 2):S158-S165.
- Lehman WB, Menche D, Grant A. The problem of evaluating in situ pinning of slipped capital femoral epiphysis: an experimental model and a review of 63 consecutive cases. J Pediatr Orthop. 1984;4(3):297–303.
- Walters R, Simon SR. The hip: proceedings of the eighth open scientific meeting of the hip Society. St. Louis: CV Mosby; 1980:145-164. Joint destruction: a sequel of unrecognized pin penetration in patients with slipped capital femoral epiphyses.
Appendix
Program Costs
- The wire navigation simulator is manufactured by Iowa Simulation Solutions (www.iasimsol.com), a small startup company founded by University of Iowa research team members. Residency or fellowship training programs can purchase a simulator package that includes the slipped capital femoral epiphysis fixation module for $20,000. Other add-on modules (e.g., pediatric supracondylar humeral fracture, hip fracture DHS wire navigation, cephalomedullary nail guidance, iliosacral screw navigation) are available and new modules are in development.
- The surrogate bone models used with the SCFE module can be purchased from Sawbones and are currently priced at $27.75 per bone (Femur with Slipped Capital Epiphysis (sawbones.com).