
JPOSNA® Special Edition
Advances in Pediatric Orthopaedic Education and Technical Training
The Next Generation of Immersive Surgical Education: We Must Achieve Presence
1Vanderbilt University Medical Center, Department of Orthopaedics, Nashville, TN; 2Vanderbilt University Medical Center, Department of Pediatrics, Nashville, TN; 3Vanderbilt University Medical Center, Department of Pathology, Nashville, TN; 4Vanderbilt University, Department of Pharmacology, Nashville, TN; 5Vanderbilt University Medical Center, Center for Bone Biology, Nashville, TN; 6Change Healthcare, Nashville, TN
Correspondence: Jonathan G. Schoenecker, MD, PhD, Vanderbilt University Department of Orthopaedics, Division of Pediatrics, 2200 Children’s Way, Nashville, TN 37232-9565. E-mail: [email protected]
Received: June 6, 2022; Accepted: June 13, 2022; Published: August 15, 2022
DOI: 10.55275/JPOSNA-2022-0068
Volume 4, Number S1, August 2022
Abstract:
The benefit of improving the quality and efficiency of training pediatric orthopaedic surgeons is clear. The ideal solution is to provide cost-efficient simulation of pediatric orthopaedic pathology that permits the development of cognitive and psychomotor skills with unlimited repetitions and no possibility of harming a child. New generation virtual reality simulations have the potential in surgical training to accomplish this goal. To be successful as a simulator, a trainee must achieve presence, the feeling of being somewhere other than where you are in physical reality. Presence is mostly derived from two constructs: immersion, or the photo-realism of the simulation, and coherence, which is the process of following a consistent mental model built by previous experiences. Technological advances since the 1980s have significantly enhanced immersion to the point that this construct is no longer rate limiting in achieving presence in medical virtual reality. This advancement has prompted significant enthusiasm to transition to virtual reality platforms in orthopaedic training. However, from our experiences at medical conferences and at our institution, we postulate that coherence is a second barrier that must be overcome prior to the adaptation of virtual reality in pediatric orthopaedic training. This barrier stems from the significant heterogeneity of mental frameworks at the cognitive and psychomotor level in pediatric orthopaedics. While efforts are ongoing to form consensus through evidence-based medicine, the rare nature of the pathophysiology in pediatric orthopaedics makes these efforts difficult, rendering much of the practice to be based on clinical intuition. Without consensus of practice, training modules are often biased towards the opinion of the author, which may prompt a learner’s rejection of the simulation, as it differs from their own coherence or mental framework. The point at which this loss of presence occurs is inversely proportional to the level of training—where the less advanced trainee will accept the simulator, the more advanced trainee will reject the same simulation. Objectively, a potential consumer must determine their optimal stopping point where the risk of investment in virtual reality outweighs the point at which their trainees lose presence and therefore the efficacy of the technology as an educational mechanism. The solution to coherence as a problem of achieving presence is two-fold. First, from a development standpoint, the point at which presence will be accepted, according to the trainee level, is a function of the ability to produce all-inclusive, unbiased material to accept all potential, equally efficacious mental frameworks to be represented, allowing for educational choice. The second, and more daunting task, is to develop consensus in the practice of pediatric orthopaedics, especially where evidenced-based medicine is an intangible goal in the immediate future.
Key Concepts:
- Virtual reality simulation has the potential to improve the efficiency of education in pediatric orthopaedics.
- Presence is mostly derived from two constructs: immersion, or the photo-realism of the simulation, and coherence, which is the process of following a consistent mental model built by previous experiences.
- Previous problems of immersion in virtual reality have largely been overcome, leading to enthusiasm for applying virtual reality in pediatric orthopaedics.
- Problems of coherence are significant barriers to achieving presence and therefore universal application of virtual reality in pediatric orthopaedic surgical education.
- Solutions to coherence problems involve both producing unbiased educational material and forming a consensus of practice in pediatric orthopaedics.
Introduction
Virtual reality (VR) is here … again. Last time, in the 1980s, after a few years of enthusiasm, embattled with the ample use of airline sanitation bags due to motion sickness, it quickly rested in peace. The current medical simulation million-dollar question is, will VR stick this time?
Every medical VR start-up advocates an enthusiastic Yes. Compared to the 1980s, substantial improvements to hardware and animation, along with a lower cost, strongly support the plausibility that medical simulation VR is here to stay. This buzz has created an extreme fear of missing out in most healthcare sectors, including orthopaedic residency training programs and equipment companies. Matching this enthusiasm, investors are showing huge financial support for VR training in medicine. For example, one orthopaedic-focused VR start-up impressively raised $70 million.
So, this is it, right? All of our problems with efficiency and delivery of pediatric orthopaedic education outlined below are solved with the use of VR simulations? Maybe.
Five years ago, I became infatuated with answering this question. Thanks to the trust of others equally as enthusiastic to determine if they should invest their interest and money in VR, I had a first-hand experience watching this ortho VR wave rise. My initial involvement in medical simulation-VR was with my co-conspirator in this quest, Dr. Bryan Tompkins, at a Medical VR symposium at Harvard in 2018, thanks to the support of our friend Dr. Peter Armstrong. Within minutes of exploring the demonstrations, we both concluded that the potential for VR to revolutionize orthopaedic training was legitimate. This appears to be the response of anyone who has explored medical simulation. The first time you put on the new generation VR gear and dive into an operating room, the sensation is overwhelmingly awesome and does not provoke the nausea of its doomed 1980s preceding form. If I had been asked to write this commentary then, I would have written an entirely different article filled with enthusiastic unconditional endorsement.
Now, after many first-hand experiences in helping develop VR training modules, testing the educational experience and efficacy of these modules at the International Pediatric Orthopaedic Symposium (IPOS®) and Vanderbilt, and quantitatively and qualitatively measuring instructor and learner feedback, I am much more reluctant to advocate full support of investing in VR as the predominant orthopaedic simulator. While there are places where I do think that VR can be successfully employed currently, I do not yet recommend revamping our educational programs for pediatric orthopaedics until the problem of presence can be resolved (Figure 1).
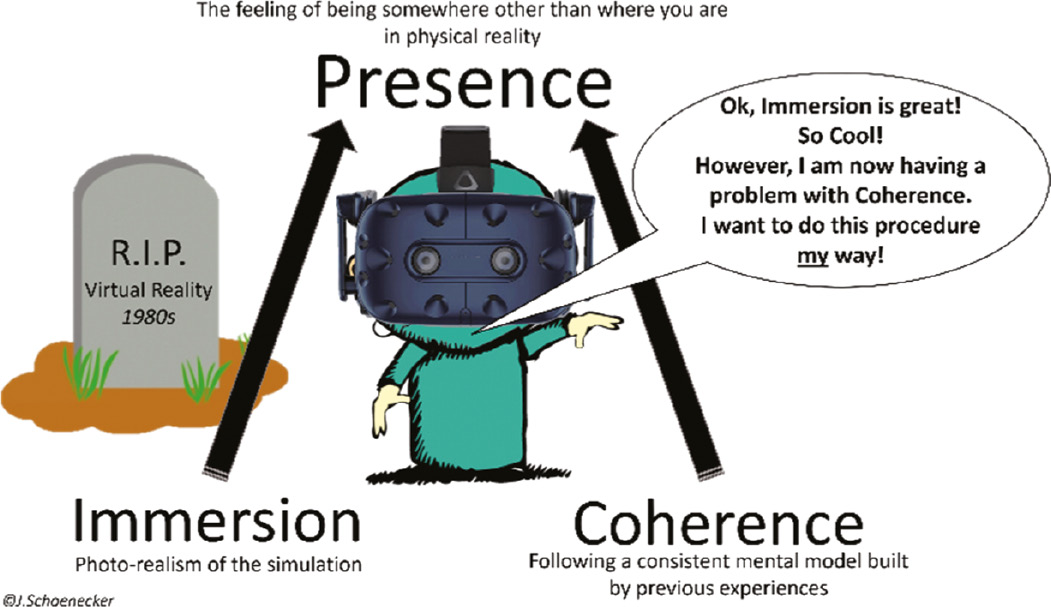
Figure 1. Has VR risen from the 1980s grave? Initial reaction is extremely optimistic. However, with regards to surgical simulation, caution to proceed slowly is advised until problems with coherence affecting the ability to achieve presence are improved.

Ok, that was an easy BLUF (Bottom Line Up Front). Now for the hard part—to provide objective rationale for this conclusion and even harder, determine what needs to be done to fix the problem of presence to unleash the utility of VR as an educational tool for pediatric orthopaedics. Thank goodness JPOSNA® is online and did not ask for a word limit. So, here we go, let us start with, Why do we need simulators?
Why Simulators? Chicago in July
Chicago in July means something very different to an orthopaedic surgeon compared to most others. To any orthopaedic surgeon, this statement evokes an extreme emotional recall. It is the culminating performance before being ordained as an American Board of Orthopaedic Surgery (ABOS) certified surgeon. ABOS certification declares that a candidate has the clinical knowledge and intuition to safely care for patients and perform orthopaedic surgery. It is the interrogation of 6 months of the candidate’s clinical practice in front of three pairs of examiners tasked with finding critical gaps in clinical knowledge and intuition. I remember that day so well. Walking to the stadium with my co-resident Nate VanZeeland, both of us were sufficiently nervous that we could not stomach a full breakfast. Yet, we were also proud of our grit for making it this far. After successfully defending myself, it was over—I passed.
For me, the pilgrimage to the Windy City was permitted only after committing 18 years to higher education—4 years of pre-medical education, 6 years of combined medical and graduate training, 5 years of surgical residency, 1 year of fellowship, and 2 years of practice. By the time I was ABOS certified, I had expended greater than half of my life training to perform surgery on pediatric musculoskeletal maladies in the operating theater.
Now, 13 years into practice, 11 years post-ABOS ordainment, I am convinced that surgical education is disproportionally inefficient compared to most other vocations that require mastery of a knowledge base combined with the development of psychomotor skills. Reflecting on what skills I need to perform even the most complex pediatric orthopaedic surgeries, I do not think it should require, at a minimum, 16 years of training (Figure 2).
Figure 2. The 16-year journey to board certification culminating in Chicago in July. Few occupations with similar requirements of cognitive and psychomotor training require this duration of training, suggesting that the efficiency of training a pediatric orthopaedic surgeon is not optimized. Many put forward that simulators have the potential to remove chance of encountering the pathology a trainee must master from the training equation with simulation can improve educational efficiency.

This inefficiency in training confers an opportunity cost that deters many and has a significant negative effect on the wellness of a training surgeon. The financial opportunity cost of becoming a surgeon is obvious, as medical education is very expensive and salaries during residency training are not sufficient to both support a family and pay off medical education loans. In addition, there are less obvious, but equally impactful, life opportunity costs in committing to become a surgeon. Surgical residency training, which often requires weekly work time equivalent to two full-time jobs, or 80 hours per week, most often coincides with the time when one marries and starts a family. Combined with the substantial material and skill required to learn, these opportunity costs turn many away from surgery. I also put forward that these opportunity costs are silent but extensive barriers to resolving the underrepresentation of race, socioeconomic status, and gender at the helm of the operating theater. There is inherent self-selection towards individuals who can afford the financial and life opportunity costs of surgical training. Therefore, we must determine the root of these inefficiencies to provide the healthcare system with the most competent, well, and diverse surgeons.
For sake of argument, let us focus on educating pediatric orthopaedic surgeons. In my opinion, there are two main barriers to increasing the efficiency of training a pediatric orthopaedic surgeon: The first, is that the experiences required to master surgical psychomotor training are reliant upon chance of the pathology presenting and a mentor to teach how to fix the pathology. The second, is the knowledge base required to practice pediatric orthopaedics is constructed in the setting of a paucity of evidence-based medicine (EBM).
Barrier 1: Chance—The Problem with Every Other Night Call
At first glance, like the development of any technical skill, surgical education should be straightforward. The learner must master the base of knowledge and the psychomotor skills required to perform the surgery. Malcolm Gladwell made popular multiple lines of research by Drs. Anders Ericsson, Michael Prietula, and Edward Cokely that indicate mastering a complex psychomotor skills requires 10,000 hours of training.1,2 This ranges from hitting a baseball, to becoming a concert pianist, or to do a periacetabular osteotomy. OK, maybe Malcolm did not mention PAO in his podcast, but that is what I heard. In a semi-scientific way, looking into our historic experiences at Vanderbilt, this equates to roughly 2,000 cases between PGY-2 and PGY-5 and 300–500 cases as a fellow. Therefore, the path is straightforward: master the knowledge and psychomotor skills required to become an orthopaedic surgeon, enter a residency program, and fellowship that provides you with your 10,000 hours or roughly 2,300 cases (Figure 3).
Figure 3. The ideal residency and fellowship training—aiming for the quality 10,000 hours to become an expert.

This is an extremely high number of cases. The necessity to fulfill this case requirement during residency training led to old mantras of “What is wrong with every other night call?”, “You miss half the cases” or “If you can’t get it done in 24 hours, you might need to stay up late.” Prior to the implementation of work hour restriction, interns and residents alike had the availability to experience more cases, particularly those that were emergent/urgent or rarer in incidence.3 A training program’s pathology catchment and therefore chance of presentation will dictate what cases that learner will experience. This is especially true for experience in pediatric orthopaedics, as much of what we care for would be considered rare diseases across the medicine landscape. Although I aim to treat multiple epiphyseal unstable SCFEs and opened multiple avascular supracondylar humerus fractures with every one of my residents and fellows, many go through our program without this experience despite having completed 2,000+ cases, because these pathologies, unfortunately did not present when they were on call or on service.
Furthermore, the trainee’s return on time investment is directly proportional to experiencing these cases with an educator who is methodical about teaching the craft. Therefore, choosing where to invest these ~2,300 cases during residency and fellowship is a risk to the trainee. They must choose a program filled with sufficient pathologic opportunity with mentors eager to provide first-hand experiences. However, even with an ideal training environment, pediatric orthopaedics is filled with rare opportunities that may be missed. These missed opportunities are compounded by work hour restrictions.3 While work hour restrictions have shown improvement in patient quality and safety across many medicine specialties, there have been numerous contrary findings when evaluating surgical subspecialties,4,5 raising the question if work hour restrictions are impeding cognitive and psychomotor learning. Therefore, there remains multiple reasons for removing “chance” from the pediatric orthopaedics educational equation.
Enter simulation. The clear answer to the first problem of education in pediatric orthopaedics is a training simulator that provides unrestricted training scenarios that comprehensively cover all pathologies, thereby removing chance. A simulator that provides the learner with cognitive and psychomotor skills required to safely care for a child, without consequences to an actual child, would be a welcome advancement to residency training. There have been many attempts to develop these simulations, many of which are excellent and used across institutions for the training of the medical students and residents. For the sake of space, I will not cover these here, though fully support their inclusion in medical training. Let us jump into VR.
Five years ago, what I took away from the VR conference at Harvard was that designing modules to fulfill the above requirements was equivalent to building a flight simulator. There was beautiful objectivity to the task that just took thought, time, and communication with a development team. Thanks to trust from Dr. Donald Bae, who was head of IPOS® at the time, he and POSNA, with help from Vanderbilt, provided resources to make a VR-based SCFE module. The results were not what I expected.
As trainees at IPOS® and Vanderbilt traveled through the training module, my research team and I quantitatively and qualitatively recorded reactions. A requirement to study responses to new technology is to allow the novelty to wear off. As the initial novelty of the virtual environment wanned, we all noticed consistent results. New learners, with little experience in the operating room, were far more intrigued about gaining the experience of being the lead surgeon provided by the VR module. Specifically, they saw great value in standing at the point of perspective of conducting the surgery as opposed to being a first assist. They also enjoyed rising to the challenge of memorizing and mastering the steps of pinning a SCFE. From these observations, we surmised that we had validated our VR-SCFE module and, therefore, the training at IPOS® and Vanderbilt would forever be changed. However, as time progressed, we detected diminishing returns and enthusiasm for the VR module proportional to the training level. Contrary to the inexperienced learner, surgeons with previous experience were quick to reject and become impatient with the simulator.
As a result, the enthusiasm of the novice was equaled out, or outweighed, by the lukewarm response from the more senior trainees and surgeon instructors. Hence, after putting much time into this effort, I was dismayed that our final report card, both at IPOS® and Vanderbilt, did not support investment into VR at the current cost: benefit assessment.
Blocking Presence: The Coherence Trainwreck
It has taken considerable reflection and discussion with many to objectify what happened and how to move forward. The authors of this work have concluded from our experiences that there was an inverse relationship between training level and the ability to achieve presence in the simulator and this is a significant barrier to overcome.
Presence is the term used in multisensory or immersive experiences of the feeling of being somewhere other than where you are in physical reality.6 It is the outcome of two constructs: immersion and coherence. Immersion pertains to the photo-realism of the simulation. In this case, immersion includes the imagery of the operating room, the patient, and the instruments. Coherence can be loosely defined as following a consistent mental model; in other words, does the experience make sense relative to the trainees’ existing experiences? Achieving presence is vital to the success of VR (Figure 4).
Figure 4. Presence is the product of the two constructs: immersion and coherence. The failure to achieve presence in the 1980s was from the technological inability to produce quality immersion. Today’s technology has overcome this obstacle, generating immense enthusiasm for applying virtual reality to surgical training. However, as outlined here, there now is a problem of coherence which has negative effects on trainees with more established mental frameworks of surgery, causing them to reject the simulator.
My first hypothesis as to why the VR SCFE modules was not accepted by the more experienced surgeons was that they were having difficulty with the immersive experience—either that they were uncomfortable with the technology or they did not find the experience realistic. However, the more we inquired and the more we measured, we found that this was not the case. In fact, many of the experienced instructors marveled at the replication of the operating room and its components and did not have a problem with the technology when allowed to use the VR for a task outside of orthopaedic simulation. This further supports how incredible the immersive experience is in current VR compared to previous attempts.
Instead of problems with the immersive experience, the constant critique that we received from the more experienced learners about the VR SCFE module was that it was too restrictive of a method as how to pin the SCFE. There was a constant barrage of how elements of my technique were incorrect. Yet from the young learners, these elements were praised. More simply put, it appears the more experienced users were having a problem with the coherence component of presence, given that their existing experiences were dissonant with my method of caring for a SCFE.
In retrospect, learning about the applied psychology term coherence has reframed my experiences in medical training. Even before the days of VR simulations, when an alternative diagnosis or treatment was suggested over my own consistent mental model of reasoning, it made me initially uncomfortable. My first response was often to reject it, such as how one feels during a critique-heavy post-op conference or being grilled by Dr. Dennis Wenger at IPOS® when presenting a Master’s Technique that varied from his method. Technically, this is cognitive dissonance theory; we have psychological tension when new information is dissonant with our established thoughts and beliefs. Cognitive dissonance is constant in our professional lives in pediatric orthopaedics. If able to overcome it, we learn much from our mentors and peers. Overcoming cognitive dissonance to improve one’s mental framework fits well with rule 1 of being a productive learner in pediatric orthopaedics as described by one of my favorite mentor’s, Dr. Jim Kasser, which is “You can’t learn anything with your mouth always open.”
Importantly, there are environments in which we are more apt to reject alternative theories, such as when we are in the middle of performing a surgical task. Disruption of focus is so distracting that it is Dr. Kasser’s second rule of being a productive learner, “I have many partners. While I am performing an operation, I do not need to hear how someone else does it.” In accordance with this concept, research suggests that although VR requires both coherence and immersion, if choosing between the two, coherence is more important to achieving presence.7 It is now clear to me that for the novice surgeon who has a basic mental model of being in the operating room and pinning a SCFE, it is relatively easy for me to create a simulation that achieves presence based on my method of pinning a SCFE, as it will not disrupt their coherence. However, as a surgeon becomes more experienced, it becomes much more difficult to achieve presence as, similar to being interrupted when one finds focus in the OR, it causes a complete disruption of coherence if an alternative method is presented. Again, refer to Dr. Kasser’s rule number two above.
So, now we know the problem. We must improve presence by adapting to accommodate a wide range of mental models in pediatric orthopaedics within VR modules. Unfortunately, this highlights a larger overarching problem: It is hard to build a flight simulator when we cannot agree on how to fly the plane or agree if the plane should even be in the air.
Barrier 2: The Paucity of Evidence-Based Medicine (EBM) In Pediatric Orthopaedics
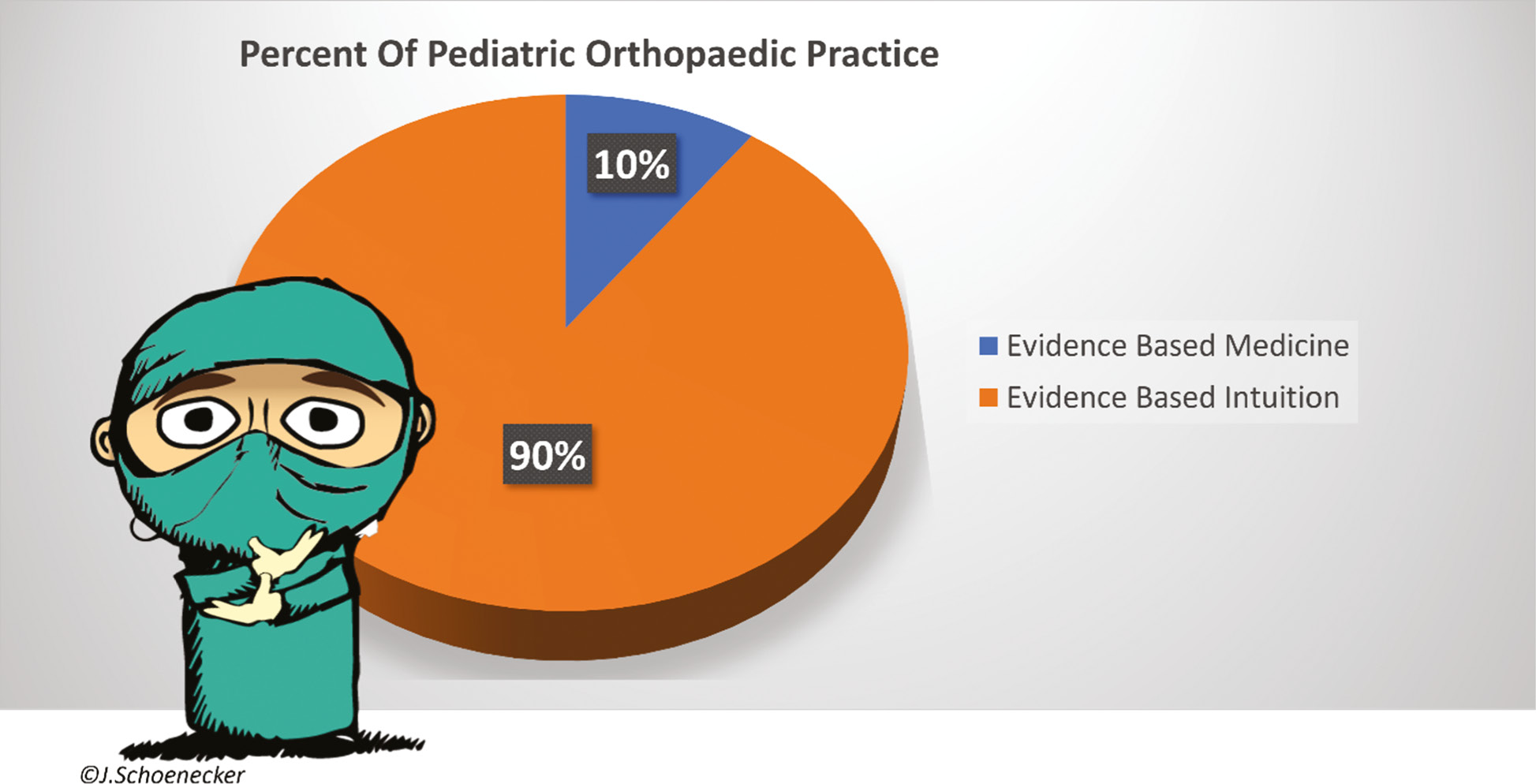
This experience in developing VR simulation, along with other projects that my research partner, Dr. Stephanie Moore-Lotridge and I have taken on to improve the efficiency of medical education, has led me to the enlightenment that 90% of what we practice in pediatric orthopaedics is not EBM, but rather evidenced based intuition (EBI). EBI is very difficult to teach universally, as it requires consensus.
Although often sufficient for publishing, a surrogate outcome measure on x-ray, a p-value > 0.05, or a moniker of a “Level-1” study does not usually translate to the holy grail declaration of EBM. Instead, EBM requires prospective randomized, blinded clinical trials with appropriate sample sizes. For pediatric orthopaedics, these three requirements are all Achilles heels of EBM. We perform surgeries on rare diseases with heterogenous phenotypes for which the most important outcome measures often require years, if not decades, of assessment. Compounding these challenges, our hierarchal priority ranking of these outcomes often differs between surgeons and, more importantly, from those of the patients and their families. Finally, randomization of surgical treatment in pediatric orthopaedics is rife with ethical, consumer, and surgeon biases that often preclude entry into studies and cloud the accuracy of data if they are included. Thus, although an everlasting penultimate target, generating true 100% EBM in pediatric orthopaedics is not going to happen anytime soon.
Optimistically, in 2022, pediatric orthopaedics is 10% EBM, leaving 90% of pediatric orthopaedic practice EBI (Figure 5). Therefore, the practice of pediatric orthopaedics is mostly a biased amalgam of EBI gleaned from our mentors and colleagues, which is then shaped by our personal experiences with our patients. These experiences tend to be most influenced by our Hippocratic oath “do no harm” in that our outcomes of our treatment, or omission of treatment, did not make the patient worse. I find this incredibly important as some of the best advice from my mentors was, and still is, what not to do. Our EBI is also influenced by improved outcomes of the patient, the family, and our expectations. In essence, the practice of pediatric orthopaedics is a patchwork of our predecessors’ EBI modified by our anecdotal good and bad personal experiences.
Figure 5. The daunting reality of the practice of pediatric orthopaedics—90% evidenced-based intuition (EBI) and 10% evidenced-based medicine (EBM).
The problems with a practice so heavily based in EBI is obvious. We cannot be certain that our chosen treatment is the best possible for that patient. EBI is difficult to measure, rendering it incredibly difficult to form a consensus. Although much of the practice of orthopaedics also practices from a high EBI:EBM ratio, pediatric orthopaedics has far less consensus as a product of the rarity of diseases, heterogeneity of penetrance, and the delayed outcomes. Therefore, in other specialties, it is more practical to develop consensus statements on appropriate care in the absence of EBM. Pediatric orthopaedic surgeons continue to practice from opinion.
This training and work environment is not for the faint of heart. A fun fact to consider is that to be a board-certified pediatric orthopaedic surgeon means that you were correct on 70% of the 10% of what will present to your emergency department and clinic. Our families invest their trust in our opinion in 90% of our practice. From a consumer standpoint, our reputation is often a perception or judgment of our EBI. This trust in our opinion is motivating to be our best, yet it is also why our practice can be so difficult when we are wrong. This is likely why pediatric orthopaedics attracts so many opinionated, empathetic risk takers.
Although the mountain we need to climb to optimize EBM in pediatric orthopaedics is titanic, we should always have that target in mind. However, until that time or in instances where EBM is impossible, we also need to formalize EBI consensus building. Consciously or subconsciously, we are always striving to do so through meetings, discussions, and research. Through anecdotal observations, pediatric orthopaedics has a higher number of formal pre- and post-operative conferences than any service out of necessity. It is essential, for the safety of our patients, that we have at least a minor group consensus that our proposed action through EBI is at a minimum going to do no harm. This is a reason not to practice pediatric orthopaedics in a silo.
On a larger scale, this is what makes many elements of IPOS® such a great conference. Allowing for lively debate over differing opinions regarding EBI further support the development and refinement of each observer’s own EBI. As educational and entertaining as these conferences can be, what is missing is a formal attempt to measure consensus through mechanisms such as the Delphi method. Instead, consensus EBI most often emanates from the loudest microphone or the most prolific authors. It is the heart of frustration for many in the paper submission process, as one’s EBI may be rejected by a differing opinion as opposed to scientific reason. Removing biased EBI from the reviewing process is a daunting task that I hope the editors of JPOSNA® can find a way to master. Clearly, there is a need for us as a society to build our EBM and EBI databases.
So, what does this all mean for my opinion about pediatric orthopaedic VR? I sympathize with the developers.
Before, the biggest problem with VR was immersion. The hardware and resolution of our operative theater were so poor that even the untrained participant could not find presence. Coherence did not even have time to weigh in. Now, immersion is no longer an issue due to improving technology. This is the reason for such enthusiasm for adapting it to medical training. However, now we must fix a bigger problem to achieve presence, that is coherence.
Coherence is far more rooted in our differences in our EBI. Without either consolidating the global pediatric EBI through consensus or a miraculous overcoming of odds and delivery of EBM, the only solution to overcoming this problem in simulation is complete equal representation of EBIs.
To add to the problem, in order to be successful in pediatric orthopaedics, we must not only learn pattern recognition of a disease but also how to fix the pathophysiology both in the decision to intervene and how to physically perform the best intervention. Thus, training requires both cognitive and psychomotor development. This means that our data dictionary required and EBI for equal representation does not just include representation of the pathology but also includes how to position a patient, which device to use, and how to use that device. We equally engage in discussions, debates, and research almost as to our technical EBI as we do regarding our debates about pathophysiology. Therefore, to be comprehensive, medical simulations would require incorporation of a considerable number of variables if they were to be universally employed in subspecialties rich in EBI. Without equal representation of EBI, there will always be a breaking point in which the coherence problem interferes with presence (Figure 6).
Figure 6. Extending the efficacy of VR in orthopaedics will require increasing presence to experience acceptance ratio. There typically is initial high acceptance of VR in training in less experienced learners, as they have less problems with coherence. The greater the learners’ existing mental framework (experience), the more likely they have less presence because of a loss of coherence secondary to differences in approach to the pathophysiology presented in the simulator. Currently, we estimate that existing virtual reality modules will be rejected by learners at the PGY-4 level and up. We propose that estimating the presence:experience acceptance ratio makes evaluating the decision to invest in the simulators an objective decision. The goal to increase the efficacy of VR in pediatric orthopaedic training is to make modules with greater presence for more experienced learners which increases the optimal investment stopping point. This can be accomplished both by producing unbiased modules with free-play as well as by moving towards consensus in the practice of pediatric orthopaedics.

Sorry developers, that is a ton of programming. Call it pediatric orthopaedic free-play—infinite options at every decision point in the programming. While the utility can be argued for developing modules for the trainee with less coherence, there is a financial breaking point on investment that must be determined if it is the investment. The risk to bet on VR is still financially significant. Purchasing VR equipment is a gamble as the equipment’s half-life can be very short. Additionally, a hardware as a service model can be pricey, and if it merely sits on a shelf, it quickly becomes a recurring unused cost for a department. Further, initial quotes by the medical VR start-ups to develop a simulation of a single pediatric orthopaedic procedure are roughly $100 thousand without retention of intellectual property rights of the simulation. Therefore, the decision to transition an orthopaedic education program over to VR cannot be taken lightly, especially for residency training programs whose yearly budget for simulation may not even cover development of one module. Consider how many Sawbones® that investment represents. Objectively, each program must determine their “optimal investment stopping point” where they determine that the risk of investment in this new technology outweighs the point at which the trainees lose presence and therefore interest in the technology as an education mechanism (Figure 6). From our experiences, the cross-over point where problems with coherence and presence began was around the PGY-4 level.
This is not to say that I think that current VR simulators do not have a place in orthopaedic training. There are modules that have excellent acceptance to learners with a high presence:experience acceptance ratio derived from excellent immersion and coherence with a lesser existing mental framework (the “you are here” in Figure 6). Going forward, I suggest that focus should be on areas where we do less heterogenous requirements to achieve universal coherence. We need to pick procedures that are truly more like a flight simulator where we agree that the plane should be in the air and how to fly the plane (i.e., EBM or EBI consensus has been achieved). This is likely why most of the VR companies find success in demonstrating intramedullary nails or joint replacements, as there is far more consensus on these procedures. By focusing on maximizing the utility of VR simulators in orthopaedic training on modules with optimal presence, it should provide the resources to build asset libraries and software to permit a digital environment that supports free-play which will reduce the problem of coherence in the more complex procedures with less consensus (the target depicted in Figure 6). In the meantime, it is our responsibility as surgeons to move towards a consensus of our EBI in areas where EBM is not possible for the foreseeable future.
So, VR is here, again. Will it stick in medical education? Yes, but we must proceed pragmatically, understanding how to achieve presence.
Acknowledgement
The authors would like to thank POSNA, IPOS®, residents from the Department of Orthopaedics at VUMC, and Dr. Bryan Tompkins, Christopher Schoenecker, and Ole Molvig for their insight and contributions to this work. They also would like to thank Drs. Peter Armstrong and Donald Bae for their support in exploring the Metaverse.
Disclaimer
Funding for this study was supported by the Department of Orthopaedics, the Division of Pediatric Orthopaedics, The Jeffrey Mast Chair of Hip and Trauma Surgery, IPOS®, and the Caitlin Lovejoy Fund. J. Schoenecker: Receives research funding from the NIH, OrthoPediatrics, IONIS pharmaceuticals, and the Department of Defense. He has ownership in RockLake. M. Tummins and S. Moore-Lotridge: No conflicts of interest to report.
References
- Gladwell M. Outliers: The Story of Success. Little, Brown; 2008.
- Ericsson KA, Prietula MJ, Cokely ET. The making of an expert. Harv Bus Rev. 2007;85:114-121.
- Klingensmith ME, Lewis FR. General surgery residency training issues. Adv Surg. 2013;47:251-270.
- Philibert I, Nasca T, Brigham T, et al. Duty-hour limits and patient care and resident outcomes: can high-quality studies offer insight into complex relationships? Annu Rev Med. 2013;64:467-483.
- Hirschl RB. The making of a surgeon: 10,000 hours? J Pediatr Surg. 2015;50:699-706.
- Slater M. Place illusion and plausibility can lead to realistic behaviour in immersive virtual environments. Philos Trans R Soc B Biol Sci. 2009;364:3549-3557.
- Skarbez R, Neyret S, Brooks FP, et al. A psychophysical experiment regarding components of the plausibility illusion. IEEE Trans Vis Comput Graph. 2017;23:1369-1378.