
JPOSNA® Special Edition
Advances in Pediatric Orthopaedic Education and Technical Training
Building a Clinical Skills Program for Orthopaedic Trainees
1Department of Orthopaedic Surgery and Biomedical Engineering, University of Tennessee Health Science Center - Campbell Clinic, Memphis, TN
Correspondence: Kyle J. Miller, MD, Campbell Clinic Orthopaedics, 1211 Union Ave., Memphis, TN 38104. E-mail: [email protected]
Received: June 4, 2022; Accepted: June 5, 2022; Published: August 15, 2022
DOI: 10.55275/JPOSNA-2022-0056
Volume 4, Number S1, August 2022
Abstract:
Orthopaedic surgery residency education is evolving from the historic mantra of “see one, do one, teach one” to incorporating more formal skill programs into curricula. Each training environment possesses unique resources and constraints, with no single one-size-fits-all approach. Cost remains the single greatest barrier to the development of orthopaedic surgery skills programs. Time also is a concern, as trainees have a finite amount of time to spend in the training environment. Furthermore, time spent in simulation or a skills workshop has the potential to interfere with time spent on direct patient care. Training programs must therefore utilize all available resources in a thoughtful and efficient manner to maximize the educational potential of such a program. By enlisting the help of enthusiastic educators and partners, program directors can build a team with shared common goals. This includes collaboration between training programs, medical schools, and industry. Experience across all levels of orthopaedic knowledge can be incorporated in a top-down fashion to both facilitate trainee education and create an environment conducive to future growth. As educational technology becomes more accessible and educational research advances, skills programs will be able to adapt and adopt evidence-based strategies to improve orthopaedic trainee education.
Key Concepts:
- The key to developing a formal orthopaedic skills program is to utilize available resources and opportunities.
- Program directors should seek willing partners with a shared interest in improving patient care and trainee experience.
- Skills programs should involve trainees of all levels of experience to maximize potential learner benefit and foster an educational culture.
Introduction
The development of surgical skills is of critical importance to orthopaedic surgery training programs. The traditional apprenticeship model of Halstead and the dogma of “see one, do one, teach one” have prevailed in medical education for over a century. However, more recent efforts have been made to formalize the teaching and assessment of surgical or clinical skills.1 This includes both low-fidelity and high-fidelity simulations as well as formal skill-development workshops. More recently, there has been a growing trend toward the incorporation of a formal skills curriculum into orthopaedic surgery training programs.2
Although most trainees and program directors agree that a formal skills program should be part of orthopaedic training, building such a training program can be quite challenging, requiring an investment of time, money, and teaching space.2 High-fidelity surgical-skills training options, such as virtual or augmented reality and surgical models, can be prohibitively expensive or impractical for most programs but can be incorporated into trainee education with some flexibility and creativity. Each training institution possesses its own unique opportunities that can be leveraged to enhance trainee education.
The purpose of this article is to share this institution’s experience in building and maintaining an orthopaedic skills program for resident trainees at all levels.
Background
Orthopaedic surgery is a technically demanding field. Numerous studies have documented the existence of learning curves for surgical procedures, with outcomes being related to the number of procedures performed.3–6 Additionally, the landscape of orthopaedic surgical training has dramatically changed over the past century. Duty-hour restrictions limit the time that trainees can spend in a hospital, and increased specialization and necessary oversight limit the number of surgical repetitions that a trainee can experience.7 As such, there has been a recent push to improve surgical skills to lessen potential risk to patients.2
The orthopaedic surgery training environment consists of a spectrum of training levels, ranging from early medical students to surgical fellows. The level of responsibility is typically stratified according to training level. The degree of autonomy and the detail of knowledge of specific procedures is highly variable based on the learner. Furthermore, surgeons themselves are lifelong learners and adopt new technologies and procedures over time. Thus, the importance of continuing to improve orthopaedic skills education and assessment cannot be overstated.
Central to the development of a successful skills program is the incorporation of metrics to track learner progress and growth. Simulation, unlike supervised patient care, allows for standardized assessment and grading, with the ability to repeat the exercise immediately after feedback. Ideally, task checklists and scoring rubrics should be used to standardize learner evaluation and measure competency.8 Likert scales also can be used to track learner satisfaction, with modules or individual components within modules.9 The efficacy of components of the skills program can then be cross-checked with clinical performance, especially if used in the setting of the recently recommended AAOS residency milestones initiative.10 In this way, both trainee ability and the reliability of the skills program can be continuously monitored and potentially improved upon. Of course, the acquisition and analysis of these data can be time consuming. However, these are the best ways to document and track improvement in both the learner and the simulation.
A number of different components can be incorporated into starting and maintaining an orthopaedic skills program. These include cadaver labs, casting and splinting workshops, suturing workshops, physical examination workshops, industry-sponsored workshops, and virtual experiences, to name a few. The number of components immediately available to a specific program will be dependent on that program’s individual resources.
Creating an Orthopaedic Skills Program
At this institution, which supports a large orthopaedic residency program and a number of subspecialty fellowships, several steps were identified for starting and maintaining a skills program. The steps included (1) enlisting support from physicians, educators, administrators, and trainees at the institution; (2) partnering with the medical school for use of their clinical skills laboratories and other patient programs; (3) building ethical industry relationships for funding, resources, and additional bioskills laboratory use; (4) encouraging life-long learning habits in trainees by establishing formal journal clubs; (5) establishing a casting and splinting skills lab; and (6) combining virtual and hands-on surgical opportunities.
Step 1. Enlisting support from physicians, administrators, educators, and trainees
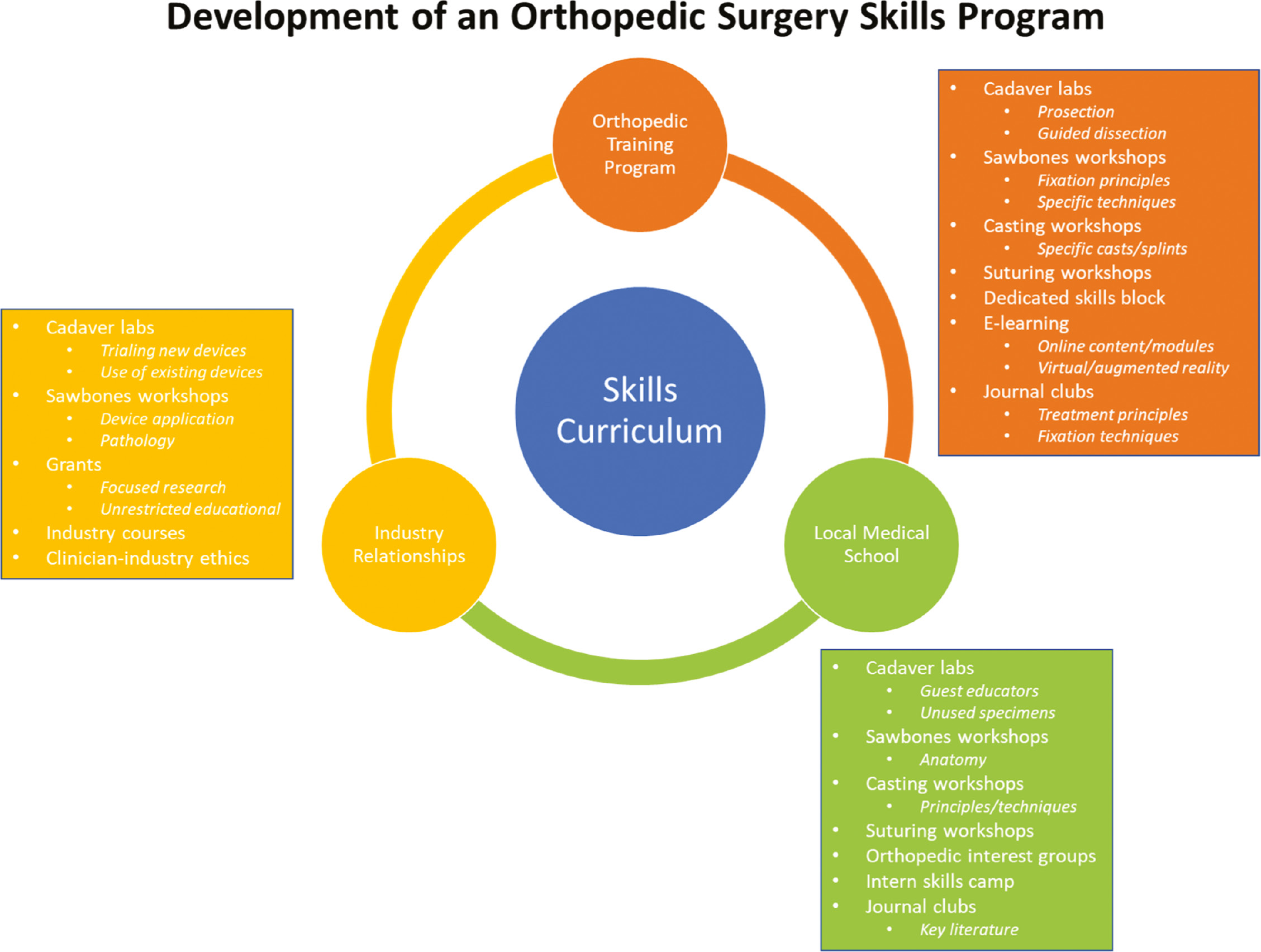
A successful orthopaedic skills program involves the use and interplay of a number of different available resources. The first step in building and incorporating a skills program into an orthopaedic surgery training program is to solicit feedback and commitment from those involved. Discussion on logistics, availability of educators, and start-up costs versus available funds will not only help to ensure there is appropriate impetus behind the teaching initiative but also will help to tailor the skills curriculum to the specific needs of the training program. At present, cost remains the greatest barrier to the adoption of surgical skills laboratory and/or curricula, with time constraint coming in as a close second.2 Having a central person or group of people leading this initiative is quite helpful, and they should be open to exploring opportunities within the department as well as in the community, the local medical school, and industry (Figure 1).
Figure 1. The successful development of an orthopaedic surgery skills program involves creative utilization of available institutional and regional resources—often with an exchange between groups and activities.
Given the amount of coordination and collaboration involved in developing a skills curriculum, it is highly recommended that detailed calendar schedules be constructed to ensure comprehensive coverage of topics and appropriate utilization of resources at appropriate times (Figure 2).11
Figure 2. A calendar of events can help to keep surgical skills training organized, comprehensive, and efficient. Adapted from Karam et al. IOJ 2013.11.

Alternatively, one could consider a curriculum that is spread out over the course of a year. If so, beginning with casting and splinting workshops for the same reasons as previously discussed is recommended. Although structure is important to standardizing education, attention to ever-present educational opportunities is also imperative as detailed in the rest of this article.
Enthusiastic education begins with enthusiastic educators. The source of eager and willing educators can be quite varied. Younger physicians who are less removed from their own training experience can bring a fresh perspective and energy to the skills program. Alternatively, more experienced providers who are winding their practice down and have the time to spend with trainees can offer a wealth of knowledge and expertise. Additional resources for educators exist within the graduated experience structure of orthopaedic surgery training programs themselves. Fellows or senior-level residents can serve as instructors for more junior learners or even among each other. The sharing of clinical knowledge between various members of the surgical department has the added benefit of creating an overall environment that is conducive to asking questions and learning.
Step 2. Partnering with medical schools
In addition to being a valuable part of the orthopaedic educational process, a local medical school can serve as an excellent partner in developing new resources or exploring existing ones. Existing cadaver dissection tools, tables, and facilities, which are utilized for anatomy or research purposes, can be incorporated into formal orthopaedic dissection opportunities. Cadavers remain one of the most clinically useful but also the most expensive sources of surgical education.2 By closely coordinating with medical student dissections, unused cadaveric specimens can be used for a number of orthopaedic dissections and/or procedures. Careful planning as to specific medical school uses and needs can assure a more formal experience for orthopaedic learners, including pre-planned or real-time prosections, learner dissections, or even procedural assessment with scoring rubrics. Numerous digits on the same specimen offer multiple attempts at the same procedure (such as metacarpal pinning), thus offering opportunities for adjustment to the learning curve and incorporation of additional techniques. Furthermore, orthopaedic trainees in turn can serve to guide medical students through surgical exposures and anatomy training during their planned cadaver procedures. In this way, both medical students and orthopaedic trainees gain a greater appreciation for anatomy and make full use of a precious resource.
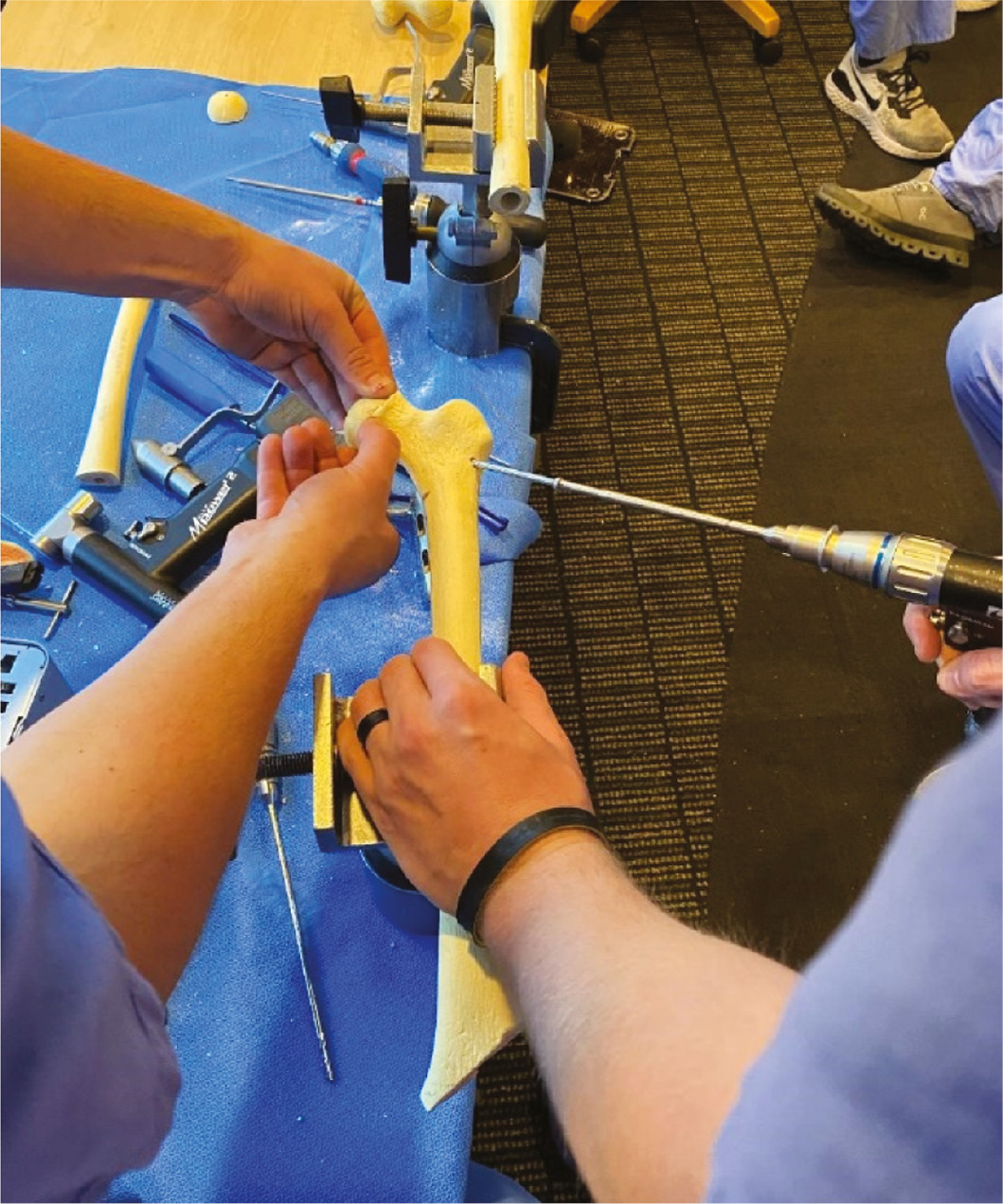
In addition to cadaver resources, medical schools can offer other basic surgical educational resources such as suturing trainers that teach basic knot tying and suture principles to new trainees and advanced suturing techniques to more experienced learners. Sawbones workshops serve as excellent means to educate trainees on both basic fixation principles and critical aspects of procedures (Figure 3). Standardized patients, now frequently employed by medical schools, offer orthopaedic trainees opportunities to enhance their clinical acumen as well as improve patient-provider interactions.12 Patient simulators, which are gaining in popularity, can be used to simulate critical care and/or patient stabilization scenarios. This will help prepare orthopaedic trainees for unforeseen hurdles and complications when managing medically unstable patients. As discussed later in this article, virtual reality trainers have been increasing in popularity in surgical training programs, particularly related to endoscopic and laparoscopic surgery. Other fields, such as general surgery or obstetrics and gynecology, may already have high-fidelity training tools that can be used to supplement the orthopaedic surgical skill set. This abundance of resources could already be available to orthopaedic training programs and could be revealed through a simple inquiry to the local medical school.
Figure 3. Hands-on simulation worships can help trainees to understand pathologies and develop operative skills.
Partnering with medical schools does not need to be a one-way relationship. Boot camp skills programs for interns have been shown to improve medical student satisfaction, preparedness, orthopaedic knowledge, program director evaluations, and match rates.8,13 By facilitating resident teaching and inclusion of medical students, residents learn teamwork and leadership skills, which they can carry forward into their future practices. Furthermore, better relationships between orthopaedic residency programs and medical schools can serve to not only improve the preparedness and candidacy of rising interns but can also help to increase the visibility of orthopaedics and attract even more talent to the field of orthopaedics.
Step 3. Ethically leveraging industry relationships
Developing a supportive and ethical relationship with medical device companies and other industry requires thoughtful and careful attention to how such agreements are structured and carried out. Orthopaedic surgery as a field has a longstanding history of close relationships with the medical device industry. Recently, much attention has focused on the potential bias from these relationships, and apparently such scrutiny is warranted. In 2018, the Center for Medicare & Medicaid reported industry payments totaling 9.35 billion dollars for all physicians,14 and orthopaedic surgeons made up a discordant 25.4% of these payments, in spite of representing only 3.4% of doctors receiving payments. The risk of bias certainly exists; however, developing principled, transparent relationships with industry lies at the heart of this matter, and well-thought-out arrangements can provide much-needed educational opportunities for residency programs, such as the use of cadaver dissection laboratories, non-sponsored conferences, and even workshops. Medical-device companies frequently employ mobile cadaver laboratories or visiting surgical workshops to educate surgeons on the various techniques associated with their products. Although geared toward practicing surgeons, these cadaver device demonstrations offer valuable opportunities for trainees to utilize existing cadavers and explore surgical approaches or anatomic dissections, saving the training program the added expenses of acquiring, storing, and maintaining additional cadaveric specimens (Figure 4).
Figure 4. Industry-sponsored cadaver labs to trial new technologies provide excellent opportunities for trainee education.

In addition to formal conferences and workshops, many educational grants are available through industry, including unrestricted grants that dictate no specific restraints on how the funds are used, avoiding potential perceived conflicts of interest. These grants allow for programs to provide educational and/or research opportunities without being restricted to a specific implant or system. Instead of distancing educational programs from industry, programs should use this as an opportunity to teach and demonstrate ethical associations.
Step 4. Supporting life-long learning habits in trainees
Journal clubs allow departments and/or divisions to come together to share and exchange ideas and knowledge. Aside from the communal benefits of these extracurricular academic endeavors, commonly described goals of orthopaedic journal clubs include the teaching of critical appraisal skills, the enhancement of clinical practice, and assimilation of current literature.15 Regarding surgical skills, such meetings facilitate the discovery and incorporation of new trainee skills and techniques. These thoughtful discussions are particularly valuable in pediatric orthopaedics, where numerous closed, percutaneous, and open reduction techniques are described in the treatment of individual conditions. It is important that these experiences function as positive educational opportunities and not arduous after-hours commitments. In this institution’s experience, quarterly journal clubs strike the right balance between frequency of events and learner engagement.
Useful in their own right, journal clubs can also serve as a beneficial time when educators and trainees are brought together outside of clinical duties. This time can be further used to advance clinical skills. Consider combining journal clubs with hands-on clinical activities such as cadaver or sawbone labs, or physical examination workshops. Combining journal clubs with industry-sponsored educational events also can help offset costs of the event while broadening educational opportunity.
Step 5. Establishing a casting and splinting lab for medical students and residents
In spite of the increasing rates of operative management of common orthopaedic injuries, casting and splinting remain core orthopaedic skills. Although generally viewed as “conservative” and noninvasive treatment, casting is not without its complications. Especially in pediatric orthopaedics, cast application remains very much in the “art of medicine,” with high variability in technique and skill level between practitioners. Perhaps because of the increasing trends toward surgery, the focus on appropriate splint and cast application appears to be diminishing. In one recent study, a mere 31% of faculty and 26% of residents rated splinting as a “must-know” skill.16 Another study reported that as many as half of all hand splints applied in the emergency department were rated as inappropriate, but with educational intervention, appropriateness of these splints improved to 70%.17 Casting and splinting workshops are especially pertinent to pediatric orthopedists as malpractice claims regarding cast issues rule in favor of the plaintiff 35% of the time, with a mean indemnity payment of $101,568.18
When designing a casting and splinting workshop, a curriculum should be built around the most common casts and splints used in the emergency room setting. These workshops provide the basic techniques from which trainees can further develop the skills required for more complicated casts and splints. A core set of casts and splints for a designated workshop allows for consistent cast assessment and grading and maintains a small and manageable list of materials that minimizes time and cost. Inclusion of the following casts and splints are recommended for a casting workshop: short arm, long arm, and short leg. Additional time at the end of the session can be dedicated to more complex casts or splints, such as the coaptation splint or the various finger/thumb immobilization splints. A casting supply list with a breakdown in cost is shown in Table 1. Cost per splint is further broken down in Table 2.
Table 1. Cast Workshop Material Cost (in USD, Prices from Year 2022)
| Material | Qty | Unit | Cost/Unit ($) | Total Cost ($) | Cost/Each ($) |
|---|---|---|---|---|---|
| 3×38” Orthoglass Splint | 3 | Boxes | 81.48/Box (10 Slabs) | 244.14 | 8.15/Splint |
| 4×38” Orthoglass Splint | 3 | Boxes | 88.42/Box (10 Slabs) | 265.26 | 8.84/Splint |
| 2” Fiberglass Rolls | 3 | Boxes | 21.59/Box (10 Rolls) | 107.95 | 2.16/Roll |
| 3” Fiberglass Rolls | 5 | Boxes | 25.15/Box (10 Rolls) | 125.75 | 2.52/Roll |
| 4” Fiberglass Rolls | 5 | Boxes | 32.39/Box (10 Rolls) | 161.95 | 3.24/Roll |
| 3” Kling Gauze | 3 | Boxes | 49.50/Box (12 Rolls) | 178.50 | 4.13/Roll |
| 4” Kling Gauze | 3 | Boxes | 49.50/Box (12 Rolls) | 178.50 | 4.13/Roll |
| 3” Stockinette | 1 | Box | 16.95/Roll (25 Yards) | 0.68/yard | 0.27/Foot |
| 4” Stockinette | 1 | Box | 16.95/Roll (25 Yards) | 0.68/yard | 0.27/Foot |
| 3” Webril Cast Padding | 3 | Bags | 13.31/Bag (12 Rolls) | 39.93 | 1.11/Roll |
| 4” Webril Cast Padding | 3 | Bags | 18.54/Bag (12 Rolls) | 44.62 | 1.55/Roll |
| 3” Coban | 2 | Bags | 32.28/Bag (24 Rolls) | 64.56 | 1.35/Roll |
| TOTAL: $1,391.50 | |||||
Table 2. Cost and Materials per Cast/Splint
| Cast/Splint Type | Material | Quantity | Cost/Material ($) | Total Cost ($) |
|---|---|---|---|---|
| Long Arm Cast | Stockinette | 1 Foot | 0.27 | 11.16 |
| Webril Cast Padding | 3 Rolls | 3.33 | ||
| 2” Fiberglass | 3 Rolls | 7.56 | ||
| Short Arm Cast | Stockinette | 1 Foot | 0.27 | 6.81 |
| Webril Cast Padding | 2 Rolls | 2.22 | ||
| 2” Fiberglass | 2 Rolls | 4.32 | ||
| Long Arm Splint | Stockinette | 1 Foot | 0.27 | 17.92 |
| Webril Cast Padding | 3 Rolls | 3.33 | ||
| 4”×38” Orthoglass Splint | 1 Slab | 8.84 | ||
| Kling Gauze | 1 Roll | 4.13 | ||
| Coban or ACE Wrap | 1 Roll | 1.35 | ||
| Short Leg Splint | Stockinette | 1 Foot | 0.27 | 31.55 |
| Webril Cast Padding | 3 Rolls | 3.33 | ||
| 4”×38” Orthoglass Splint | 1 Slab | 8.84 | ||
| 3”×38” Orthoglass Splint | 1 Slab | 8.15 | ||
| Kling Gauze | 2 Rolls | 8.26 | ||
| Coban or ACE Wrap | 2 Rolls | 2.70 | ||
| Short Leg Cast | Stockinette | 1 Foot | 0.27 | 13.32 |
| Webril Cast Padding | 3 Rolls | 3.33 | ||
| 4” Fiberglass | 3 Rolls | 9.72 | ||
| Sugar Tong Splint | Stockinette | 1 Foot | 0.27 | 15.88 |
| Webril Cast Padding | 3 Rolls | 3.33 | ||
| 3”×38” Orthoglass Splint | 1 Slab | 8.15 | ||
| Kling Gauze | 1 Roll | 4.13 | ||
| Coban or ACE Wrap | 1 Roll | 1.35 | ||
| Short Arm Splint (Volar/Dorsal, Radial Gutter, Ulnar Gutter, etc.) | Stockinette | 1 Foot | 0.27 | 17.92 |
| Webril Cast Padding | 3 Rolls | 3.33 | ||
| 4”×15” Orthoglass Splint | 1 Slab | 8.84 | ||
| Kling Gauze | 1 Roll | 4.13 | ||
| Coban or ACE Wrap | 1 Roll | 1.35 | ||
Casting workshops are particularly helpful early in the academic year with a focus on early trainees because splinting and casting will comprise a large proportion of the emergency department volume where these trainees spend a significant portion of their time. A casting workshop also provides a terrific opportunity to involve more advanced trainees in the education of junior residents, medical students, and even primary care or emergency department colleagues (Figure 5).
Figure 5. Casting and splinting workshops represent excellent opportunities to educate orthopaedic trainees and medical students on closed fracture management.

In addition to cast application, operation of a cast saw is also a very important component of a casting workshop. Cast burns are common and completely avoidable sequelae of cast management. Bae et al. evaluated total healthcare costs in a small series of pediatric patients who experienced cast saw burns.19 With a baseline incidence of 4.3% and a treatment/indemnity cost-per-case ranging from $2,995 to $25,000, they showed a potential return on investment of 11 to 1 on a cast-saw training program. Each cast application provides a potential educational opportunity for safe and appropriate use of a cast saw.
Step 6. Combining hands-on and virtual-education opportunities
As previously mentioned, a number of high-fidelity learning platforms and simulators exist in the sphere of orthopaedic education. The use of virtual reality (VR) trainers in surgical skills has recently been extensively explored, with a number of studies confirming the transfer of skills from VR to the operating room (OR).20 VR trainers have been developed for a number of orthopaedic surgical simulations, including arthroscopic surgery (Figure 6), arthroplasty, and internal fixation.21–23 Although the transfer of skills through these high-fidelity trainers has been explored, the efficacy and retention rate of skills developed as part of their use is still being investigated.24
Figure 6. Arthroscopic simulators provide a computerized platform (left) with a number of interchangeable surgical trainers (right), including shoulder, knee, and hip arthroscopy.

Internet-based electronic learning (e-learning) has been gaining popularity in recent years. With the growing use of virtual meeting technologies and the rising popularity of virtual reality, e-learning will continue to become an increasing component of trainee education. E-learning has been studied in orthopaedic education, with both learners and educators demonstrating satisfaction with internet-based educational tools.25 The combination of e-learning and traditional face-to-face education (blended learning) has been shown in some instances to improve learner scores, with some evidence that e-learning is best-suited as a precursor to bedside learning.26 More recently, blended learning has been employed for remote skills modules in the setting of COVID-19 educational restrictions.9 Although blended learning has shown promise in enhancing orthopaedic medical education, as of yet little evidence exists for the direct translation of blended learning into practical clinical skills.27
With duty-hour restrictions and potentially fewer opportunities for trainees to provide patient care, there is ongoing concern for additional activities that may infringe upon valuable direct patient care educational opportunities. Blended learning may provide training institutions a solution to time concerns by allowing trainees to complete e-learning at a time more convenient to them, allowing them to spend their time within the hospital to focus on skill reinforcement and patient care. This principle of the flipped classroom, whereby pre-session educational materials are used to reinforce in-person workshops, is gaining traction in medical education. The concept has been applied to the surgical clerkship to great effect, with an over 90% excellent or outstanding learner rating of a simulation-based flipped classroom curriculum.28 An in-depth video lecture and tutorial of how to implement the flipped classroom in medical education is available online.29
Blended learning appears to be most popular with trainees, demonstrating higher learner motivation, subjective learning gains, and satisfaction with the learning process. Educators, however, may be more recalcitrant to the changes that accompany blended learning.30,31 Some of this discordance may be attributable to the decreased interpersonal interactions associated with more time dedicated to e-learning. Still yet, there may be some skepticism or dissatisfaction among the educators with learning processes that are unfamiliar to them. It is somewhat ironic that a rate-limiting step in the blended learning process may be first educating the educators. Regardless, physicians remain a versatile and adaptive population when it comes to education, and further investigations on this front will undoubtedly yield greater improvements in medical education.
Summary
Orthopaedic surgical training is rapidly evolving. The pressures of duty-hour restrictions and limits placed on graduated autonomy make simulation training an important component of trainee education and skill development. Starting and building a clinical skills program for orthopaedic trainees can at first seem daunting, but it does not necessarily have to be prohibitively expensive or time consuming. Program directors should leverage local resources and invested partners, including local medical schools, enthusiastic staff surgeons, and medical-device manufacturers. Trainees of all levels should be considered and incorporated whenever possible to maximize teaching benefit and provide teaching opportunities for more experienced learners. Thoughtful planning, such as a calendar of events, can help to capitalize on available opportunities. Quarterly journal clubs are ideal, incorporating a clinical skills portion or lab as often as possible. Creating a surgical skills training program does not mean that a large array of high-fidelity models and virtual reality simulators must be procured. Although these are certainly options available to some programs, much more cost-effective and readily available options exist. A bit of creativity and dedication are all that are needed to put a program on a path toward a successful simulation program.
Disclaimer
No funding was received. K. Miller and B. Sheffer: No conflicts of interest to disclose. D. Kelly: Elsevier royalties.
References
- Reznick RK, MacRae H. Teaching surgical skills – changes in the wind. N Engl J Med. 2006;355(25):2664-2669.
- Karam MD, Pedowitz RA, Natividad H, et al. Current and future use of surgical skills training laboratories in orthopaedic resident education: a national survey. J Bone Joint Surg Am. 2013;95(1):e4.
- Jain NPM, Jowett AJL, Clarke NMP. Learning curves in orthopaedic surgery: a case for super-specialization? Ann R Coll Surg Engl. 2007;89(2):143.
- Riedel BB, Mildren ME, Jobe CM, et al. Evaluation of the learning curve for reverse shoulder arthroplasty. Orthopedics. 2010;33(4). doi:10.3928/01477447-20100225-09.
- Sodhi N, Khlopas A, Piuzzi NS, et al. The learning curve associated with robotic total knee arthroplasty. J Knee Surg. 2018;31(1):17-21.
- Gonzalvo A, Fitt G, Liew S, et al. The learning curve of pedicle screw placement: how many screws are enough? Spine (Phila Pa 1976). 2009;34(21):E761-E765.
- Immerman I, Kubiak EN, Zuckerman JD. Resident work-hour rules: a survey of residents’ and program directors’ opinions and attitudes. Am J Orthop. 2007;36(12):E172-E179; discussion E179.
- Sonnadara RR, Van Vliet A, Safir O, et al. Orthopedic boot camp: examining the effectiveness of an intensive surgical skills course. Surgery. 2011;149(6):745–749.
- Bhashyam AR, Dyer GSM. “Virtual” boot camp: orthopaedic intern education in the Time of COVID-19 and beyond. J Am Acad Orthop Surg. 2020;28(17):e735-e743.
- Ames SE, Ponce BA, Marsh JL, et al. Orthopaedic surgery residency milestones: initial formulation and future directions. J Am Acad Orthop Surg. 2020;28(1):E1-E8.
- Karam MD, Westerlind B, Anderson DD, et al. Development of an orthopaedic surgical skills curriculum for post-graduate year one resident learners – the University of Iowa experience. Iowa Orthop. 2013;33:178-184.
- Taormina DP, Zuckerman JD, Karia R, et al. Clinical skills and professionalism: assessing orthopaedic residents with unannounced standardized patients. J Surg Educ. 2018;75(2):427-433.
- Yu HH, Lockwood WC, Shaw KG, et al. Formal orthopaedic surgery “boot camp” curriculum to optimize performance on acting internships. J Am Acad Orthop Surg. 2022;30(6):247-254.
- Dougherty PJ. CORR® curriculum—orthopaedic education: teaching the intricacies of the surgeon-industry relationship. Clin Orthop Relat Res. 2020;478(2):225.
- Dirschl DR, Tornetta P, Bhandari M. Designing, conducting, and evaluating journal clubs in orthopaedic surgery. Clin Orthop Relat Res. 2003;413(413):146-157.
- Fitch MT, Kearns S, Manthey DE. Faculty physicians and new physicians disagree about which procedures are essential to learn in medical school. Med Teach. 2009;31(4):342-347.
- McEvenue G, FitzPatrick F, von Schroeder HP. An educational intervention to improve splinting of common hand injuries. J Emerg Med. 2016;50(2):228-234.
- Oetgen ME, Parikh PD. Characteristics of orthopaedic malpractice claims of pediatric and adult patients in private practice. J Pediatr Orthop. 2016;36(2):213-217.
- Bae DS, Lynch H, Jamieson K, et al. Improved safety and cost savings from reductions in cast-saw burns after simulation-based education for orthopaedic surgery residents. J Bone Joint Surg Am. 2017;99(17):e94.
- Seymour NE. VR to OR: a review of the evidence that virtual reality simulation improves operating room performance. World J Surg. 2008;32(2):182-188.
- Logishetty K, Rudran B, Cobb JP. Virtual reality training improves trainee performance in total hip arthroplasty: a randomized controlled trial. Bone Joint J. 2019;101-B(12):1585-1592.
- Cannon WD, Nicandri GT, Reinig K, et al. Evaluation of skill level between trainees and community orthopaedic surgeons using a virtual reality arthroscopic knee simulator. J Bone Joint Surg Am. 2014;96(7):e57.
- LeBlanc J, Hutchison C, Hu Y, et al. A comparison of orthopaedic resident performance on surgical fixation of an ulnar fracture using virtual reality and synthetic models. J Bone Joint Surg Am. 2013;95(9):e60.
- Atesok K, Satava RM, van Heest A, et al. Retention of skills after simulation-based training in orthopaedic surgery. J Am Acad Orthop Surg. 2016;24(8):505-514.
- Citak M, Calafi A, Kendoff D, et al. An internet based learning tool in orthopaedic surgery: Preliminary experiences and results. Technol Health Care. 2009;17(2):141-148.
- Hull P, Chaudry A, Prasthofer A, et al. Optimal sequencing of bedside teaching and computer-based learning: a randomised trial. Med Educ. 2009;43(2):108-112.
- Back DA, Haberstroh N, Antolic A, et al. Blended learning approach improves teaching in a problem-based learning environment in orthopedics - A pilot study. BMC Med Educ. 2014;14(1):1-8.
- Liebert CA, Mazer L, Bereknyei Merrell S, et al. Student perceptions of a simulation-based flipped classroom for the surgery clerkship: a mixed-methods study. Surgery. 2016;160(3):591-598.
- Implementing a flipped classroom in medical education [Incl. Seminar] | Lecturio Medical. Available at: https://www.lecturio.com/pulse/implementing-a-flipped-classroom-in-medical-education/. Accessed April 29, 2022.
- Woltering V, Herrler A, Spitzer K, et al. Blended learning positively affects students’ satisfaction and the role of the tutor in the problem-based learning process: results of a mixed-method evaluation. Adv Health Sci Educ Theory Pract. 2009;14(5):725-738.
- Gray K, Tobin J. Introducing an online community into a clinical education setting: a pilot study of student and staff engagement and outcomes using blended learning. BMC Med Educ. 2010;10(1):6.