
JPOSNA® Special Edition
Advances in Pediatric Orthopaedic Education and Technical Training
High-Fidelity Simulation Training for Closed Reduction and Casting of Distal Radius Fractures
Department of Orthopaedics, Children’s Hospital of Philadelphia, Philadelphia, PA
Correspondence: J. Todd Lawrence, MD, PhD, Department of Orthopaedics, Children’s Hospital of Philadelphia, 3401 Civic Center Blvd., Philadelphia, PA 19142. E-mail: [email protected]
Received: June 2, 2022; Accepted: June 27, 2022; Published: August 15, 2022
DOI: 10.55275/JPOSNA-2022-0069
Volume 4, Number S1, August 2022
Introduction
Nonoperative management through closed reduction and immobilization is the mainstay of treatment for the majority of distal radius fractures in the pediatric and adolescent population.1–7 However, approximately one-third of the reduced distal radius fractures will re-displace, with 7% requiring additional treatment.4–11 While loss of reduction can be related to the fracture pattern, for simple fracture patterns, the major risk factors for re-displacement appear to be modifiable, namely inadequate reduction, poor cast molding, and inexperience of the caregiver.6–13
Fracture reduction and cast placement are core orthopaedic principles. In most institutions, these are performed in the emergency room by a junior resident without the direct supervision of an attending. Teaching and assessing technical competency of these skills while minimizing patient risk is, therefore, a challenging but essential component of residency training.14 The need for a consistent, reproducible training tool with high-face validity (realism of simulation) and the opportunity for objective feedback prompted us to develop a simple, yet realistic, model for distal radius fracture reduction and casting simulator.
We have been using this simulation training exercise since 2015. This is done annually with each new intern class in our residency program as part of a series of simulation training exercises to teach basic orthopaedic skills and help prepare them for independent emergency room call. The simulation allows for immediate feedback during the training module, and we have shown that it improves clinical care by reducing the number of reductions that re-displace early in a trainee’s time delivering independent care. Although it has the capability to also provide a quantitative discriminatory assessment of performance, we are not yet using it to assess competence prior to independent clinical care or using it longitudinally to evaluate trainee skill development over time.
Simulation Models
The training module involves a step-wise progression of models to (1) teach residents about the role of the periosteum in fracture displacement and reduction and (2) teach the typical maneuver to unlock and reduce a fracture. The first model demonstrates the effect of periosteum in the process of fracture reduction in a two-dimensional model. The second model is a low-fidelity model simulating the reduction maneuver for just the bony segments. The third model is an anatomic model of the forearm, wrist, and hand with simulated periosteum to help introduce the concept of ligamentotaxis. The final model is a high-fidelity model that incorporates simulated bone and periosteum with overlying soft tissue. It also incorporates deforming forces that require continued counter force with a well-molded cast to maintain the reduction, allowing learners to practice both the reduction maneuver and application of a well-molded cast to hold the reduction.
The first model is constructed from a flat and wide block of wood (approximately 0.5 × 3 inches) that is about 8 inches in length. The block is cut towards one end. A piece of rope is tethered around the circumference of the block with a gap on one side of the “fracture” to mimic the torn periosteum (Figure 1). The rope is left unattached on one side of the segments on the side of the “fracture” opposite the torn periosteum to mimic the stripped periosteum and allow for displacement of one segment relative to the other. A complete list of supplies needed to create this model is included in Appendix 1. This model is used to demonstrate the role of the periosteum in tethering the fracture fragments and the need to recreate the deformity to unlock the fracture fragments before the segments can be reduced. A slight angle to the cut in the block of wood can help mimic the effect of fracture obliquity relative to the area of the intact periosteum. This model demonstrates fracture reduction in a single plane as a way for learners to conceptualize the periosteum as a reduction aid.
Figure 1. A demonstration of the first model used in the simulation, consisting of a block of wood with an oblique saw cut in the middle. A rope is screwed in circumferentially around the block, with a gap on one side of the saw cut to simulate torn periosteum. (A) This model is used to demonstrate the role of the periosteum and the mechanism of fracture reduction, involving re-creating the deformity and traction (B), translation (C), and reduction (D).

We then use a second model to demonstrate these concepts three-dimensionally. This second model is constructed from a 0.75″ × 1.5″ × 10″ piece of wood with a transverse cut towards one end to mimic a distal radius fracture. A piece of sturdy cloth (canvas or even an OR towel) is glued circumferentially around the site of the saw cut. Care is taken to apply glue all the way up to the edges of the wood pieces except on the top of the end of the longer piece where the small piece will eventually sit when the “fracture” is displaced (Figure 2).
Figure 2. In constructing the second model, an OR towel or piece of canvas is glued to the “proximal” and “distal” pieces of wood, taking care to leave approximately 1.5 cm of the distal end of the “proximal” fragment unglued (delineated by marked line) to mimic periosteal stripping and allow the “distal” fragment to translate.

Once the glue is dry, the fabric is cut along the interface between the two pieces, starting on the bottom. Usually, the fabric must be split all along the bottom and then just a small amount up each side to allow the smaller fragment to fully displace. Leaving more fabric on the sides helps the fracture displace in such a way as to prevent reduction with direct longitudinal traction and instead, requires angulation of the fracture prior to translating the fragment back into position (Figure 3). A complete list of supplies needed to create this model is included in Appendix 1. Once created, this model is used to reinforce the role of periosteum in blocking the reduction and introduces the maneuvers used to “unlock” the fracture and reduce it. Learners are able to feel the segments directly in this model, something that they will not necessarily be able to feel as easily in the final simulation.
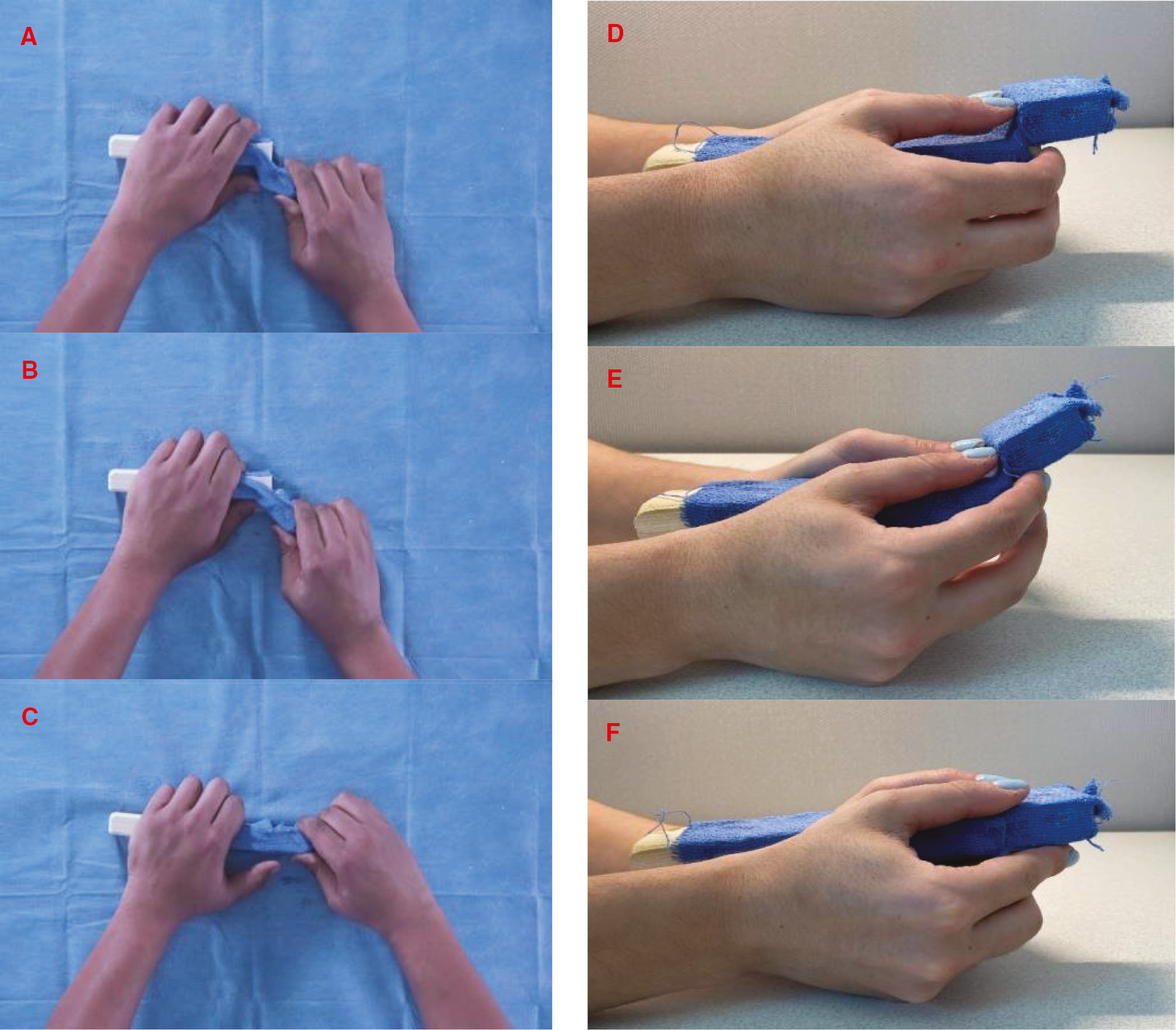
Figure 3. The second model similarly demonstrates the role of the periosteum in fracture reduction. An OR towel is glued around a cut block and then cut on one end. The nature of the model ensures that the “fracture” will not reduce with pure traction and requires re-creating the deformity first. Figures 3A–C demonstrate the first one, with a hand on each segment to control the proximal and distal fragments. Figures 3D–F demonstrate the other, stabilizing the proximal segment between the palms and the small and ring finger of both hands so that the index and long fingers can control angulation of the distal fragment while the thumbs push the distal fragment over the edge of the proximal fragment.
The next model is an anatomic model of the bones of a forearm, wrist, and hand (Sawbones, Vashon Island, WA) with a transverse cut through the distal radius (Sawbones SKU 1022-16; $85). This model is used to cement the concepts presented in the prior models while also introducing the concept of ligamentotaxis. Nylon webbing is glued on the dorsal part of the distal radius proximal to the fracture site up to about 1.5 cm away from the fracture site. The nylon webbing is then glued to the distal fragment and across the wrist joint. Wrapping the webbing through the metacarpals and back around to the distal aspect of fracture volarly helps secure the webbing better (Figure 4). Leaving a small amount of slack in the webbing as it passes over the radiocarpal joint helps solidify the concept that slight wrist flexion and ulnar deviation places the dorsal carpal ligaments on stretch and aids in control of the distal radial fragment when casting.
Figure 4. An anatomic Sawbones model with a short oblique fracture created in the distal radius. Taut nylon straps are glued across the wrist joint to simulate volar and dorsal carpal ligaments. Additionally, the nylon strap on the dorsal side also crosses the fracture line to simulate intact periosteum. This model allows learners to understand the concept of ligamentotaxis and practice typical hand positioning and manipulation for reduction. Figures 4A–C demonstrate the mechanism of fracture reduction involving the displaced fragment, angulation re-creating the deformity and traction, translation, and reduction.

Finally, we introduce the high-fidelity simulation model (Sawbones SKU 1530; $1575). The model was developed at The Children’s Hospital of Philadelphia with engineering assistance and model production performed by Pacific Research Laboratories Inc. (Sawbones, Vashon Island, WA). The internal skeleton of the model is constructed of synthetic radius and ulna bones mounted to an articulating hinge to simulate elbow joint flexion and extension. The bones are coated with radiopaque paint to allow for visualization with standard fluoroscopy. The arm is attached to a table clamp that allows for three planes of shoulder motion (flexion-extension, abduction-adduction, and internal-external rotation) and simulates the position of a patient who has been brought over to the edge of the table with their shoulder just off the edge of the bed (Figure 5).
Figure 5. Close up view of the clamp used to attach the simulation model to the OR table. A series of three hinges allow for motion in three planes and mimics motion at the shoulder for a patient who is positioned at the edge of the table with their arm off the table.

Monofilament radiopaque markers are embedded within the distal radius and a simple extra-articular transverse distal radius metaphyseal fracture is created using an extra-fine rotary bit. Nylon strapping is secured to the dorsal aspect of the distal radius to simulate periosteum as in the third model described above. This strap continues across the wrist joint to simulate the dorsal and volar wrist ligaments. Attachment points on the nylon strap are fashioned to simulate apex volar fracture displacement and to block reduction if the reduction was not adequately performed. As with the other models, the reduction requires sequential steps: re-creation of dorsal angulation, followed by pulling it out to length with traction, then displacement correction, and finally, angulation correction. An additional dynamically tensioned nylon cord is attached to the dorsal radial aspect of the distal radial fragment to simulate deforming forces from the brachioradialis. The inflection point of this dynamic displacing force is designed to allow for stable reduction with little force from a standard three-point mold if the fracture is reduced anatomically. However, release of this minimal force on an anatomically reduced fracture causes fracture angulation and displacement. The radiopaque markers allow for quantification of displacement and angulation during assessment (Figure 6).
Figure 6. Image of the simulation model under fluoroscopy. The bones are painted with radiopaque paint to be visible on x-ray. A radiopaque line marker is also placed across the site of fracture prior to the cut for students to better visualize alignment.

The model is covered with a high-quality polyurethane foam and silicone-based skin to allow for normal cast application. The bones and overall size of the limb is sized to be that of the average late adolescent. The model allows for motion at the elbow and shoulder and allows learners to practice reduction techniques in a way that is comparable to doing it on a patient in the emergency department.
Simulation Training Exercise
At our institution, this teaching session is typically done in the operating room on a weekday afternoon when case volumes decrease and C-arms and an operating room can be utilized for the simulation without impacting patient care. One instructor is usually able to teach four trainees in a 3-hour session. Trainees should ideally be proficient with standard casting techniques prior to participating in the simulation training. To prepare for the session, two high-fidelity models are clamped to a regular OR bed, one on each side. We usually use a regular C-arm on one side and a mini C-arm on the other side to allow trainees to become comfortable with positioning and maneuvering around both types of machines. C-arms are positioned coming in from the side of the bed on each end (Figure 7). The monitor for the regular C-arm is positioned at the end of the bed. Certified radiology technicians are engaged to ensure that the machines are utilized safely and properly through the exercise and full coverage wrap around lead is recommended.
Figure 7. Picture of the typical setup for the training. An OR room is utilized with two simulation models clamped on each side of the bed in opposite orientations. A C-arm is brought in from each side. We use one regular C-arm and one mini C-arm so learners can get comfortable with both. Groups are split into groups of two, with each person taking turns going through reduction and casting of the model while the other functions as an untrained assistant.

The exercise starts with the first model laid out flat on the table in a displaced position and trainees are asked to articulate the steps required to “reduce the fracture.” This model nicely illustrates the point that direct pull on the blocks along the long axis will not allow the edge of one piece to clear the other piece. Instead, the pieces must be angulated in such a way that the bottom edge of the displaced fragment can clear the top edge of the other fragment. This concept is articulated as the necessity to “recreate the deformity.” The exercise is completed when all learners can properly articulate the steps necessary to reduce a fracture, namely, recreate the deformity and translate the displaced fragment distally to the extent necessary to clear the end of the other fragment, correct displacement until the edges with the intact periosteum are lined up, then correct angulation until the segments are properly aligned (Figure 1). This model can also be used to illustrate how three points of force, one point on the side of the disrupted periosteum and two other points on the opposite corners, easily holds the fracture reduced but that it is quite unstable if this force is not applied. Learners should articulate this as the basis for the three-point mold that they will eventually use for holding the fracture reduced.
The next exercise utilizes the low-fidelity wooden replica of a distal radius fracture with cloth-based periosteum. The model is presented to the learner in the displaced configuration, and they are asked to reduce the fracture through direct manipulation of the segments. We usually teach them two different techniques, one with a hand on each segment and another stabilizing the proximal segment between the palms and the small and ring finger of both hands so that the index and long fingers can control angulation of the distal fragment while the thumbs push the distal fragment over the edge of the proximal fragment (Figure 8). This exercise allows the learner to directly receive the haptic feedback of the fracture reduction process. The exercise is complete when all learners can easily demonstrate competency reducing (and subsequently re-displacing) the fracture using both techniques. At the end of this exercise, learners are asked to demonstrate how and where a three-point mold would be applied to keep the fracture perfectly reduced.
Figure 8. A demonstration of the two techniques taught to trainees. Figure 8 demonstrates the two techniques used to reduce the fracture using direct manipulation as they are taught to trainees. These techniques are illustrated in greater detail in Figure 3.

The third exercise utilizes the forearm, wrist, and hand model. Following up on the three-point mold question from the last exercise, learners are then asked how they would apply the three points of force to a forearm of a patient to hold the fracture reduced given the small size of the distal segment of a distal radius fracture. Learners should be led by additional prompting to articulate that cast materials cannot usually be molded to create points of force small enough to directly target the dorsal aspect of the distal fragment and the volar fracture site but even if they could, that the underlying soft tissues would be injured by such sharp molds. They are then asked how they plan to control the distal segment of bone once they obtain the reduction. Learners should be led by additional prompting to articulate the concept that the dorsal radiocarpal ligaments can be placed on stretch with slight wrist flexion and ulnar deviation and that through this process of ligamentotaxis, the distal fragment can be controlled. This part of the training usually just involves demonstrating that the reduction is completely stable, with the model held in a palm down position, but that force applied in any other direction causes significant instability. Learners can then be informed that the model that they are about to manipulate has essentially the same setup, with the addition of overlying soft tissue and deforming forces.
The bulk of the time during the training is spent working with the high-fidelity model. The four learners are split into two-person teams. One participant from each team is instructed to perform a reduction on the model and then place a short arm cast that is molded to hold the reduction. Their teammate is advised to try to simply function as an assistant in this process, only doing what they are specifically instructed to do. Although not the main purpose of the simulation, this setup allows the learners to consider and practice other practical concerns that they may encounter in the emergency department, such as collecting and having all needed supplies on hand and within reach, patient and imaging positioning, and directing and supervising an untrained assistant. Usually, minimal guidance is provided to the learner during the simulation, allowing learners to troubleshoot and make decisions by themselves. Final x-rays are obtained in the cast. After the first cast on both models is cured, a group debrief is performed asking learners to articulate things that went well and things that they could improve upon. The instructor then provides structured feedback on the performance, again highlighting things that the learners did well and providing suggestions on how they could improve their performance. The cast is removed and then the partners switch roles and repeat the exercise. Teams switch models after one to two rounds to practice using the other C-arm. Typically, improvements are noted with every iteration, requiring fewer attempts to obtain a satisfactory reduction and producing better molded casts. In a typical initial session, learners each place three to four casts and the entire simulation typically runs approximately 3 hours. A debrief is performed at the end of the simulation to go over teaching points.
We have previously studied the effect of this simulation training by retrospectively comparing distal radius fracture reductions treated by residents who underwent simulation training and those that did not. Patients treated by simulation-trained residents had less residual angulation, translation, and fracture re-displacement, indicating the efficacy of this training technique.15
Summary
Currently, the majority of distal radius reduction models use fractured synthetic bones. However, the lack of soft tissues lowers the fidelity of the simulation causing poor discriminative abilities between individuals of different experience levels. When soft tissues are incorporated into the model to increase haptic feedback, the outer shell of the model makes it difficult to accurately assess the adequacy of the reduction. Thus, while these models can provide biofeedback to develop a feel for the process of fracture reduction, they may not truly simulate the process of fracture reduction and casting. We thus sought to create a model that requires the learner to master all the steps of the process to achieve a good result. When combined with fluoroscopy, the simulation training with the fracture reduction model described here can recapitulate the entire process of distal radius fracture reduction and give the learner haptic and visual feedback on their reduction and casting performance in real time. The exercise also helps them think through some of the logistical challenges that they are likely to face with real patients. This is the first distal radius fracture model to incorporate this objective feedback, allowing the participant to appreciate the effectiveness of their reduction and casting technique.
Disclaimer
No funding was received for the publication of this manuscript. The authors have no conflicts of interest to report pertaining to this manuscript.
References
- Chung KC, Spilson SV. The frequency and epidemiology of hand and forearm fractures in the United States. J Hand Surg Am. 2001;26(5):908–915.
- Bae DS. Pediatric distal radius and forearm fractures. J Hand Surg Am. 2008;33(10):1911-1923.
- Rodriguez-Merchan EC. Pediatric fractures of the forearm. Clin Orthop Relat Res. 2005;(432):65–72.
- Ryan LM, Teach SJ, Searcy K, et al. Epidemiology of pediatric forearm fractures in Washington, DC. J Trauma. 2010;69(4 Suppl):S200-S205.
- Chapman DM, Hayden S, Sanders AB, et al. Integrating the Accreditation Council for Graduate Medical Education Core competencies into the model of the clinical practice of emergency medicine. Ann Emerg Med. 2004;43(6):756-769.
- Jones K, Weiner DS. The management of forearm fractures in children: a plea for conservatism. J Pedimat Orthop. 1999;19(6):811-815.
- Perished J, Williams S, Wan J, et al. Pediatric distal radial fractures treated by emergency physicians. J Emerg Med. 2009;37(3):341-344.
- Pretell Mazzini J, Rodriguez Martin J. Paediatric forearm and distal radius fractures: risk factors and re-displacement--role of casting indices. Int Orthop. 2010;34(3):407-412.
- Haddad FS, Williams RL. Forearm fractures in children: avoiding redisplacement. Injury. 1995;26(10):691-692.
- Proctor MT, Moore DJ, Paterson JM. Redisplacement after manipulation of distal radial fractures in children. J Bone Joint Surg Br. 1993;75(3):453-454.
- Alemdaroglu KB, Iltar S, Cimen O, et al. Risk factors in redisplacement of distal radial fractures in children. J Bone Joint Surg Am. 2008;90(6):1224-1230.
- Roy DR. Completely displaced distal radius fractures with intact ulnas in children. Orthopedics. 1989;12(8):1089-1092.
- Sharma S, Bowe D, Walters SJ, et al. Dorsal cortical comminution as a predictor of redisplacement of distal radius fractures in children. Injury. 2010;42-2:173-177.
- Scott DJ, Cendan JC, Pugh CM, et al. The changing face of surgical education: simulation as the new paradigm. J Surg Res. 2008;147(2):189-193.
- Jackson TJ, Shah AS, Buczek MJ, et al. Simulation training of orthopaedic residents for distal radius fracture reductions improves radiographic outcomes. J Pediatr Orthop. 2020;40(1):e6-e13.
Appendix
Appendix 1. Materials for Models 1 and 2
- Blocks of wood: $3–$5
- Nylon Rope (50 ft): $5
- Nails (0.5in): $5
- Tape: $4–$5
- Hand saw (if unable to borrow one): $10
- Hammer (if unable to borrow one): $10
- Gel Superglue: $2–$6
- OR towel or canvas fabric (if unable to use extra from the OR): $10
- Scissors (if unable to borrow a pair): $6
Total: $55–$62