JPOSNA® Special Edition
Advances in Pediatric Orthopaedic Education and Technical Training
Integrating Simulation for Developing Pediatric Supracondylar Humeral Fracture Reduction and Fixation Skills into an Orthopaedic Surgery Residency Program
1Department of Orthopedics and Rehabilitation, University of Iowa, Iowa City, IA; 2Department of Biomedical Engineering, University of Iowa, Iowa City, IA; 3Department of Industrial and Systems Engineering, University of Iowa, Iowa City, IA
Correspondence: Joshua B. Holt, MD, Department of Orthopedics and Rehabilitation, 200 Hawkins Drive, Iowa City, IA 52242. E-mail: [email protected]
Received: June 3, 2022; Accepted: June 27, 2022; Published: August 15, 2022
DOI: 10.55275/JPOSNA-2022-0070
Volume 4, Number S1, August 2022
Introduction
Supracondylar humeral fractures are the most common fracture managed with surgical intervention in the pediatric population.1 There is a well-described trend for these injuries to be transferred to tertiary care centers and managed by orthopaedic surgeons with pediatrics subspecialization/expertise.2,3 As such, academic providers involved in orthopaedic resident education must have confidence in the resident teams who help to manage these injuries. Orthopaedic residents and fellows are experiencing increased exposure to these injuries and are expected to develop proficiency in their surgical treatment.
It has previously been reported that “the gap between surgeons who can and cannot pin an elbow increases every year,”4 and it is important that a similar trend does not occur amongst residents while obtaining their training at differing teaching institutions. There is a strong demand and critical need for improved resident training on the appropriate reduction and fixation techniques in a safe, encouraging, and reproducible environment in an effort to promote competency in the operating room when real patient function, safety, and long-term outcomes are at stake. The American College of Graduate Medical Education (ACGME) has steadily placed increased emphasis on the development of improved techniques for resident education and skills assessment. In this light, the development and widespread adoption of surgical simulation is ever increasing across all surgical fields. This includes the advancement of pediatric supracondylar humeral fracture reduction and fixation simulation models.
The thoughtful evolution of orthopaedic resident education and skills assessment has been a long-standing goal at the University of Iowa. Clinical faculty and research personnel have pioneered the creation and advancement of a novel pediatric supracondylar humeral fracture simulator. Through state-of-the-art calibration techniques, the model can simply, yet realistically, provide real-time training and immediate feedback on the assessment, reduction, and fixation of a pediatric supracondylar humeral fracture, without the necessity of fluoroscopic imaging. Through repeated exposure to the methods of reduction, wire navigation for proper placement, and functional assessment of specific aims, the simulation model can provide feedback that cannot be obtained in a live operating room setting.
Surgical simulation of pediatric supracondylar humeral fractures provides orthopaedic residents an ideal setting to develop and refine their surgical technique to a defined level of proficiency. Multiple biomechanical models have demonstrated that wire positioning is important for construct stability, including overall wire spread relative to fracture plane morphology.5,6 Understanding the 3D relationship between the bony anatomy and wire navigation is a necessary skill for proficient orthopaedic surgeons to develop. The high frequency of these injuries, requiring surgical fixation at academic institutions, allows for repetitive surgical exposure and assessment of skill development over the course of a typical orthopaedic training program. Through refinement of surgical techniques developed on a pediatric supracondylar humeral fracture model, all residents trained in this manner would be expected to be proficient and safe when performing the basic principles of surgery prior to experiencing them in the operating room. Surgeon confidence and skill can be increased while simultaneously decreasing operative time, radiation exposure, and potentially improving patient outcomes.
Simulator Overview
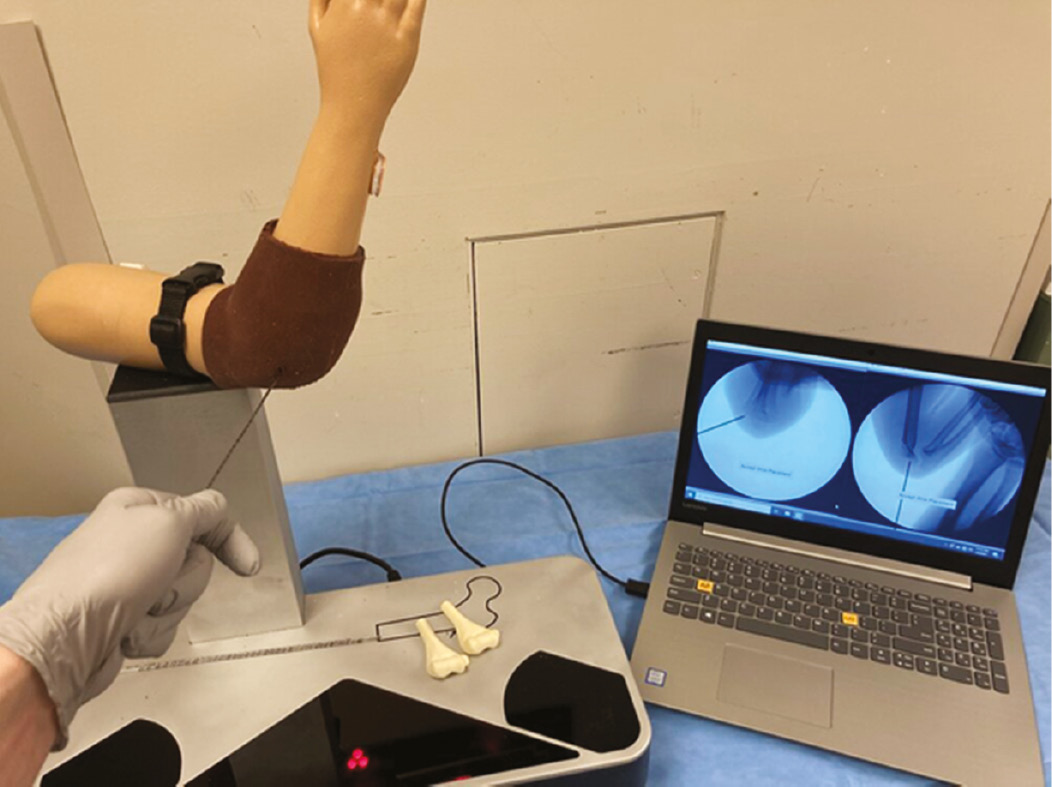
A novel camera system was developed in conjunction with a pediatric supracondylar humeral fracture 3D model, as shown in Figure 1. The camera system allows radiation-free imaging to be obtained and mapped to the calibrated bony model at any time during simulation. A laser-etched wire with calibrated barcoding allows the camera system to determine the exact position of the wire in space, thereby providing immediate feedback of where the wire is in relation to the distal humerus anatomy. The sawbones model of the supracondylar humeral fracture with associated fabricated soft tissue envelope is aligned with previously obtained coordinating anterior/posterior and lateral fluoroscopic imaging on the computer screen. This allows for real-life feel and immediate tactile feedback of the wire entering the bony anatomy of the sawbones model while simultaneously providing the visual feedback of the wire depicted on the radiation-free “fluoro” image projected on the computer screen. Due to the calibrated system, the computer model knows where the wire is being drilled into the model and where the fracture plane lies. This allows for an automated scoring algorithm to provide immediate feedback regarding wire placement, trajectory, and overall wire spread relative to the fracture plane morphology. This data allows for comparison across and between various levels in training.
Figure 1. The pediatric supracondylar humeral fracture pinning simulator is shown here. To the right, the laptop displays AP and lateral “fluoro” images of the wire as it is positioned relative to the pediatric elbow model.
Implementation of Pediatric Supracondylar Humeral Fracture Pinning at Your Institution
Depending on the training program, the ideal timing of simulation training in supracondylar humeral fracture management can be variable. At the University of Iowa, the third-year orthopaedic residents are most often involved in surgical reduction and fixation of supracondylar humeral fractures due to our trauma call system. As such, we incorporate the simulator training into the final 6 months of the second year of residency, most likely within a few months of high-volume hands-on exposure to operative treatment of pediatric patients. As part of the overall curriculum, a pre-simulator training program involving an 8-minute informational video on the basics of supracondylar humeral fracture epidemiology, classification, surgical indications, and goals of fixation is completed by each resident. Upon completion of the video tutorial, each participant is taken through the simulator training curriculum by trained faculty and research personnel.
Each participant first performs a pre-assessment during which they are tasked with the placement of three lateral, divergent, multi-planar, bicortical wires into a pediatric distal humerus model with the wire starting point on the capitellum in the configuration shown in Figure 2. Participants are made aware of the measures being evaluated, which include procedure duration, the total number of “fluoroscopic” images obtained, number of wire redirections, and overall wire spread, with a goal AP wire spread of greater than one-third the distance of the fracture line (or fixation of at least two of the three columns of the distal humerus).7 Participants are free to obtain “fluoroscopic” AP and lateral imaging at any time and as often as they deem necessary during their pre-assessment simulation.
Figure 2. The goal wire configuration with representative AP and lateral images. Also demonstrates how wire spread ratio is calculated on the AP image, with a goal wire spread ratio of >1/3.

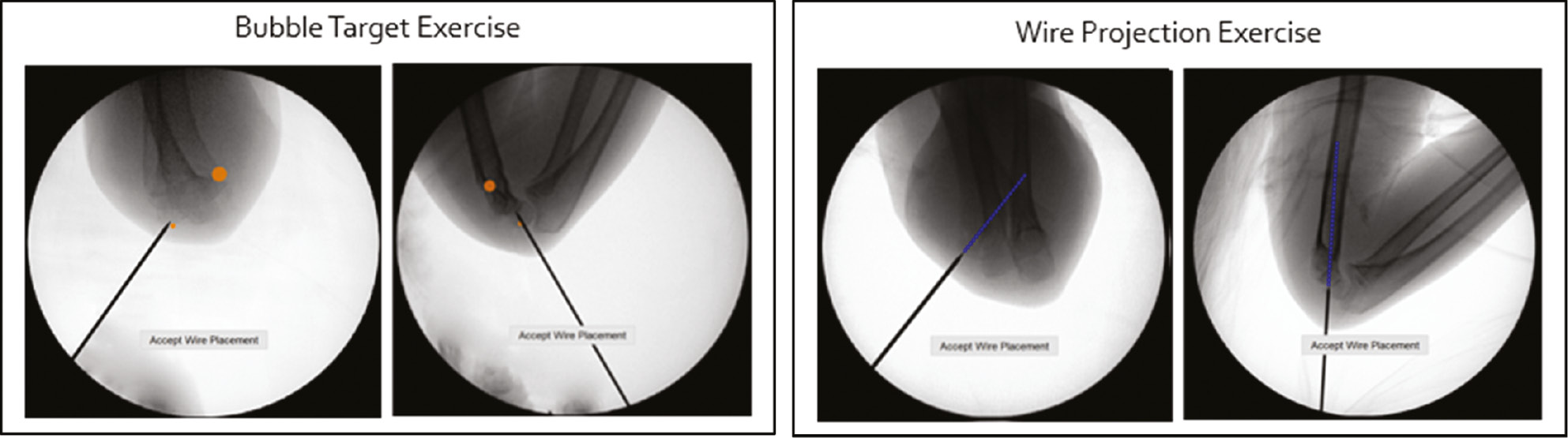
Following the pre-assessment, each participant is then taken through their simulation by faculty and their performance is reviewed. This includes a review of the objective data collected by the novel simulation model as well as any subjective feedback provided by the faculty observer. After the review is completed, all questions are answered and goals clarified, each participant is taken through two additional training modules on the simulator, focusing on overall wire navigation skills and ideal wire placement and trajectory (Figure 3). These modules are designed to provide understanding to the participant on how to develop the ideal three-wire construct and how to best understand the 3D trajectory of each wire placed in real-time. In the first training module, a series of bubble targets are overlaid on the AP and lateral images. These simulated targets are positioned such that the participant can “pop” the bubble with their wire if positioned appropriately. The resulting fixation construct will provide appropriate wire spread and multi-planar fixation in both AP and lateral planes. In the second training module, participants have a projected line emanating from the tip of their wire onto the “fluoroscopic” image. This further provides real-time, immediate visual feedback to the participant and allows a more precise visual understanding of where the wire will terminate if they choose to maintain the current path in the AP and lateral planes. Participants often find this added visualization extremely beneficial in planning their three-wire construct, particularly for those less experienced. Upon completion of all three training modules, the participants are then asked to perform a final post-training assessment. This is performed in a similar fashion to the pre-assessment, where a wire fixation construct composed of three, divergent, laterally placed pins is created and a similar objective assessment is made regarding procedure duration, images obtained, wire redirections, and overall wire spread. A final score of the simulation performance is calculated by combining the AP wire spread, the total time, and the total number of imaging shots obtained into a normalized value ranging from −1.5 to +1.5. This score is presented relative to a competency benchmark defined by data obtained from expert surgeons evaluated on the simulator. A comparison of results is made between pre- and post-training simulation outcomes.
Figure 3. Left: The first of three “bubble” targets can be seen. These targets provide guided positions for participants to place the wires when learning how to build a three-wire construct. Right: A projected line from the tip of the wire shows the path the wire will take in the bone if advanced in the current trajectory.
Resident Feedback
Residents at our institution complete a survey after participating in this training module and the results suggest that they have found working with the pediatric supracondylar humeral fracture simulation model very positive and beneficial (see Appendix 2). When surveyed on the realism of the simulator and associated tasks, residents graded the simulator an average of 4.3 out of 5. All residents involved have expressed that simulator training has significant benefit as an adjunct to their live operating room experience with supracondylar humeral fracture fixation. Participants report that the simulator improves their performance and increases their confidence in the operating room, scoring 4.8 and 4.5 out of 5, respectively.
Future Directions: Advanced Simulation Model with Fracture Reduction and Fixation
At the University of Iowa, we are currently integrating a new pediatric supracondylar humeral fracture simulator into the residency training program. The new simulator model is comparable to the one described above, only includes a true bony fracture that requires a realistic feeling reduction prior to wire fixation. The model is a hybrid reality simulator that replicates a fracture reduction and pinning procedure on an anatomically correct surgical model using actual operating room instrumentation. Tracking sensors are attached to the 3D printed synthetic bone model placed within an artificial soft tissue envelope (Figure 4). Bony specimens used for the simulation model are printed from patient computed tomography (CT) data, making them truly anatomic. An array of synthetic fractures is then manually produced in the models to create numerous fracture types of varying reduction difficulty. The use of CT data allows for the creation of accurate digitally reconstructed images which serve as the “fluoro” images during simulation exercises. This new simulation model incorporates all aspects of surgical management of supracondylar humeral fractures and provides real-feel fracture evaluation, reduction, fixation, and stability assessment in a safe, reproducible, radiation free environment. Immediate automated objective feedback is then available to the participant.
Figure 4. Pediatric supracondylar humeral fracture simulator with 3D printed bony anatomy, real-feel fracture reduction capabilities, true surgical instrumentation compatibility, and real-time radiation-free “fluoro” imaging available.

Disclaimer
Funding: 2018 POSNA Directed Research Grant, Amount $50,000. S. Long, M. Tatum, G. Thomas, D. Anderson, M. Karam: Part owner, Iowa Simulation Solutions, LLC. J. Holt and H. Kowalski: No conflicts of interest to disclose.
References
- Frick SL, Mehlman CT. The community orthopaedic surgeon taking trauma call: pediatric supracondylar humeral fracture pearls and pitfalls. J Orthop Trauma. 2017;31:S11-S15.
- Holt JB, Glass NA, Bedard NA, et al. Emerging U.S. national trends in the treatment of pediatric supracondylar humeral fractures. J Bone Joint Surg Am. 2017;99(8):681–687.
- Holt JB, Glass NA, Shah AS. Understanding the epidemiology of pediatric supracondylar humeral fractures in the United States: identifying opportunities for intervention. J Pediatr Orthop. 2018;38(5):e245-e251.
- Wenger DR. Practice in paediatric orthopaedics, Third Edition. J Pediatr Orthop. 2017;37(4):e302.
- Gottschalk HP, Sagoo D, Glaser D, et al. Biomechanical analysis of pin placement for pediatric supracondylar humerus fractures: does starting point, pin size, and number matter? J Pediatr Orthop. 2012;32(5):445-451.
- Skaggs DL, Hale JM, Bassett J, et al. Operative treatment of supracondylar fractures of the humerus in children: the consequences of pin placement. J Bone Joint Surg Am. 2001;83(5):735-740.
- Pennock AT, Charles M, Moor M, et al. Potential causes of loss of reduction in supracondylar humerus fractures. J Pediatr Orthop. 2014;34(7):691-697.
Appendices
Appendix 1. Program Costs
- The wire navigation simulator is manufactured by Iowa Simulation Solutions (www.iasimsol.com), a small startup company founded by University of Iowa research team members. Residency or Fellowship training programs can purchase a simulator package that includes the pediatric supracondylar humeral fracture module for $20,000. Other add-on modules (e.g., slipped capital femoral epiphysis, hip fracture DHS wire navigation, cephalomedullary nail guidance, iliosacral screw navigation) are available and new modules are in development.
- The surrogate bone models used with the pediatric module can be purchased from Sawbones (Vashon Island, WA) and are currently priced at $16.25 per bone (https://www.sawbones.com/humerus-pediatric-right-solid-foam-distal-segment-only-w-6mm-canal1052-2-1.html).
- The fracture reduction simulator is under final development with a company named FX-Systems and will be available to programs for purchase in the near future.
Appendix 2. Post OR Data Collection Survey