
JPOSNA® Special Edition
Advances in Pediatric Orthopaedic Education and Technical Training
Construction and Use of an Inexpensive, Free-Hand, Pedicle Screw Placement Model
1Department of Orthopaedic Surgery, Montefiore Medical Center, Bronx, NY; 2Division of Pediatric Orthopaedics, Children’s Hospital at Montefiore, Bronx, NY
Correspondence: Jacob Schulz, MD, Division of Pediatric Orthopaedics, Children’s Hospital at Montefiore, 3400 Bainbridge Ave., 6th floor, Bronx, NY, 10467. E-mail: [email protected]
Received: May 19, 2022; Accepted: May 22, 2022; Published: August 15, 2022
DOI: 10.55275/JPOSNA-2022-0060
Volume 4, Number S1, August 2022
Introduction
We have described and validated an inexpensive and reproducible model to practice the free-hand placement of pedicle screws.1 This model helps the learner develop the skills required to use procedure-specific surgical instruments and allows for the high-repetition practice necessary to become facile with those instruments.
Free-hand pedicle screw placement in spine surgery, described by Kim and Lenke, is an important, complex skill with a steep learning curve.2 Gang et al. reported that residents needed to place approximately 60 screws under direct supervision before they could independently insert a pedicle screw safely.3 Practicing free-hand placement of pedicle screws outside of the operating room allows for procedure-specific skill development in a controlled environment, decreasing the risk to the patient and increasing intra-operative efficiency and safety. While composite spine models and cadavers are valuable training tools and can be used for skill development, they are expensive and not readily available to all training surgeons. In addition, the combination of their high cost and limited availability does not allow for high-repetition practice.
Our resident skills training laboratory has prioritized the development of models that can teach the skills necessary to use the tools required for most orthopaedic procedures. Inexpensive, “low-fidelity” models allow for the high-repetition training needed to familiarize the learner with the tools themselves as well as develop the muscle memory necessary to repeat those skills reliably and accurately in any situation. This is similar to a baseball player’s use of a batting tee to hone a swing prior to swinging at a pitched ball in practice or a game. The pedicle screw placement model (PSPM) was developed at our institution in 2017 to provide an inexpensive training model that allowed for the affordable, high-repetition practice required to develop the skills necessary for free-hand placement of pedicle screws.1
At our institution, the PSPM has been made part of the skills month that is required for all incoming orthopaedic residents. During that month, first-year residents are taught and practice the fundamental skills needed to use 24 orthopaedic instruments that have been identified by our faculty as essential. The tools required for pedicle screw placement are part of this program and each first-year resident learns and practices on their own PSPM under the direct supervision of a fellowship-trained spine surgeon. The instructor teaches the skills along with the proper order of steps for placement of a pedicle screw.
As learners use the model and develop their skills, their progress is measured with a score sheet that focuses on the five tools used for performing four main tasks: 1) opening a hole over the pedicle with a high-speed burr, 2) developing a channel in the pedicle with a pedicle probe and checking its integrity with the ball-tip sound, 3) cutting the threads in the pedicle channel using a tap, and 4) placing the screw with a driver into the threaded channel. Points are awarded for proper handling of surgical tools (such as holding the high-speed burr and pedicle probe with two hands or using the ball-tipped sound to feel the walls of the pedicle) as well as following the proper order of procedural steps. The procedural technique is evaluated and graded for critical steps such as opening the simulated cortical bone in the correct location and maintaining the integrity of the pedicle channel when placing the screw. Trainees are awarded 1 point for novice-level skills, 3 points for advanced-level skills, and 5 points for demonstrating expert-level skills (Appendix 1). An individual participant can score a maximum of 44 points. The time needed to place a screw and the success frequency (correct placement/time) are also calculated and used as markers of skill development. Residents can then track their scores as they progress through residency.
PGY2-5 residents and fellows can return to the skills laboratory prior to and throughout their spine and pediatric rotations to reinforce their pedicle screw insertion skills and become fluent with their use. Residents are then able to confidently take those learned skills to the operating room and focus on the surgical plan and complex operating environment as opposed to trying to learn the skills while simultaneously managing the environment.
Description of Model, Preparation, and Simulation Exercise
The base of the PSPM model is constructed of a common white pine board measuring 76 × 25 × 200 mm. The front and back of the base measure 76 × 200 mm, the top and bottom measure 25 × 200 mm, and the sides of the base measure 25 × 76 mm. Five 19 mm holes, evenly spaced, are drilled from the front to the back of the base. Five angled 7.6 mm holes are drilled from the top of the base into the body of the base, crossing the 19 mm holes. Six-millimeter epoxy tubes, which simulate the cortical walls of the pedicle, are fitted and glued into the 7.6 mm holes. Epoxy tubes, selected because they most closely approximated the haptics of an in situ pedicle, are readily available and inexpensive. The walls of the epoxy tubes are sturdy enough to resist gentle probing but not so sturdy that a poorly directed pedicle finder would not pierce them. The epoxy tubes were placed across the 19 mm hole to simulate the normal pedicle anatomy. The 19 mm hole also allowed for visualization of the final construct resulting in the ability to determine if the pedicle had been breached. The epoxy tubes were filled with 4 mm square balsa sticks to help emulate the structure of the pedicle. To re-create the cancellous “feel” of the pedicle, we found that balsa wood sticks inside of the epoxy tubes give adequate resistance but less than that of the epoxy wall, helping the learner grasp the feel of cannulating a pedicle by hand when the orientation is obscured. After insertion, the epoxy tube and balsa sticks are cut flush with the top of the base. Automotive body filler (Bondo®) is used to cover the top of the base to simulate the posterior vertebral cortical bone. With the epoxy tubes covered with body filler, the high-speed burr can be used to “find” the pedicle.
Several iterations of each component were tried before we arrived at the final model. After both construct and face validation testing, we are confident that this model is reproducible and simulates reality.1
Description of Model Preparation
Creating the model requires the following power tools that are readily acquired: a powered miter saw, a powered oscillating multitool, a portable tabletop saw, and an adjustable-base drill press. These tools are commonly used in our skills laboratory to build all our low-fidelity models. In addition, a 19 mm (3/4 inch) Forstner drill bit, a 7.6 mm twist drill, a 3/4 in. chisel, an awl, and a lightweight ball-peen hammer are needed. The following personal protective equipment is recommended: eye and ear protection, gloves, and a 3M respirator (recommended for use with the automotive body filler).
Using the miter saw, a 76 × 25 mm piece of pine board is cut into 200 mm long pieces. The locations of the five 19 mm holes are marked along the front of the pine board using a premade template. The template is constructed from a thin piece of 76 × 200 mm plywood. Two-millimeter holes that mark the center of each 19 mm hole are placed 15 mm from the top of the block, 25 mm from each side of the block, and 38 mm from center-to-center (Figure 1A). The template is placed over the cut pine board and an awl is used to locate the starting point for each of the 19 mm holes. A drill press with a 19 mm Forstner drill bit is used to create the front-to-back holes in the pine board. A guide is secured to the worktable of the drill press to help simplify the process. Five 19 mm holes are then drilled in each pine board (Figure 1B). The center of each 19 mm hole is marked along the top of the base with a pencil (Figure 1C). A combination square is used to draw a line to mark the lengthwise center line of the top of the base as well.
Figure 1. A. Using a template with pre-drilled appropriately spaced holes allows for faster marking and production of viewing holes. B. Drill press with 19 mm Forstner drill bit is used to create holes along the pine board. C. Completed holes with centers marked.
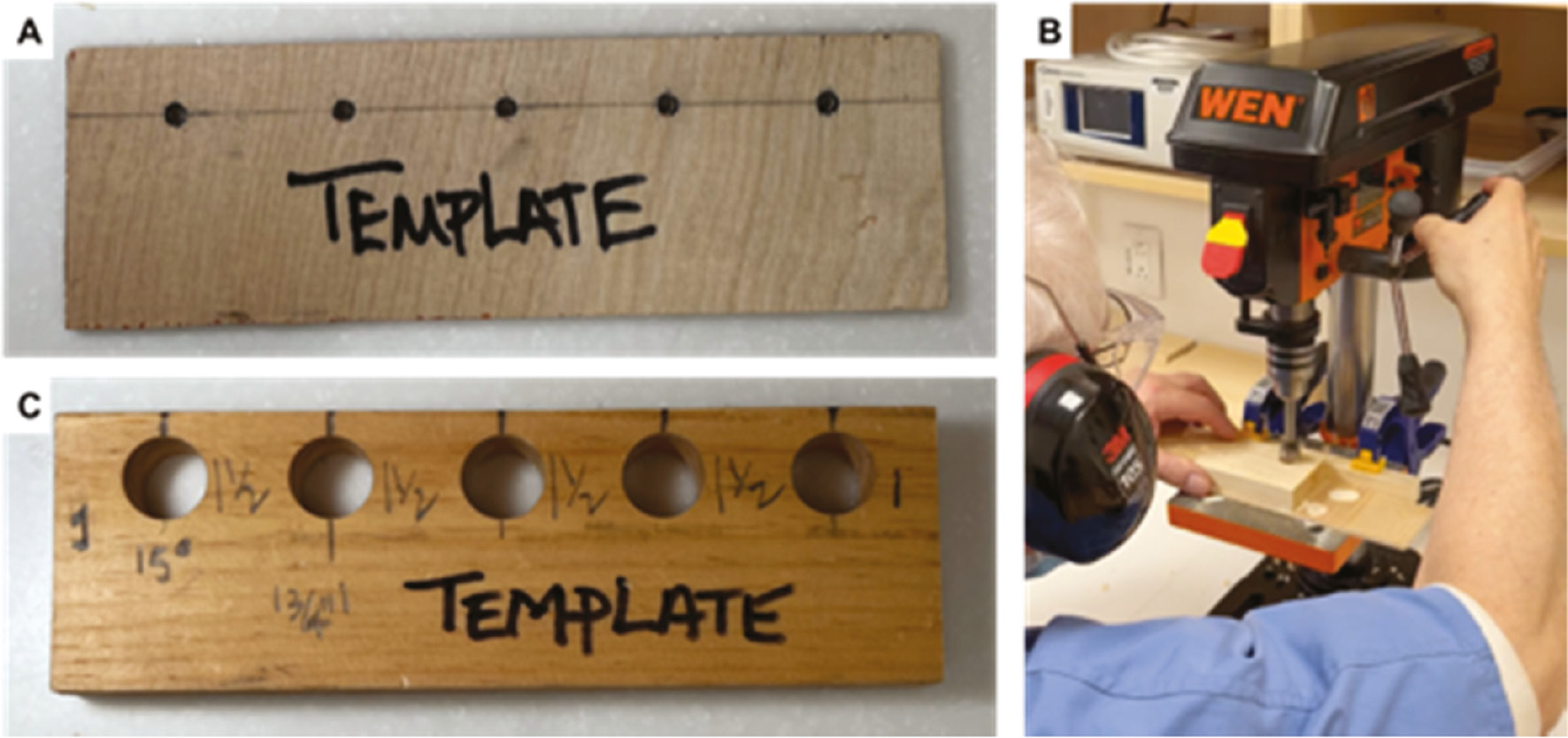
Once all 19 mm holes are created and the block marked, the drill press, with a 7.6 mm twist drill bit, is used to create the holes for the epoxy tubing. The worktable of the drill press is angled to 15 degrees, and the angle is confirmed with a level (Figure 2A). A guide is secured to the worktable of the drill press to ensure the twist drill will always enter the top of the pine board along the pre-marked center. The twist drill bit should enter the top of the 19 mm hole on one side of the hole’s marked center and enter the bottom of the 19 mm hole on the other side of the marked center (Figure 2B). This ensures the angled epoxy pedicle is secured only on its ends (emulating anatomy) and will be visible for most of its length. The angled hole should be drilled to a depth of 45 mm. While the 19 mm and epoxy pedicle holes can be drilled with handheld tools, we found the drill press increases both accuracy and speed for model production on a larger scale. Care should be taken not to attempt to pass the drill bit in one push to avoid binding of the bit. The channel should be smooth and free of debris to allow easy insertion of the epoxy tube.
Figure 2. A. Forstner drill bit is placed in the drill press and the base is adjusted to the appropriate pedicle angle. Set up is confirmed with angled level. B. Hole for pedicles are drilled along the midline of the superior part of the pine board. The drill bit starts on one side of the viewing hole and should exit on the opposite side. The pre-marked viewing hole center allows for easier visualization of drill angle.

The pedicle walls are simulated with a 6 mm wide epoxy tube (wall thickness 1.5 mm) cut into 50 mm long pieces with a portable tabletop saw (Figure 3A). One end of the cut epoxy tube is circumferentially covered with a thin layer of polyurethane adhesive (Gorilla Glue®, The Gorilla Glue Company, Cincinnati, OH), which adds lubrication for easier insertion and fixes the tube in the channel. The tube is gently hammered into the pre-drilled 7.6 mm hole, and when it becomes visible within the 19 mm hole, it can be directed with finger pressure to align it into the distal hole (Figure 3B). Care is taken not to force the tube into the distal hole as too much force or incorrect placement can result in the splintering of the epoxy tube. If splintering occurs, pliers can be used to remove the tube before the glue dries. Roughly 5 mm of the tube will be left proud.
Figure 3. A. Pine board block is secured in a clamp-on bench vise (pictured at bottom). Materials used to insert pedicles include a hammer, Gorilla Glue®, 6 mm wide epoxy tube cut into 50 mm pieces (center), and dowels of 4.8 mm wide balsa wood (right). B. A hammer is used to insert the Gorilla Glue®-coated epoxy tubes into the drilled hole. C. Gorilla Glue® coated balsa wood is placed into each tube and cut. D. Completed pedicle walls and cancellous bone model, the epoxy tubes and balsa wood remain proud and will be cut once Gorilla Glue® is dry.
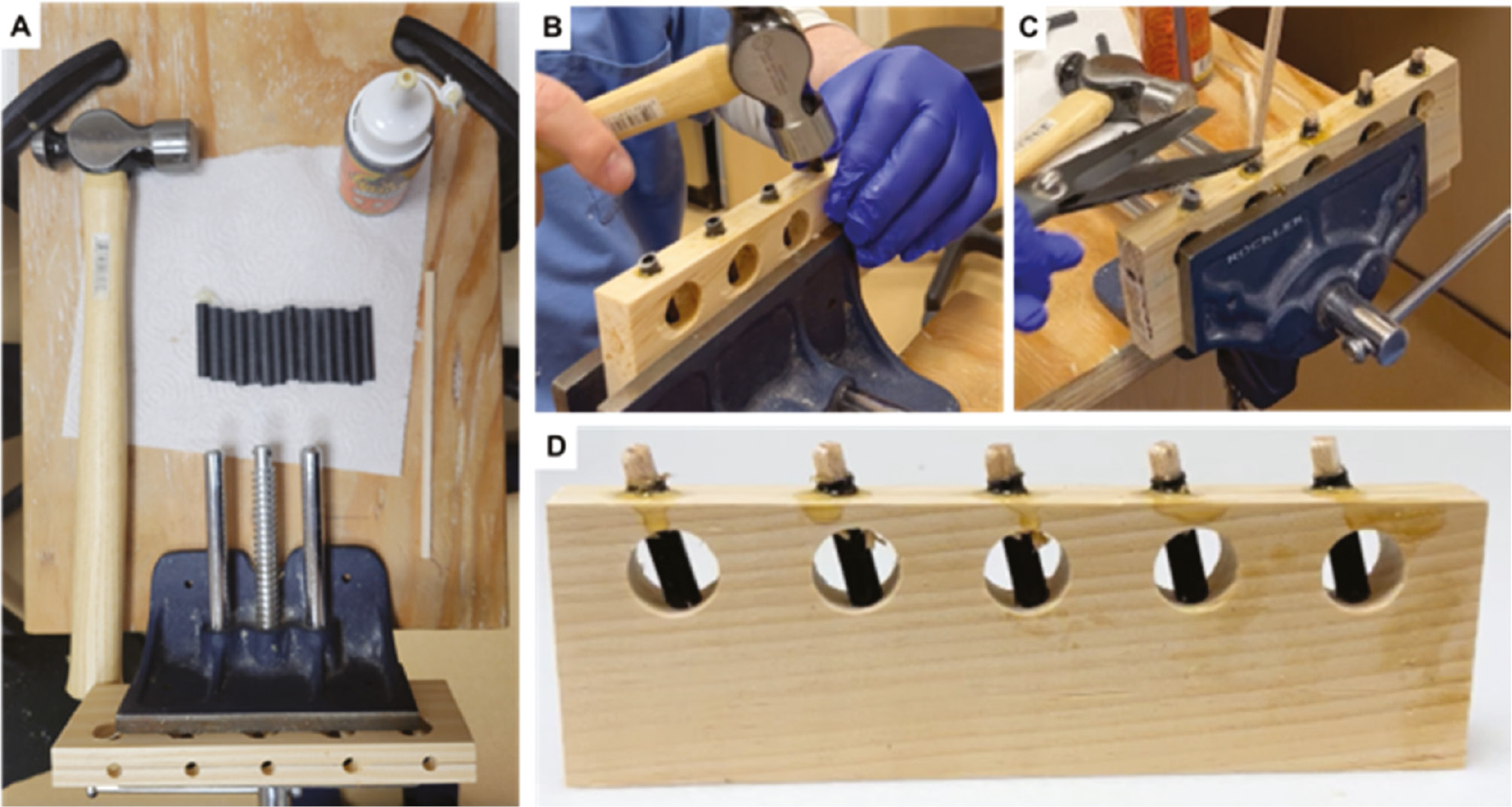
To simulate the cancellous bone within the pedicle, a 4.8 mm square balsa wood stick is inserted into the epoxy tube. A thin layer of glue (Gorilla Glue®) is placed on the tip of a long stick of balsa wood to help glide the stick into the epoxy “pedicle.” The balsa wood does not need to be pre-cut. Instead, the stick can be cut with scissors or a knife after it is inserted into each pedicle (Figure 3C). The model is then left until the glue fully dries—typically 1–2 hrs. (Figure 3D).
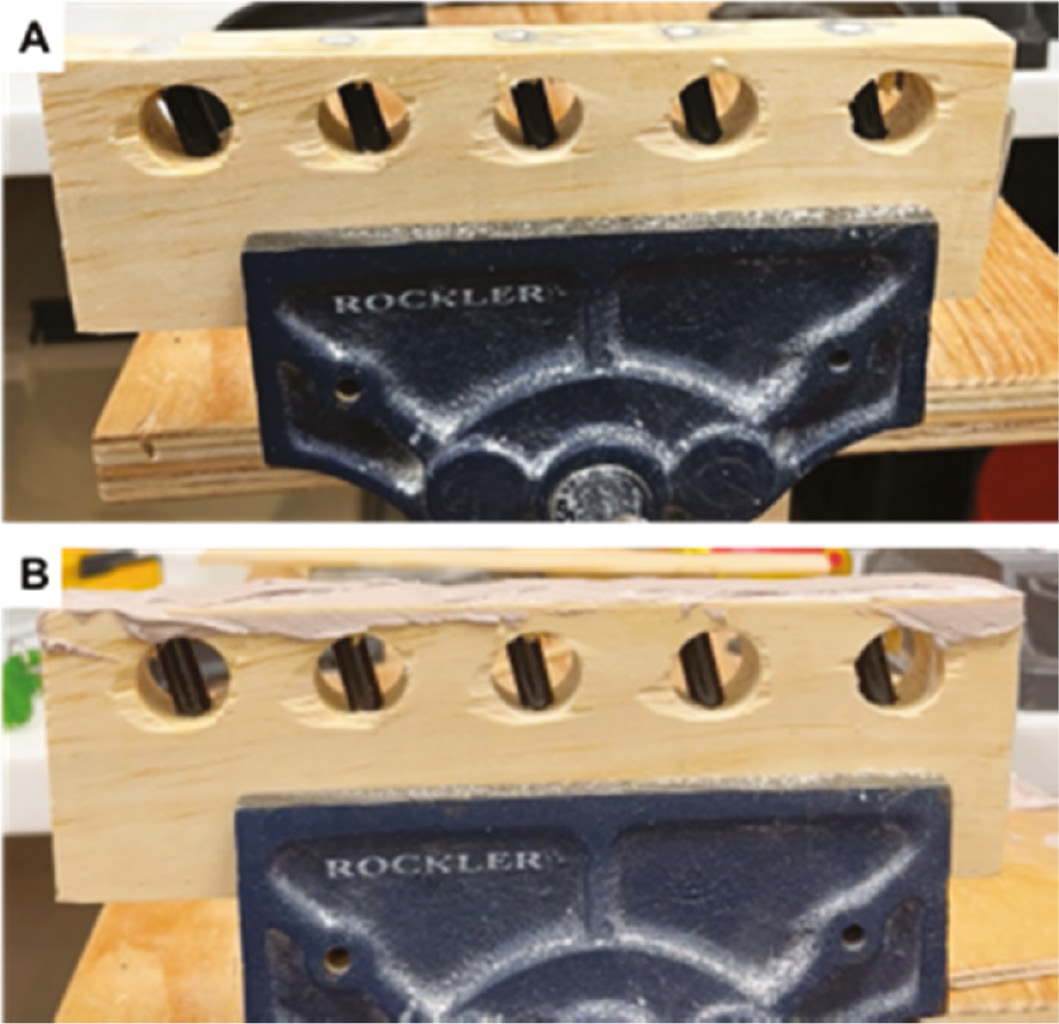
Once the glue dries, an oscillating multitool is used to make a flush cut along the top of the model to remove the proud epoxy tube and balsa wood. A sander can be used to smooth any rough edges (Figure 4A). Automotive body filler (Bondo®, 3M, St. Paul, MN) is then activated with hardener and a smooth, thin coat is layered along the top of the model (Figure 4B). The filler will harden to simulate a hard, cortical spine layer. After it hardens, the excess filler is easily removed with a chisel. The model is allowed to fully dry for a minimum of 24 hrs. prior to use.
Figure 4. A. Excess epoxy tube and balsa wood are cut flush with the top of the model to create a smooth surface. B. Bondo® is placed in a thin layer and allowed to dry. This will simulate hard cortical bone overlying the pedicle.
Minimal changes have been made to the model since its development. Alterations have mainly focused on simpler and faster production of models such as cutting epoxy tube and balsa wood longer than the hole to make insertion easier.
Description of Simulation Exercise
The locations of the pedicles are marked on the side of the model and the 19 mm holes are then covered with tape to prevent direct visualization of pedicle walls. The finished model is secured to the work area with a clamp-on bench vise (Rockler Woodworking and Hardware, Medina, MN). A variable high-speed rotary drill with a 3 mm rotary burr (Dremel), a curved pedicle probe, a flexible ball-tipped sound, a 5.5 mm tap, a pedicle screwdriver, and a 5.5 × 40 mm pedicle screw are placed on the work area next to the model. At the start of the learning session, participants are provided with verbal and visual instructions on how to correctly place their pedicle screw and are told of the 15-degree orientation of the pedicle. The high-speed drill is used to open the starting point of the pedicle through the cortical layer (dried filler). The pedicle probe is used to find the path of the pedicle, and the ball-tipped sound is used throughout the procedure to ensure pedicle walls are not breached. During the training period, participants are encouraged to frequently use the ball-tipped sound to ensure they remain within the pedicle and are properly oriented. Once the pedicle probe reaches the depth of 40 mm, the tap is used to thread the epoxy tube, and the screw can then be inserted. After all five screws are placed, the tape is removed from the base and the pedicle walls are inspected for breaches. The scoring sheet can be filled in and tallied and feedback provided.
The scoring sheet is meant to provide an objective value for a participant’s performance with the understanding that each step may be executed in a variety of ways that are unique to each learner. The final goal is to achieve personal fluency with the tool/skills so that they can be transferred to the OR setting. The time variable should be reserved for more advanced participants, once they have achieved accuracy with the steps so that they can then be judged on their ability to place multiple screws quickly. This combination of accuracy and speed is the hallmark of skill mastery.
Summary
In a time of ever more realistic training models, it may seem anachronistic to advocate for this simple and low-fidelity model. A recent review article on spine simulation training did not even consider the possibility of such a model.4 We believe, however, that the simplicity of this model is its greatest asset. The simplicity allows for high-repetition training with low cost (Appendix 2) and nearly limitless modifications to simulate different surgical situations. The pedicle portion (epoxy tube to mimic pedicle walls and balsa to mimic cancellous bone) can also be combined with more complex, 3D printed models to better simulate the surgical environment. Additionally, the act of producing the model is itself an opportunity for tool learning and practice for the novice or intermediate trainee and can help incorporate diverse levels of learners into the teaching process.
Once the tools and materials are acquired, the model can be quickly produced and easily adapted to simulate different environments. Pedicle angle and length can be varied within the same block, allowing for increased reliance of tactile feel to remain within the pedicle. Varying the diameter of the drills and epoxy tubes can be used to create different pedicle sizes, allowing practice for more challenging pedicles. Deformity cases can also be simulated by varying the angle of the pedicle in multiple planes. To increase the fidelity of the model, the starting point of the pedicle could be overlayed with a drawing or image of thoracic or lumbar posterior elements so that the starting point corresponds to the anatomically correct intersection of the superior articular facet and transverse process.
In the future, we hope to establish a quota or standardized rate of success that can be used to better track resident progress and ability before entering the operating room. With the assistance of both adult and pediatric spine attendings, a standard number of successful pedicle screw placements will be agreed upon after working with the model. This will give residents and fellows a concrete milestone to reach prior to live placement in the operating room.
Disclaimer
A. Morris, L. Alvandi, and I. Levy have no conflicts of interest to report; J. Gomez: financial relationships with Zimmer and Stryker; J. Schulz: financial relationship with OrthoPediatrics.
References
- Mendelis JR, Gomez J, Lo Y, et al. Validity of a novel free-hand pedicle screw placement training tool. J Am Acad Orthop Surg. 2020;28:172–180.
- Kim YJ, Lenke LG. Thoracic pedicle screw placement: Free-hand technique. Neurol India. 2005;53:512-519.
- Gang C, Haibo L, Fancai L, et al. Learning curve of thoracic pedicle screw placement using the free-hand technique in scoliosis: how many screws needed for an apprentice? Eur Spine J. 2012;21:1151-1156.
- Wang Z, Shen J. Simulation training in spine surgery. J Am Acad Orthop Surg. 2022;30:400-408.
Appendices
Appendix 1 – Copy of Scoring Sheet

Appendix 2 – Model Cost Estimate
Table 1: A list of supplies needed to both make a free-hand pedicle screw model and train individuals on it. All model assembly tools and materials can be purchased from a local hardware store. The simulation tools were obtained from the operating room for use in a lab environment. Each price point represents an estimate and can be variable depending on both brand and store. Assembly tools and simulation tools need to be only purchased once for this model, only the low-cost model materials will need to be repurchased to create new models.
| Model Assembly Tools | Price | Quantity | Total Price |
|---|---|---|---|
| Miter Saw | $169.00 | 1 | $169.00 |
| Adjustable-base drill press | $240.00 | 1 | $240.00 |
| Awl | $3.00 | 1 | $3.00 |
| Hammer | $24.98 | 1 | $24.98 |
| Forstner drill bit set | $27.97 | 1 | $27.97 |
| Twist drill bit set | $26.97 | 1 | $26.97 |
| Bench-vise | $27.27 | 2 | $54.54 |
| Clamp | $12.47 | 4 | $49.88 |
| Total cost assembly tools | $596.34 | ||
| Model Materials | Price | Quantity | Total Price |
| Pine board (8 ft) | $6.25 | 4 | $25.00 |
| Epoxy rods | $4.35 | 4 | $17.40 |
| Balsa wood bundle | $7.65 | 4 | $30.60 |
| Bondo® wood filler | $22.00 | 1 | $22.00 |
| Gorilla Glue® | $18.56 | 1 | $18.56 |
| Thin plywood (template) | $6.98 | 1 | $6.98 |
| Total cost model materials | $120.54 | ||
| Simulation Tools | Price | Quantity | Total Price |
| Dremel 4000-6/50 with flexi shaft | $240.00 | 2 | $480.00 |
| Dremel tungsten carbide cutter | $7.24 | 2 | $14.48 |
| Curved Lenke Probes | $100.00 | 2 | $200.00 |
| Flexible ball-tipped sound | $100.00 | 2 | $200.00 |
| 5.5 mm tap | $100.00 | 2 | $200.00 |
| 5.5 × 40 mm pedicle screw | $25 | 10 | $250.00 |
| Total cost simulation tools | $1,344.48 | ||
| Total estimated cost: | $4,122.72 | ||