
JPOSNA® Special Edition
Advances in Pediatric Orthopaedic Education and Technical Training
Surgical Simulation in Pediatric Orthopaedics: An Introduction
Boston Children’s Hospital, Boston, MA
Correspondence: Donald S. Bae, MD, Harvard Medical School, Boston Children’s Hospital, 300 Longwood Ave., Hunnewell 2, Boston, MA 02115. E-mail: [email protected]
Received: May 11, 2022; Accepted: May 22, 2022; Published: August 15, 2022
DOI: 10.55275/JPOSNA-2022-0052
Volume 4, Number S1, August 2022
What is Simulation?
Simulation has been defined by Gallagher, Gallagher, and O’Sullivan as the “the imitation of some real thing, state of affairs, or process.”1 In any simulation—be it a video game, flight simulation, or virtual reality orthopaedic surgery—there are several key elements which are important to recognize (Table 1). First, every simulation seeks to capture the relevant behaviors or tasks inherent to the simulated activity. For a pediatric orthopaedic simulation of scoliosis surgery, for example, replication of pedicle screw placement would be a critically important component. Second, simulations must make simplifying approximations of the task or process. For a pediatric spine simulation, there would likely be approximations of the relationship between the pedicles, lamina, facets, and spinal cord; aberrant anatomy or differences in patient bone quality, for example, would not be easily incorporated into a reproducible simulated task. Third, we understand that simulations will have varying levels of fidelity. Scoliosis simulations, for example, can never truly replicate the exact “feel” or process of instrumenting the human spine. Finally, there should be some measurement of outcome for the learner. Successful placement of a simulated pedicle screw without cortical breakout or violation of the spinal canal, for example, would be key metrics in a scoliosis simulation.
Table 1. Characteristics of Simulations1
| Key Elements of Simulations |
|---|
| Capture relevant behaviors or tasks |
| Simplifying approximations |
| Varying fidelity |
| Measurement of outcome |
While simulations incorporate simplifying approximations of varying fidelity, it is important to recognize that low fidelity simulations can still provide important teaching and learning points for the participant; realism is not directly proportional to learning, and even the simplest simulations can provide meaningful and impactful benefits for the learner. With advancing technology, the field of simulation training is rapidly changing. With a mobile app and computer programming, simulation training has become more individualized, portable, and on-demand. Advanced technologies have also allowed for more immersive user experiences, through augmented or virtual reality platforms. Despite these technological advances, however, all simulations have the same fundamental elements.
Why is Simulation So Important?
Today, simulation has become an integral part of surgical education, both for the resident-in-training as well as the experienced practitioner. Historically, surgical education has followed a mentorship model.2–4 Didactic education and classroom learning were followed by observation and carefully supervised clinical care. The “learn one, see one, do one” approach has been utilized in the United States since its inception in the early 1900s. While generations of surgeons have been successfully trained in this manner, several challenges have promoted changes and improvements in surgical training, particularly through the use of simulation. First, there is an increasing desire to maximize patient outcomes by optimizing technical skills. Simulation training allows for reflective practice to improve performance. Following the dictum of “do no harm,” there is also an increasing desire and expectation to maximize patient safety. The oft-cited 1999 Institute of Medicine report To Err is Human: Building a Safer Health System reported that 44,000 to 98,000 preventable deaths occur in U.S. hospitals every year.5 These data reinforce the importance of avoiding errors to protect our patients. The orthopaedic simulation literature is already replete with examples of how simulation may decrease technical errors and complications.6–10 Finally, the specialty of orthopaedic surgery has seen rapid advances, particularly with minimally or less invasive surgical techniques. Arthroscopic surgery is the prime example of this phenomenon, as we are increasingly seeing arthroscopic-assisted treatment of fractures, ligament and cartilage injuries, growth disturbance, and even congenital differences. Simulation allows for the acquisition and practice of rapidly evolving techniques in a safe and controlled way.
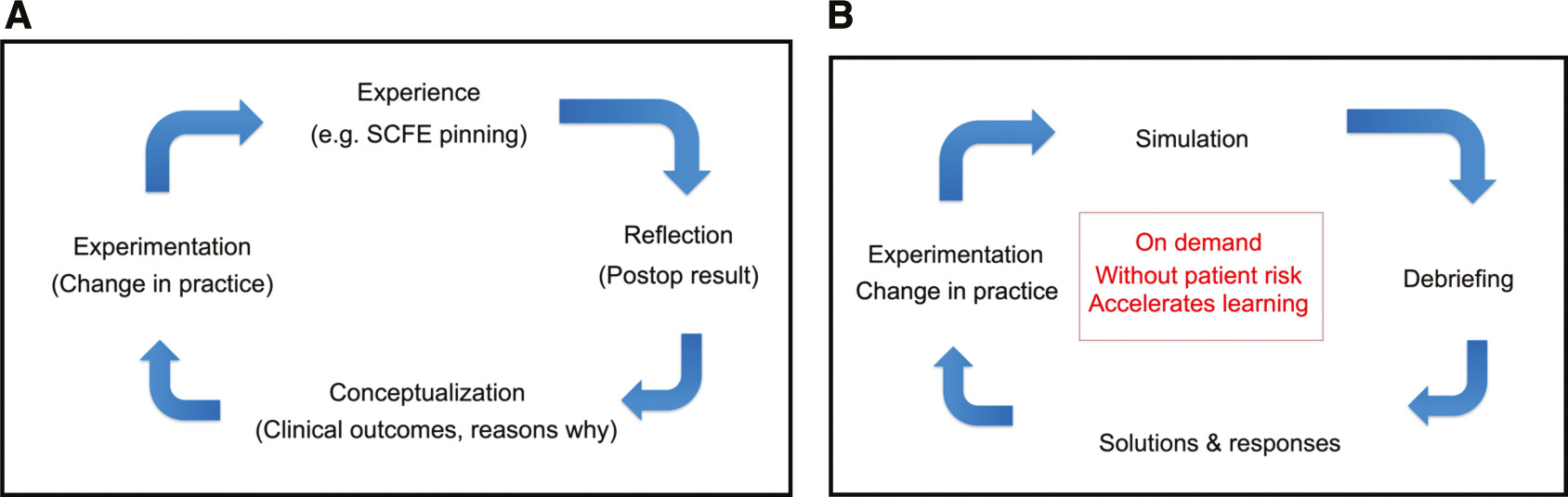
The most compelling reason for simulation training, however, is that simulation is ideally suited for adult learning. We know that adults learn best through independent, problem-based experiences.11–13 Iterative and summative feedback, combined with time for learner reflection, provides the opportunity for analysis and changes/improvements in behavior, which may then be applied to the next experience. Furthermore, this process allows for what is often described as “double-loop feedback.” Rather than simply learning “what” to do, learners have the opportunity to take the next step in understanding “why” they are doing it.14 This process has elegantly encapsulated in Kolb’s learning cycle (Figure 1). Simulation allows for all of the steps of Kolb’s learning cycle—experience, analysis, reflection, and experimentation—in a safe, reproducible, and repeatable way.
Figure 1. (A) Kolb’s Learning Cycle.14 In any experience, such as in-situ pinning of a slipped capital femoral epiphysis (SCFE), adult learners reflect and conceptualize the experience, which then drives experimentation and changes in behavior. (B) In simulation, this cycle is recapitulated through simulated tasks and debriefing.
POSNA Leads the Way
The mission of the Pediatric Orthopaedic Society of North America (POSNA) is “to advance pediatric orthopaedics by promoting education, research, and quality care.” In serving the three pillars of this mission, POSNA has been a leader within orthopaedics in developing, promoting, and implementing simulation training. On the individual level, there are countless society members who have contributed to simulation education, research, and innovation. From curricular development to model creation to research about efficacy, POSNA members have made tremendous contributions. As a society, POSNA has also committed itself to improving the care of children and the excellence of pediatric orthopaedic surgeons through its commitments to simulation training. POSNA was well represented at the original Surgical Simulation Summits of the American Academy of Orthopaedic Surgery in 2011 and 2013. Through its support of the Top Gun surgical simulation program at the annual International Pediatric Orthopaedic Symposium (IPOS®), POSNA has introduced the next generation of pediatric orthopaedic surgeons to the benefits of simulation training. Finally, POSNA has successfully engaged all stakeholders, including our valued industry partners, in developing educational models and curriculae for simulation training, ranging from training models of slipped capital femoral epiphysis to virtual reality modules using immersive audiovisual headsets and haptic feedback (Figure 2).
Figure 2. The spectrum of pediatric orthopaedic surgery simulation. (A) Low fidelity technical skills training using a model of a pediatric distal radius fracture (Photo courtesy of Children’s Orthopaedic Surgery Foundation). (B) Group simulation exercise from the “team challenge” at the IPOS® Top Gun Surgical Skills Competition, focusing on shared technical performance as well as communication and teamwork. (C) Virtual reality simulation performing in-situ pinning of a slipped capital femoral epiphysis using goggles and hand controllers (Photo courtesy of Children’s Orthopaedic Surgery Foundation).

How to Read This Edition
The purpose of this special edition of JPOSNA® is to highlight simulation advances in pediatric orthopaedic education and provide a “blueprint” on how to incorporate simulation training in training programs and established practices. The section on Pediatric Orthopaedic Modules will provide the reader with detailed descriptions of existing exercises for a host of pediatric orthopaedic conditions and procedures. Other articles—including the description of IPOS® Top Gun—will describe innovative societal efforts in simulation. Extending beyond solely technical skills, other articles will describe simulation activities focused on teamwork, communication, and crisis resource management. And finally, in selections on augmented and virtual reality as well as competency-based training, we will get a glimpse into the future of this rapidly changing and exciting field.
Undoubtedly, this special edition will serve as an inspiration and challenge to us all. Perhaps most importantly, after reading this special edition, we will all be inspired to look for opportunities to improve our own practices and programs, begin to measure our clinical results and outcomes, develop our own innovative simulation exercises, and improve our field through continued research and sharing. In this way, we will all learn, improve, and continue to provide outstanding care to our patients and their families.
Acknowledgments
A number of people merit special recognition and acknowledgment. Without them, this special edition would not be possible. Drs. Kenneth Noonan and Elizabeth Hubbard deserve special acknowledgment for their efforts on this special edition of JPOSNA®. Under Dr. Noonan’s leadership, the journal has become the flagship publication for POSNA, and Dr. Hubbard is applauded for organizing an entire edition to the critically important topic of surgical simulation. We are fortunate that our POSNA leadership—the Presidential Line, the Board of Directors, and particularly past presidents Drs. Peter Waters, Jack Flynn, and Michael Vitale—have recognized and supported simulation activities by and for our POSNA members. Through their vision and leadership, we have improved the care of children everywhere and been an “industry leader” within orthopaedics. Special thanks to the many contributors to this edition, who have shared their innovations and simulation expertise so that we may improve our own individual and institutional efforts. Their commitment to innovation, education, and clinical excellence is seen throughout the ensuing pages. And finally, I thank you for your interest in this topic, for your desire to learn and improve, and for the care you provide children and families every day.
Disclaimer
The author has no relevant conflicts of interest to report.
References
- Gallagher AG, O’Sullivan. Simulations for procedural training. In: Gallagher AG, O’Sullivan GC, eds. Fundamentals of Surgical Simulation. London: Springer-Verlag; 2012.
- Cameron JL. William Stewart Halsted: our surgical heritage. Ann Surg. 1997;225:445–458.
- Grillo HC. Edward D. Churchill and the “rectangular” surgical residency. Surgery. 2004;136:947-952.
- Pellegrini CA. Surgical education in the United States: navigating the white waters. Ann Surg. 2006;244:335-342.
- Kohn LT, Corrigan JM, Donaldson MS. To Err Is Human: Building a Safer Health System. Washington, DC: National Academy Press; 2000:196-197.
- Ahlberg G, Enochsson L, Gallagher AG, et al. Proficiency-based virtual reality training significantly reduces the error rate for residents during their first 10 laparoscopic cholecystectomies. Am J Surg. 2007;193:797-804.
- Nagendran M, Gurusamy KS, Aggarwal R, et al. Virtual reality training for surgical trainees in laparoscopic surgery. Cochrane Database Syst Rev. 2013;8:CD006575.
- Pollard TCB, Khan T, Price AJ, et al. Simulated hip arthroscopy skills: learning curves with the lateral and supine patient positions. J Bone Joint Surg Am. 2012;94:e68(1-10).
- Seymour NE, Gallagher AG, Roman SA, et al. Virtual reality training improves operating room performance: results of a randomized, double-blinded study. Ann Surg. 2002;236:458-463.
- Sroka G, Feldman LS, Vassilou MC, et al. Fundamentals of laparoscopic surgery simulator training to proficiency improves laparoscopic performance in the operating room—a randomized controlled trial. Am J Surg. 2010;199:115-120.
- Knowles MS. Andragogy, not pedagogy. Adult Leadership. 1968;16:350-352.
- Ericsson KA, Krampe RT, Tesch-Romer C. The role of deliberate practice in the acquisition of expert performance. Psychol Rev. 1993;100:363-406.
- Schon D. The Reflective Practitioner. How Professionals Think In Action. New York: Basic Books; 1983.
- Kolb. DA, Fry R. Toward an applied theory of experiential learning. In: Cooper C, ed. Theories of Group Process. London: John Wiley; 1975.