
JPOSNA® Special Edition
Advances in Pediatric Orthopaedic Education and Technical Training
Surgical Simulation Curriculum at Boston Children’s Hospital: Improving Skills, Outcomes, and Value
Boston Children’s Hospital, Boston, MA
Correspondence: Donald S. Bae, MD, Harvard Medical School, Boston Children’s Hospital, 300 Longwood Ave., Hunnewell 2, Boston, MA 02115. E-mail: [email protected]
Received: April 19, 2022; Accepted: May 5, 2022; Published: August 15, 2022
DOI: 10.55275/JPOSNA-2022-0053
Volume 4, Number S1, August 2022
Abstract:
Since 2012, the Department of Orthopaedic Surgery at Boston Children’s Hospital (BCH) has implemented a surgical simulation curriculum in pediatric orthopaedics designed to improve trainee education and optimize patient safety and outcomes. The purpose of this review is to briefly describe the current simulation curriculum at Boston Children’s Hospital; provide an example of how these simulation efforts improve safety, outcomes, and value; and discuss recent innovations that are paving the road to future curriculum improvements.
Key Concepts:
- By providing independent, active, problem-based learning with appropriate double-looped feedback, simulation training is ideally suited to adult education.
- Simulation curriculae should be paired with data collection and research to characterize the effectiveness of the simulation training and impact on clinical care.
- Simulation training in distal radius fracture reduction, casting, and cast removal improves patient safety and outcomes in a highly cost-effective fashion.
Introduction
The Department of Orthopaedic Surgery at Boston Children’s Hospital is dedicated to providing the highest quality musculoskeletal care to our patients and improving the health of children everywhere through basic science and clinical research, all while educating the next generation of orthopaedic surgeons. Since 2012, surgical simulation has been a critical component to achieving this three-pronged mission. In close collaboration with the Boston Children’s Hospital Simulator Program, we have developed and implemented a simulation curriculum for surgical trainees who rotate through our department.1 In addition to teaching fundamental skills in pediatric orthopaedics, our simulation curriculum has served as an effective platform to teach pediatric orthopaedic knowledge, improve communication and teamwork, optimize patient safety, and maximize clinical outcomes. Through teaching and research, this simulation curriculum has, in turn, served as a model for other initiatives, including the Top Gun program at the International Pediatric Orthopaedic Symposium (IPOS®) and other societal simulation efforts in New Zealand, Ireland, and beyond.2
The purpose of this review is to briefly describe the current simulation curriculum within the Department of Orthopaedic Surgery at BCH; provide an example of how these simulation efforts improve safety, outcomes, and value; and discuss recent innovations that are paving the road to future curriculum improvements.
Simulation Curriculum
At present, orthopaedic surgical residents participate in simulation training at the onset of their 6-month rotation at BCH. In its current form, this consists of a single afternoon in which the trainees are excused from clinical duties and may devote 4 hours strictly to simulation-based learning. The objectives of this curriculum are to provide core pediatric orthopaedic knowledge, teach safe and effective procedural skills, and deliver iterative and summative feedback for improved technical performance, thus ensuring our trainees have the cognitive and psychomotor knowledge necessary to provide quality care to children. While seemingly focused on specific surgical procedures or individual clinical conditions, our curriculum was intentionally designed to teach residents fundamental, relevant, and transferrable skills (Table 1). These skills include fracture reduction, proper cast application and removal, percutaneous pinning, cannulated screw insertion, and more complex implant placement (e.g., pedicle screw insertion). While not presented in this review, additional modules are available to more advanced learners on arthroscopic knot tying, clubfoot cast application, and periacetabular osteotomy. These simulations were intentionally selected, as they represent fundamental tasks with broader applications that could be effectively taught using impactful but low-fidelity models. Some exercises represent low complexity conditions or procedures performed with high frequency (e.g., short arm cast application) while others address procedures performed less frequently but with potentially greater complexity and risk (e.g., periacetabular osteotomy).
Table 1. Boston Children’s Hospital Simulation Curriculum Exercises
| Specific Simulation Exercise | Universal Application |
|---|---|
| Distal radius fracture reduction, casting, and cast removal | Fracture manipulation, cast application, cast removal |
| Supracondylar humerus fracture reduction and pinning | Percutaneous pinning |
| In situ screw fixation of slipped capital femoral epiphysis | Cannulated screw insertion |
| Thoracic and lumbar pedicle screw insertion | Spine anatomy and instrumentation |
| Arthroscopic knot-tying for labral repair | Arthroscopic triangulation, knot-tying skills |
| Ponseti cast application for clubfoot* | |
| Periacetabular osteotomy for hip dysplasia* |
*Simulations for pediatric orthopaedic fellows
Pre-Simulation Preparation
For each simulation exercise, a learning “toolkit” is provided to the trainees to review prior to the training session. This toolkit consists of background didactic materials (e.g., review articles or primary literature), slides or videos of the planned simulation activity, and a copy of the Objective Structured Assessment of Technical Skill (OSATS). An example of the distal radius fracture toolkit is provided in Table 2 and Appendix 1. It is expected that all learners review the pertinent material and come prepared for the simulation program. Prior to the start of the hands-on activities, the entire group meets for a brief review of didactic material and introduction to the program schedule.
Table 2. The Distal Radius Fracture Reduction, Casting, and Cast Removal “Toolkit”
| Toolkit Category | Specific Items |
|---|---|
| Background readings | Halanski M, Noonan KJ. Cast and splint immobilization: complications. J Am Acad Orthop 2008; 16: 30–40. Halanski MA, Halanski AD, Oza A, Vanderby R, Munoz A, Noonan K. Thermal injury with contemporary cast-application techniques and methods to circumvent morbidity. J Bone Joint Surg Am 2007; 89: 2369-77. |
| Distal radius fracture model | Modified Sawbones distal radius fracture model (SKU 1511-36, Sawbones, Vashon Island, WA)17 |
| Videos | Videos demonstrating technique of cast application and removal |
| Objective structured assessment of technical skill (OSATS) | Modified OSATS, see Appendix 118 |
Simulation Exercise
During the actual simulation exercises, our trainees are divided up into pairs of learners, with four simultaneous activities happening at once. Each pair rotates from station to station during the simulation program, conducting the expected exercise under the watchful eye of a faculty facilitator. In our experience, this program allows for invaluable peer-to-peer learning, as well as real-time iterative feedback from the faculty educator. For critically important learning points, group “pauses” may be taken in which a particular faculty member points out a key learning point to the entire group, irrespective of which station individuals may be situated. Furthermore, our simulation exercises are video-recorded with overhead cameras to allow for subsequent scoring, if necessary, and group debriefing.
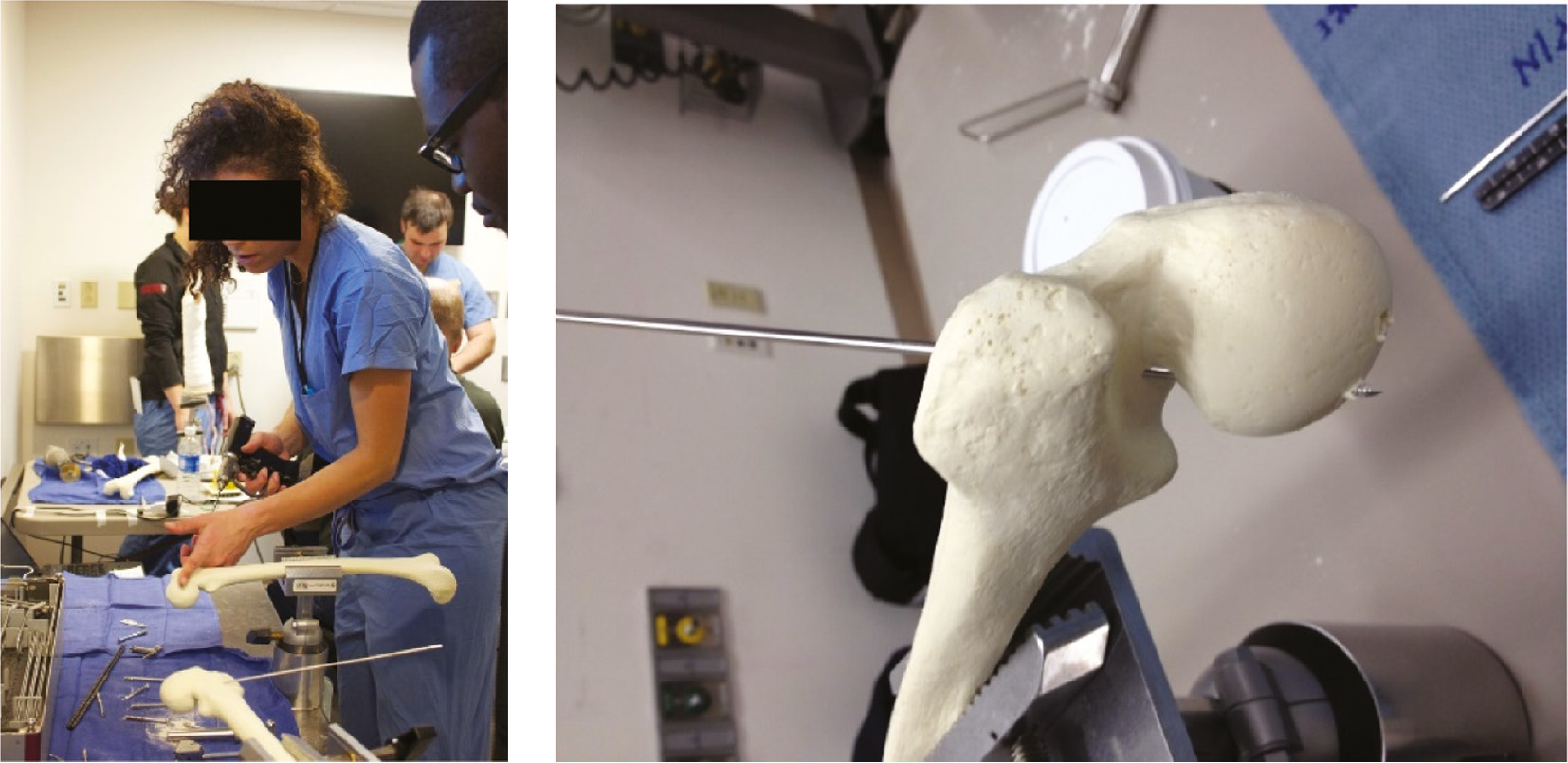
In the distal radius fracture reduction, casting, and cast removal station, learners are asked to reduce an extra-articular distal radius fracture on a commercially available model, apply a well-molded short-arm cast, and then remove the cast using an oscillating cast saw3 (Figure 1). Learners are assessed using a validated OSATS, measurement of the cast index for the cast they applied, and when possible, real-time measurement of peak surface temperatures generated by the cast saw.3–5
Figure 1. Distal radius fracture reduction, casting, and cast removal exercise (Photo courtesy of Children’s Orthopaedic Surgery Foundation).

In the second station, learners perform a simulated reduction of a pediatric supracondylar humerus fracture using a commercially available model (Synbone, PR1110.1, Zizers, Switzerland), followed by “percutaneous” pin fixation using standard operating room equipment (Figure 2). Learners are assessed using our OSATS and have the opportunity to assess their pin constructs and learn about the biomechanics of pin fixation by removing the “skin” from the model and assessing the underlying bone.
Figure 2. Pinning model of pediatric supracondylar humerus fracture (Photo courtesy of Children’s Orthopaedic Surgery Foundation).

The third rotation provides learners the opportunity to perform an in situ cannulated screw placement on a commercially available model of a moderately displaced pediatric slipped capital femoral epiphysis. (Sawbones, SKU 1161, Vashon Island, WA). In addition to the OSATS, learners may assess their screw placement through direct inspection of the model after screw placement, given the absence of fluoroscopic imaging capability (Figure 3).The fourth and final core simulation exercise involves the placement of a thoracic and/or lumbar pedicle screw in a pediatric spine model. To replicate the experience in the operating room on actual patients, the same implants and instruments we utilize in our surgical cases are used in the simulation setting. Assessment is again provided through OSATS and real-time feedback is delivered by the faculty facilitator. Typically speaking, 20 to 30 minutes per station is sufficient time for each of these simulation exercises.
Figure 3. Left: In-situ screw fixation of a pediatric femur with a slipped capital femoral epiphysis. Right: Axial view of the model, demonstrating inadvertent guide pin passage out of the femoral neck. (Photo courtesy of Children’s Orthopaedic Surgery Foundation).
Debriefing
A common adage in the field of simulation training is “Simulation is just an excuse to debrief.” Too often neglected, appropriate debriefing following any simulation activity is critically important to summarize the event(s) and crystallize the take-home learning points. After our trainees complete their rotations through our simulation exercises, we reserve time for group discussion to debrief the day’s events. Emphasis is made to share objective observations—not personal critiques—and provide a psychologically safe setting to discuss the salient technical skills featured in the simulation exercise. While a number of different rubrics for debriefing have been utilized, our current practice is to stimulate meaningful discussion of learning points using the observation-advocacy-inquiry approach.6
Improving Outcomes and Value
While simulation training appeals to the principles and best practices of adult learning, it is critically important that these efforts ultimately improve patient safety and outcomes. Simulation should not be done for simulation’s sake. For this reason, a concerted effort has been made at BCH to pair simulation training with quality improvement or clinical research efforts to quantify the beneficial effects and value-added. To date, the most comprehensive work has been done looking at our distal radius fracture simulation module.
Through prospective evaluation of both simulation performance as well as the clinical results of children treated by our orthopaedic residents for displaced distal radius fractures, we have been able to characterize the impact of our simulation training on patient outcomes. At BCH, we have successfully created and validated a novel distal radius fracture model with embedded thermocouples, which allow for real-time recording of surface temperatures during both cast application and cast saw use.3 Implementation of this cast model within our simulation curriculum has resulted in a decrease in cast saw burns at our institution.7,8 Furthermore, when comparing the cost savings from the avoidance of cast burn complications compared to actual costs of simulation curriculum implementation, we were able to demonstrate a theoretical 11:1 return on investment of our educational efforts. Additional clinical and radiographic analysis determined that our cast simulation curriculum resulted in improved fracture reductions as well as a lower rate of subsequent loss-of-reduction of displaced distal radius fractures.9 Finally, through prospective data collection, we were able to determine the optimal frequency or “dosing” of simulation training, allowing us to optimize our simulation curriculum schedule in the context of limited time and resources.9 While these findings may not be generalizable to all practice settings or academic training programs, they do highlight the importance of concomitant data collection and quality improvement or research protocols to characterize—and optimize—the benefits of any simulation curriculum.
Innovation and Future Directions
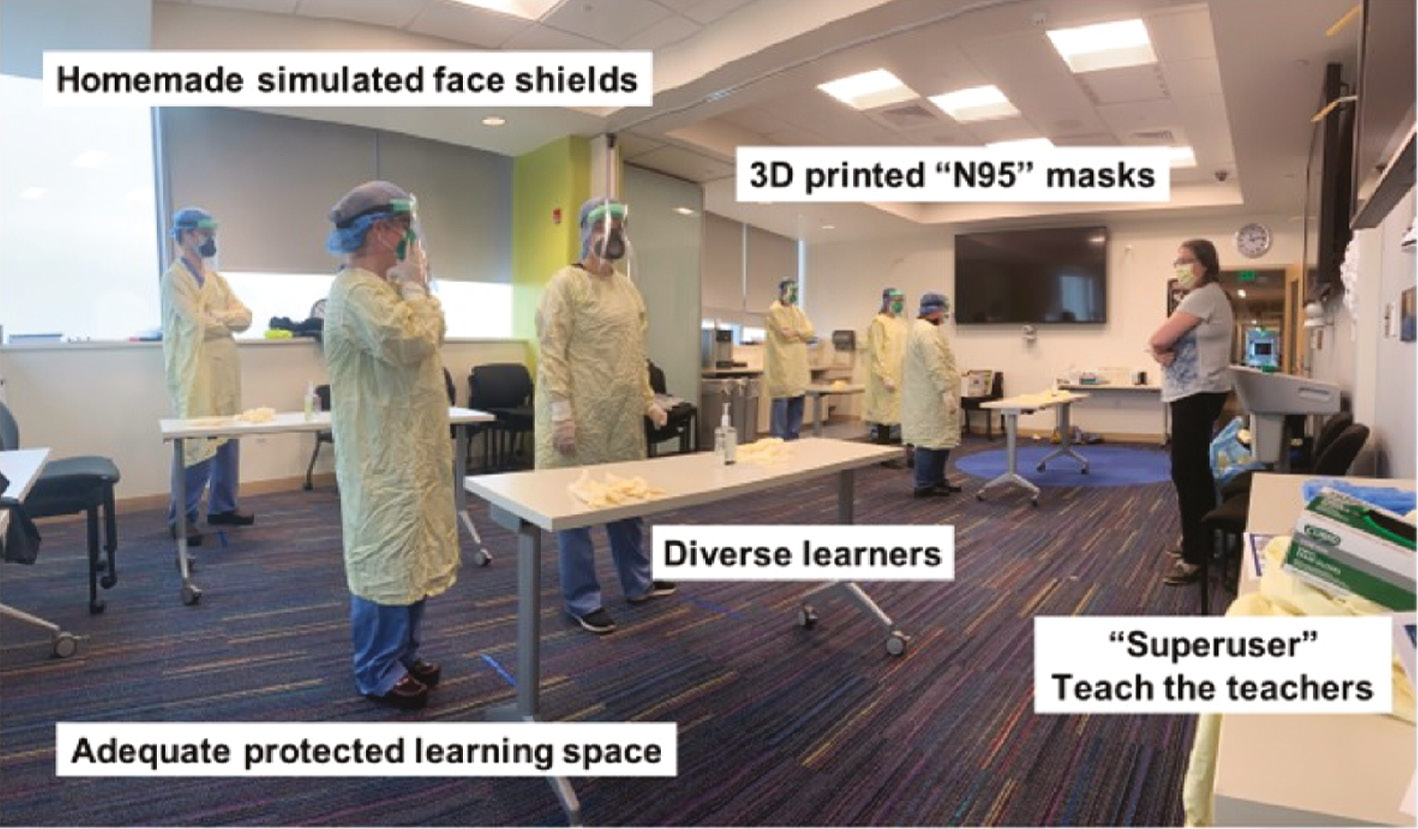
Like all areas of orthopaedic surgery, simulation training is rapidly changing. Adhering to the foundational principles of surgical simulation, a number of recent innovations at BCH continue to grow and evolve. First, while there is continued focus on the acquisition and practice of technical skills, there is recognition of the greater importance, perhaps, of non-technical skills. To this end, we continue to participate in simulation training in teamwork, communication, and crisis resource management.10 Additional details regarding these initiatives can be found in the accompanying article by Dr. Peter Waters in this issue of JPOSNA®. Second, we recognize the opportunities of new technology as well as the new platforms younger learners utilize for their education. At BCH, for example, we have developed a mobile application-based simulation module focusing on the care of pediatric septic arthritis of the hip.11 Similarly, we have contributed to the development of a virtual reality simulation of surgery for slipped capital femoral epiphysis, in conjunction with the Pediatric Orthopaedic Society of North America and an industry partner Osso VR. Finally, we have improved our abilities to utilize simulation training to address critical acute needs. At the outset of the COVID-19 pandemic, for example, our institution faced challenges in teaching our frontline orthopaedic care providers the proper technique to don and doff personal protective equipment (PPE). We were able to develop and implement a surgical simulation on the donning and doffing of PPE within 7 days, eventually cycling over 70 orthopaedic practitioners through our simulation center in the first few weeks, using 3D printed models of respirator masks (Figure 4).
Figure 4. Simulation training in proper donning and doffing technique of PPE during the early COVID-19 pandemic (Photo courtesy of Children’s Orthopaedic Surgery Foundation).
While these innovations are exciting, the foundational principles of our simulation program remain steadfast. Using simulation training, we strive to provide the highest quality education for our orthopaedic trainees and to optimize procedural safety, clinical outcomes, and healthcare value for our patients and their families.
Disclaimer
The author has no relevant conflicts of interest to report.
References
- Bae DS, Waters PM. Pediatric orthopedic surgical simulation at Boston Children’s Hospital. J Pediatr Orthop B. 2016;25:292–295.
- Flynn JM. IPOS Sponsors Surgical Simulation Competition. AAOS Now, March 2013. Available at: https://www.aaos.org/aaosnow/2013/mar/youraaos/youraaos9/.
- Brubacher JW, Karg J, Weinstock P, et al. A novel cast removal training simulation to improve patient safety. J Surg Educ. 2016;73:7-11.
- Moktar J, Popkin CA, Howard A, et al. Development of a cast application simulator and evaluation of objective measures of performance. J Bone Joint Surg Am. 2014;96:e76.
- Bae DS. Pediatric distal radius and forearm fractures. J Hand Surg Am. 2008;33:1911-1923.
- Rudolph JW, Simon R, Rivard P, et al. Debriefing with good judgment: combining rigorous feedback with genuine inquiry. Anesthesiol Clin. 2007;25:361-376.
- Shore BJ, Hutchinson S, Harris M, et al. Epidemiology and prevention of cast saw injuries: results of a quality improvement program at a single institution. J Bone Joint Surg Am. 2014;96(4):e31.
- Bae DS, Lynch H, Jamieson K, et al. Improved safety and cost savings from reductions in cast-saw burns after simulation-based education for orthopaedic surgery residents. J Bone Joint Surg Am. 2017;99(17):e94.
- Rabinovich RV, Shore BJ, Glotzbecker M, et al. The effect of casting simulation on maintenance of fracture alignment following closed reduction of pediatric distal radius fractures: does more simulation matter? J Surg Educ. 2021;78(5):1717-1724.
- Arriaga AF, Gawande AA, Raemer DB, et al. Harvard Surgical Safety Collaborative. Pilot testing of a model for insurer-driven, large-scale multicenter simulation training for operating room teams. Ann Surg. 2014;259:403-410.
- Shore BJ, Miller PE, Noonan KJ, et al. Predictability of clinical knowledge through mobile app-based simulation for the treatment of pediatric septic arthritis: a pilot study. J Pediatr Orthop. 2018;38(9):e541-e545.
Appendix 1. OSATS for Application & Removal of Short-Arm Cast for Distal Radius Fracture
Instructions to Candidates:
The patient has fractured their distal radius. Apply a short arm circumferential cast to maintain the reduced fracture
| ITEM | Not done/Incorrect | Done/Correct |
|---|---|---|
| I. Stockinette | ||
| 1. A small snip is made in the stockinette for the thumb | 0 | 1 |
| 2. The stockinette is smoothed out, leaving no wrinkles or creases | 0 | 1 |
| II. Webril application | ||
| 1. Appropriate soft roll width is selected (2–4 inches for forearm) | 0 | 1 |
| 2. Soft roll is applied using moderate tension | 0 | 1 |
| 3. Soft roll is wrapped such that each layer overlaps the previous layer by 50% | 0 | 1 |
| 4. Thicker soft roll layers are applied over the palm and proximal base of cast | 0 | 1 |
| 5. Soft roll coverage extends from the antecubital fossa to past the MCPJs | 0 | 1 |
| III. Fiberglass application | ||
| 1. Appropriate fiberglass roll width is selected (2–4 inches for forearm) | 0 | 1 |
| 2. The fiberglass is soaked in tepid water with the free end slightly unrolled | 0 | 1 |
| 3. The first fiberglass layer extends from 2–3 cm distal to the antecubital fossa to the proximal palmar crease | 0 | 1 |
| 4. Thumb should remain exposed at metacarpophalangeal joint | 0 | 1 |
| 5. Fiberglass is applied to leave a distal and proximal border or “cuff” of soft roll and stockinette | 0 | 1 |
| 6. The stockinette and soft roll cuffs are folded over the first layers of plaster | 0 | 1 |
| 7. A second fiberglass layer is applied to cover the folded cuffs to leave a smooth border | 0 | 1 |
| IV. Molding | ||
| 1. Thenar eminences of palm are used to apply pressure until mold is firm | 0 | 1 |
| 2. Mold is applied firmly but retains natural contours of the arm | 0 | 1 |
| 3. For dorsally angulated fractures: 3 point fixation applies dorsal pressure proximal and distal to the fracture, and volar pressure over the reduced fracture | 0 | 1 |
| V. Cast removal | ||
| 1. Saw blade is checked for sharpness and security | 0 | 1 |
| 2. A zip-stick is placed beneath cast if available | 0 | 1 |
| 3. The hand is braced against cast during saw use | 0 | 1 |
| 4. An in-and-out motion is used during saw use | 0 | 1 |
| 5. The saw blade is intermittently cooled during use | 0 | 1 |
| 6. Cast spreaders are used properly | 0 | 1 |
| 7. The cast is gentle removed with appropriate use of bandage scissors to protect underlying skin | 0 | 1 |
| 8. The cast is removed without any marks/burns on the skin | 0 | 1 |
| Total score (Maximum 25) | ||
Adapted from Moktar, J and Murnaghan ML. Casting Simulation in Orthopaedics: Improving a Lost Art. 2012