
JPOSNA® Special Edition
Advances in Pediatric Orthopaedic Education and Technical Training
Tablet-Based Fluoroscopy Simulator for Supracondylar Humeral Fracture Pinning
1University of Otago, New Zealand; 2Starship Hospital, Auckland, New Zealand
Correspondence: Phil Blyth, BHB, MBChB, PhD, 290 Great King St., Dunedin, Otago, New Zealand. E-mail: [email protected]
Received: April 13, 2022; Accepted: May 22, 2022; Published: August 15, 2022
DOI: 10.55275/JPOSNA-2022-0067
Volume 4, Number S1, August 2022
Introduction
The reduction and surgical fixation of a pediatric supracondylar humeral fracture can be a difficult procedure. It is a common emergency operation that can be technically difficult due to swelling, small bones, and co-existing vascular and neurologic trauma. The procedure relies heavily on fluoroscopic confirmation of fracture reduction and pin position. This makes the development of expertise difficult as the repetitive practice required exposes the participant to ionising radiation.1 The ideal surgical simulation would reproduce the clinical scenario as closely as possible. We, therefore, have created a model where the bone structure and soft tissues mimic as closely as possible what we experience in the clinical setting. Objective assessments of particular tasks such as this are prone to issues with intra- and inter-rater reliability. The metrics available within this model may offer a means to determine skill progress within a trainee and comparison between trainees.
Although non-fluoroscopic supracondylar pinning practice has been in place within our training programme for years, the introduction of this tablet-based approach was first introduced at the annual Australian/New Zealand Paediatric Orthopaedic Society meeting in 2017. It is now being incorporated into hospital training and as a skill station within the advanced training programme of our residents.
Description of Simulator
Our group has developed an artificial elbow model. This was created after testing four sets of artificial bones with eight advanced residents and four consultants. Repetitive testing and evaluation were subjectively measured so a model was created that mimics a pediatric humerus as closely as possible (Figure 1). The bones are 3D printed using a standard fused depositional modeling printer (Flashforge Creator Pro 2, Zhejiang Flashforge 3D Technology Co., Jinhua City, China) using standard Acrylonitrile Butadiene Styrene (ABS) plastic. Although tolerant to several K-wire passes, the experience is diminished after multiple passes and thus the inexpensive humerus bone can be replaced as required.
Figure 1. Part of the silicone casting process showing forearm bones and humerus which will be incorporated within the soft tissue.

Similarly, different tissue hardness’s were incorporated within three soft tissue models to reproduce the swelling and turgor of the tissues that are usually associated with this fracture. These models were tested in a similar blinded way. The result is a simulation model that is as close to reality as we can manufacture (Figure 2). The soft tissue elements are constructed with a number of materials. Muscle, skin, and subcutaneous tissues of the elbow are produced using multiple 3D printed silicone casts. Silicones of different shore hardness’s are used to match the oedematous tissue. The silicone has withstood upwards of 100 penetrations with little deterioration. The forearm and hand are fabricated using thermoplastic polyurethane (TPU) plastic.
Figure 2. The combined upper limb model, including removable bones, muscle, soft tissue, and distal forearm and hand.

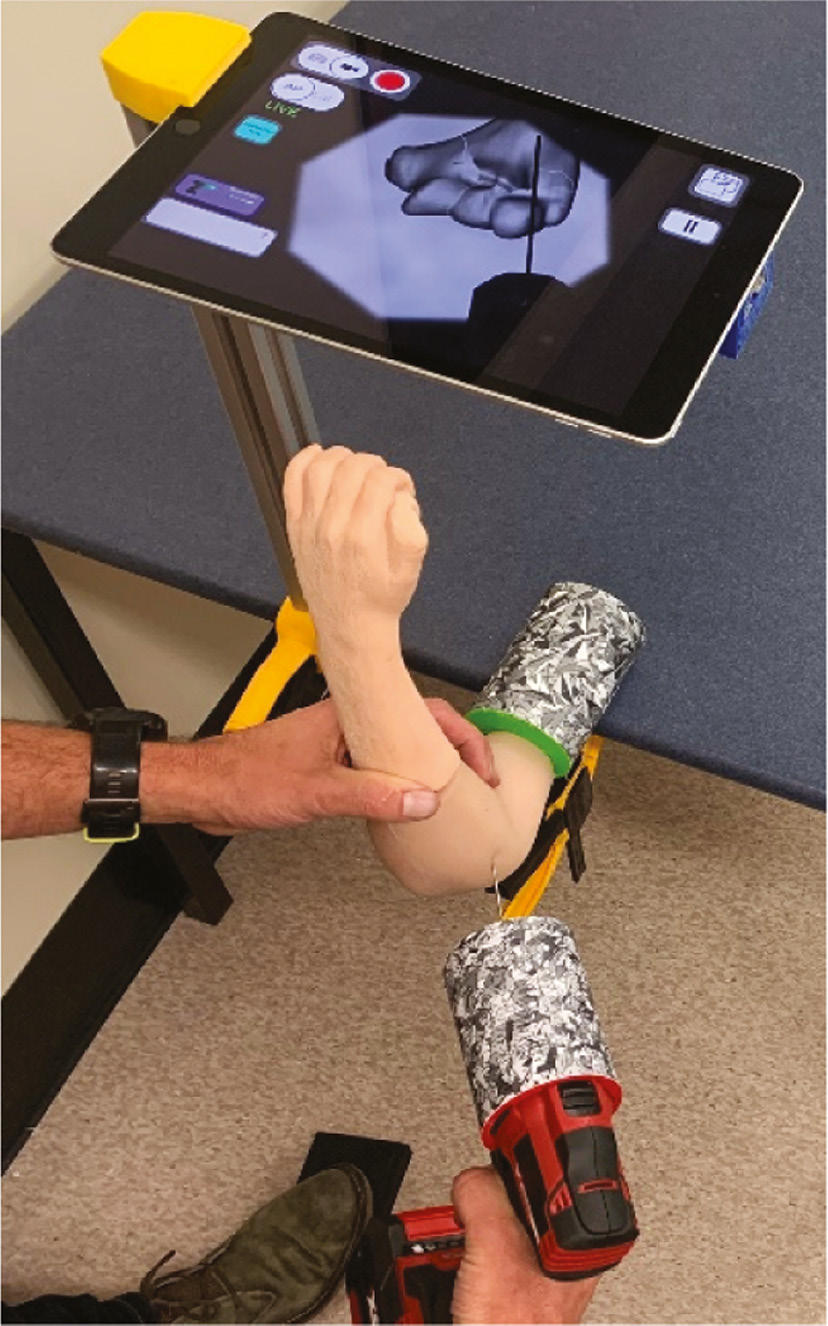
To eliminate ionising radiation, the Bonedoc AR simulator was developed. This mixed reality iPad app provides real-time simulated fluoroscopy images. Using optical tracking technology combined with fiducial markers (reference points) placed on the upper limb model and the drill, the location and poise of these physical components are calculated, and a simulated fluoroscopic image is produced (Figure 3).
Figure 3. View of the simulator with upper limb, drill, K-wire, foot pedal, and “fluoroscopy.”
The morphology of the bones was based on CT images of an anonymous normal pediatric elbow. These were downloaded from an open-source website (embodi3D, Bellevue, WA - https://www.embodi3d.com). Using the open-source imaging software from Slicer (Slicer - https://slicer.org), surface segmentation of bone and soft tissue elements were undertaken. These 3D datasets were imported into the open-source modeling software Blender (Blender, Amsterdam, the Netherlands - https://blender.org). Using sculpting tools within this software, the skin and subcutaneous tissue was adapted to produce a moderately swollen elbow; similarly, muscle, bone, and cartilage structures were created. The models were purposely created to allow the exchange of the bones as required.
The Bonedoc AR app has been developed using the Unity cross-platform gaming engine (Unity Technologies, San Francisco, CA - https://unity.com). Using mixed reality techniques and the camera within the iPad, based on optical tracking of fiducial markers (reference points), the exact location and poise of the bone and drill are identified. Subsequently, fluoroscopic images are created, and the position and trajectories of all passes of the wire are recorded (see video #1 – Demonstration of Real-time Continuous Fluoroscopic Imaging). The location of the ulnar nerve is tracked, and any K-wire penetration is recorded.
The other hardware includes fiducial markers which are custom-produced plastic to match the drill and the upper-limb holder and 3D printed with Acrylonitrile Butadiene Styrene (ABS) plastic. A standard cordless drill and a standard K-wire are used. A 10.2ʺ iPad with a custom-built stand is easily capable of running the Bonedoc AR app, and a custom-made Bluetooth pedal is used to obtain hands-free fluoroscopic images.
Description of Simulation Exercise
The exercise involves the pinning of a 7-year-old with a Gartland Type 2 supracondylar humeral fracture. It is assumed a satisfactory closed reduction of the fracture has been achieved. The resident is tasked to place two laterally based diverging percutaneous pins under fluoroscopy guidance. The location of these pins is as described by Kocher et al.2 The simulation can be undertaken by a sole operator, with one hand to maintain the position of the forearm appropriately and the other to drill the K-wire. Fluoroscopic images are obtained using the foot pedal. The fluoroscopy can produce lateral and AP images in real-time, and both continuous and single-shot imaging is possible.
Images are stored as obtained, allowing the trainee (and or supervisor) to reflect on the procedure. The app logs the location and poise of the wires in real-time, such that misplaced K-wires are recorded regardless of whether an x-ray was acquired. Scores and logs are stored on the iPad and can be uploaded to a server. All components fit in a small aluminium case. The time for setup is around 1 minute (see video #2 – Demonstration of Setup and Procedure Performed by Resident).
Metrics Acquired
Surgical Time
Note, this does not include reduction time, as this part of the procedure is assumed to be complete. Further split into time taken for each of the wires.
Fluoroscopy Time
Includes an adjustment for the time normally needed to switch between AP and lateral views.
Radiation
The amount of radiation used both from single and continuous shots. This has been shown to reduce with more experience.3
Pin Accuracy
The exact pin placements measured to the millimetre; this includes accuracy of entry point, location at the fracture site, and cortical exit point. Due to the logistical cost of evaluating the position of K-wires on fluoroscopic images, an objective score for the position of K-wires is difficult in real life. In contrast, within the app, the exact location and poise of the K-wire is tracked in real-time and scores for pin placement.
Errors
The number of misplaced K-wires as well as the amount of excursion (measured in millimeters). Iatrogenic injury to the ulnar nerve is included.
Total Score
An arbitrary percentage score is calculated based on a weighted calculation combining the above variables. The pin accuracy is weighted higher than other variables.
Summary
This simulation model has the advantage of reproducing the clinical scenario as closely as possible. It allows the participant multiple attempts without the risk of ionising radiation. It can be used for both education and as an assessment tool for residents. It has taken a number of years to refine the technology to make the simulator user-friendly, portable, reproducible, and able to be used without an instructor. By keeping the setup simple, the task is focused on the skill, not using the simulator. It has been important to reproduce the texture of the bone and soft tissue as close as possible to real life so the feedback from the simulation is authentic.
Future Directions
Incorporating fracture reduction within the model would be advantageous; however, the limits of optical tracking make this difficult. While electromagnetic tracking would facilitate this, the drill’s electric motor impacts significantly on this approach. The fiducial markers are multi-purpose, allowing the simulation of similar fluoroscopy-guided procedures of other joints, especially the wrist, hand, foot, and ankle. This would allow for other “fluoroscopic” simulations to adopt this non-ionising radiation technique.
Transfer validity of the simulator is currently being undertaken.4
Disclaimer
P. Blyth: Developer of Bonedoc AR; H. Crawford: No conflicts of interest to report.
References
- Ericsson KA, Krampe RT, Tesch-Römer C. The role of deliberate practice in the acquisition of expert performance. Psychol Rev. 1993;100(3):363–406.
- Kocher M, Kasser J, Waters P, et al. Lateral entry compared with medial and lateral entry pin fixation for completely displaced supracondylar humeral fractures in children. J Bone Joint Surg. 2007;89(4):706-712.
- Kalenderer O, Turgut A, Bilgin E, et al. The influence of resident level of training on fluoroscopy time in pediatric supracondylar humeral fractures treated with closed reduction and percutaneous pinning. Cureus. 2018;10(2):e2245.
- Guo J, Clifford K, Hooper NM, et al. Transfer validity of paediatric supracondylar humeral fracture pin placement practice on in-theatre performance by orthopaedic trainees using an augmented reality simulator: protocol for a non-randomized intervention cohort with retrospective comparator pilot study. JMIR Res Protoc (submitted). http://doi.org/10.2196/preprints.38282
Appendices
Appendix A. Score Sheet
| Competency | Observer Assessment | Bonedoc AR Assessment |
|---|---|---|
| Correct elbow position during pinning | Flexion maintained (True/False) | (Planned) |
| Appropriate assessment of pulse | Pulse taken/mentioned (True/False) | (Planned) |
| Assesses/avoids risk of ulnar nerve damage | Demonstration/mention of risk of ulnar nerve damage if medial approach proposed (True/False) |
Penetration of K-wire to ulnar nerve measured |
| Places pin accurately | Acceptable position (True/False) | Percentage score, calculated with reference to perfect measurement (mm):
|
| Acceptable number of misplaced K-wire passes | Within acceptable range (True/False) | Percentage score, calculated with reference to
|
| Radiation | Not excessive, assumes fluoroscopy available (True/False) | Percentage score, calculated with reference to
|
Time
|
Within allocated time (True/False) | Percentage score, calculated with reference to:
|
Appendix B. Approximate Cost
| Item | Approximate Cost (US$) |
|---|---|
| Single Purchase Items | |
| Bonedoc AR app | Yet to be finalized |
| Simulation Rig (Includes iPad, Cordless Drill, iPad Case, iPad Support, Aluminium Case, Bone Clamp and Fiducial, Bluetooth Foot Pedal, Drill Fiducial, Forearm (Includes Radius/Ulna) |
$1300 |
| Consumables | |
| Soft Tissue Elbow Model Multi-use, expect ~ 30–50 usages |
$100 |
| K-wires Multi-use, expect ~ 5–10 usages |
$60 per 10 pack |
| Distal Humerus Bone Single-use (Can be multiple-use, depending on the number of passes of wires) |
$5 |