
JPOSNA® Special Edition
Advances in Pediatric Orthopaedic Education and Technical Training
Acquiring the Skills to Perform Point of Care Ultrasound of the Infant Hip Through Simulation
1NYU Langone Health, New York, NY; 2Ortopedia y Traumatología, Centro Médico ABC, Mexico City, MX
Correspondence: Christina Herrero, MD, 301 East 17th St., New York, NY 10003. E-mail: [email protected]
Received: March 23, 2022; Accepted: April 6, 2022; Published: August 15, 2022
DOI: 10.55275/JPOSNA-2022-0065
Volume 4, Number S1, August 2022
Introduction
Developmental dysplasia of the hip (DDH) is the most common anatomical pathology in newborns. The reported incidence ranges from 4.4% to 51.8%, depending on risk factors, populations, and reporting methods.1 Traditionally, the standard physical exam for newborns includes hip stability testing using the Barlow and Ortolani maneuvers. If the pediatrician detects hip instability, the baby is typically referred to a pediatric orthopaedic surgeon. Also, either the pediatrician or pediatric orthopaedic surgeon obtains a hip ultrasound—the gold standard for DDH diagnosis.
Ultrasound (US), though most well-known for diagnostic purposes, is also instrumental in treating and monitoring DDH. Compared to standard radiographs, US allows dynamic evaluation to determine the presence of instability in addition to the dysplasia. It dramatically improves the sensitivity for hip dislocation diagnosis, with one study finding that the sensitivity of ultrasound screening was 88.5% compared with clinical screening, which had a sensitivity of 76.4%.2 Roovers et al. also found that a much higher proportion of patients in the ultrasound screening group were referred before the age of 13 weeks compared to those referred from the clinical screening group.2 US also has a much higher sensitivity rate (89%) when compared to radiographs (66%) for the diagnosis of hip dysplasia in children under 4 months old.3 US is also used to monitor acetabular development and appearance of the ossific nucleus of the femoral head, and these measures can help guide the type and duration of treatment. US is also a valuable tool for the intraoperative evaluation of closed reduction.4
Ultrasound equipment and technology have evolved in parallel to maintaining imaging quality, allowing physicians to take the tool to the point of care and incorporate it into the clinical evaluation and workup of patients.5 US has decreased time delays on urgent matters throughout musculoskeletal medicine and decreased costs for both physicians and patients.6 However, learning the technique of infant hip ultrasound can be difficult. It may impede incorporating this into clinical practice. The lack of exposure and paucity of patients makes learning the technique unreliable. The nature of pediatric orthopaedic practices means that for many residents on a rotation, there may not be many newborns brought in for ultrasound examination of the hip.
We present our experience with a simulation model for teaching point-of-care ultrasound examination of an infant hip. The senior author of this paper developed a program in Mexico City dedicated to teaching physicians how to perform ultrasound-enhanced physical examination of the infant’s hip and started this specific course in 2007. We incorporated the training simulation into practice due to a lack of exposure to patients and the difficulty of getting enough repetitions with actual patients. In January 2021, this method, along with the incorporation of the phantom baby and simulation training, was expanded to include the residency program. The method taught in this program now includes the current postgraduate orthopaedic surgery residency training program where all third-year residents rotate through the simulation training and practice weekly over 4 months as part of the curriculum. We have successfully deployed this training method, during which learners apply the method and ultimately screen children and evaluate in follow-up. The training program in Mexico City entails the residents practicing weekly and graduating to using US on infants in clinic. We are not currently testing proficiency with our teaching techniques. The focused 2-day course has been successful, training over 150 physicians in 8 years. This remains as a stand-alone course run by the AMDUC (Asociacion Mexicana de Displasia y Ultrasonido de Cadera). Information can be found at http://www.amduc.com.mx/.
Description of Simulation Exercise: Ultrasound Examination of Infant
US of the newborn should be performed in a relatively dark, quiet room with adjustable lights and minimal interruption. At our institution, there is a patient exam room specifically reserved for training users in this technique. One should have a warm blanket to ensure the infant is comfortable and that the ultrasound gel is warm. Any ultrasound device can be used as long as it obtains high-definition images and uses a linear 5–7.5 Mhz transducer.
For simulation training, the Graf method has proven reliability. It is easily reproducible using a low-fidelity “phantom baby,” which is a simulation model that is commercially available and is helpful for the acquisition of the skill of understanding transducer placement and anatomic definition.
The method described by Graf is beneficial in learning to ensure consistency and accuracy and uses a standardized checklist and measurements, which allow learners to develop the pattern recognition skills necessary to acquire the ability to identify morphology on sonographic imaging.
- The Graf Checklist consists of identifying seven anatomical structures (Figure 1) in addition to two reference landmarks:
- The osteochondral border
- The femoral head
- The synovial fold
- The capsule
- The labrum
- The cartilaginous roof
- The bony roof
Two reference landmarks:
- The lower limb (Os ilium)
- The turning point (the exact point where the concavity of the acetabulum turns into a convexity and where the beta angle should be drawn)
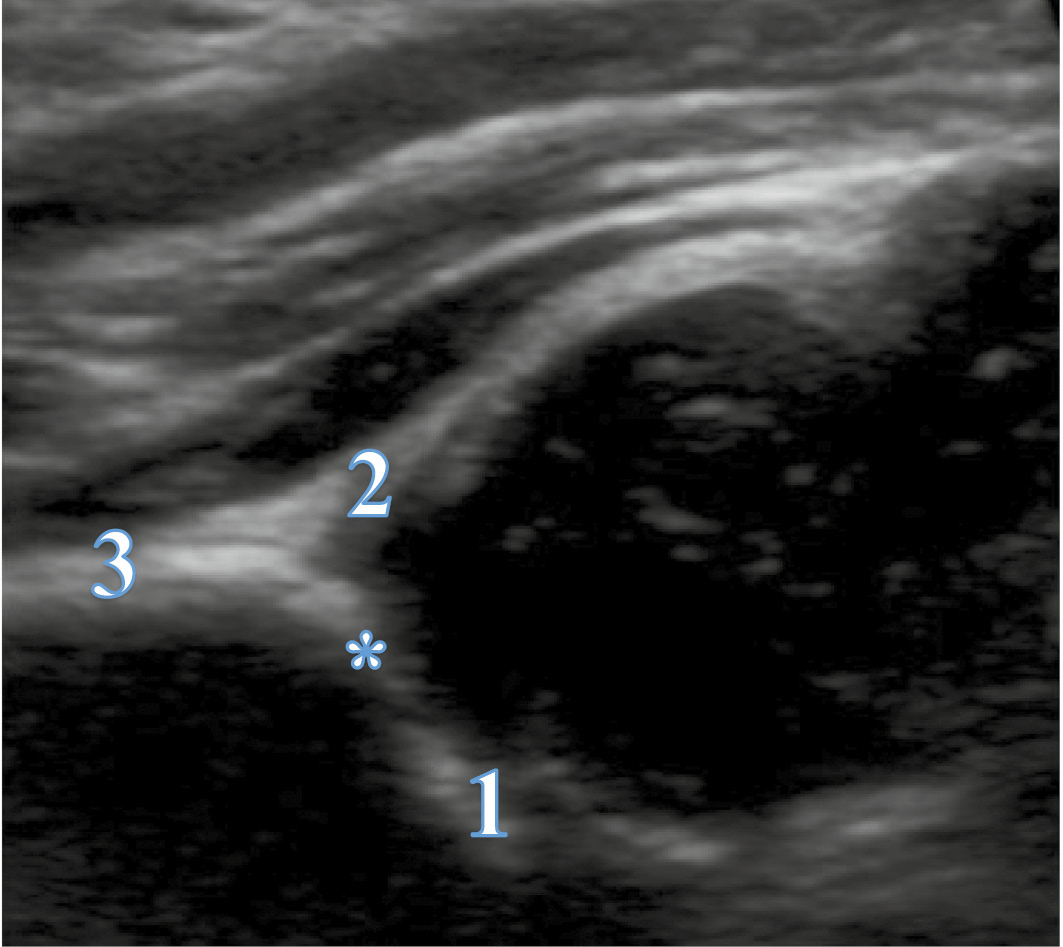
2. There is also a “usability list.” Three landmarks should be obtained to draw the lines for alpha and beta angles (Figure 2).
- Lower limb (Os ilium): the most ossified point of the ilium and where the alpha line goes through (and not to the triradiate cartilage)
- Labrum
- Straight iliac line
Figure 1. Graf Checklist.
1. Osteochondral border
2. Femoral head
3. Synovial fold
4. Capsule
5. Labrum
6. Cartilaginous roof
7. Bony roof
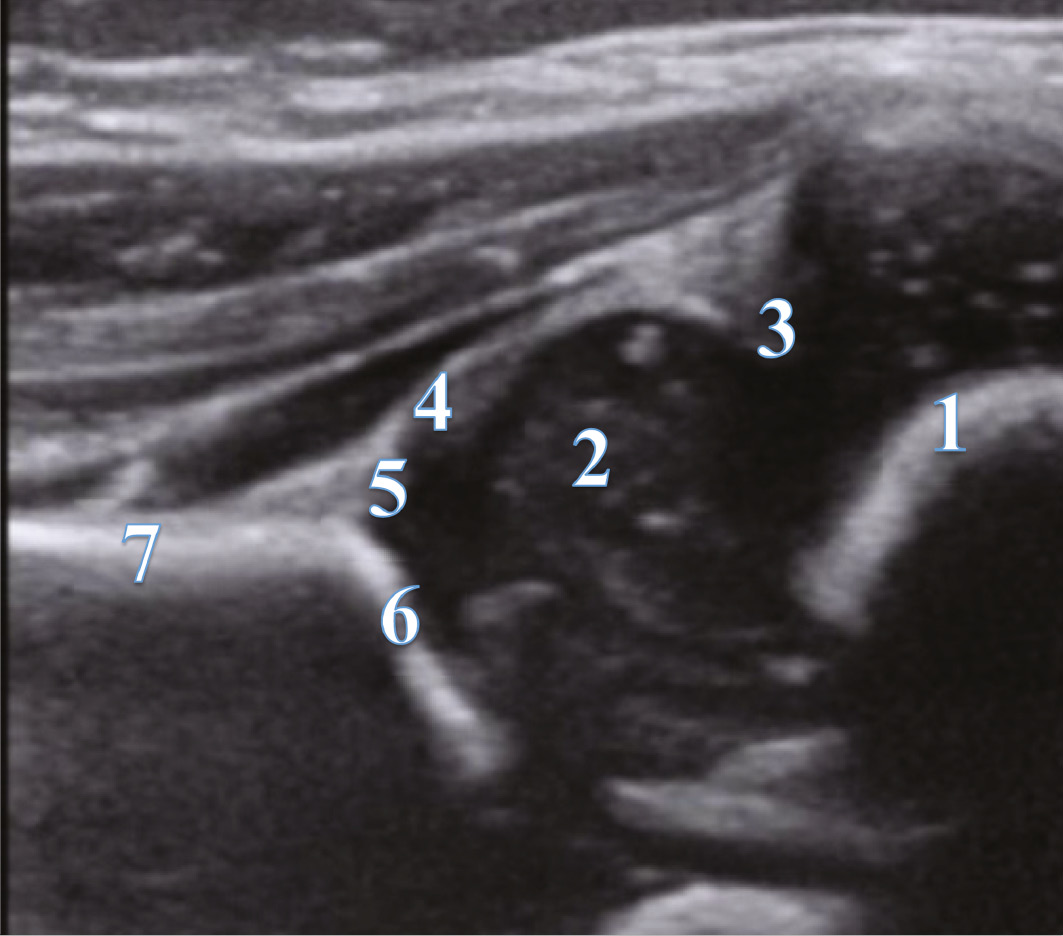
Figure 2. Checklist Two: Usability List.
1. Lower limb (Os ilium)
2. Labrum
3. Straight iliac line
* Turning point
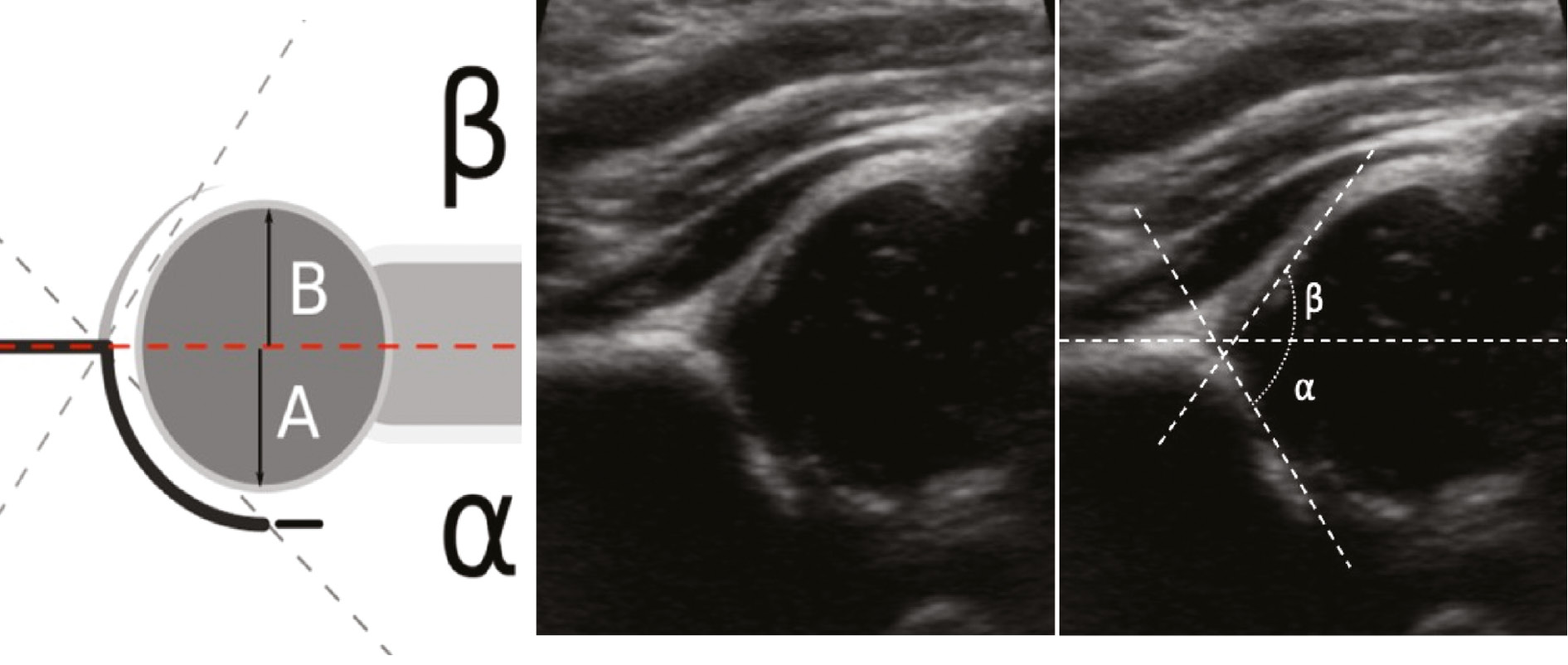
The straight iliac line is used to measure acetabular depth; this line should intersect the femoral head, with at least 50% of the head inferior to the line, with smaller values suggesting dysplasia. The angle between the straight iliac line and the lower limb line is called the alpha angle. The alpha angle should measure at least 60 degrees by 4 weeks and increase with age. A third line is drawn to determine cartilaginous coverage and goes from the so-called turning point (the exact point where the concavity of the acetabulum turns into a convexity). The angle between the baseline and this line is the so-called beta angle and should be no more than 55 degrees, with increased angles representing increased severity of subluxation (Figure 3).
Figure 3. Alpha and beta angles.
Once the learner has proven proficiency in this static method, the training continues with live patients. US evaluation of the infant hip categorizes hips into four types: normal, dysplastic, unstable, or dislocated. This reproducible, easy-to-follow system allows the immediate identification of hips that will require treatment. In evaluating trainee skill development, each US examination along with specific US images are evaluated by an expert. The trainee must identify all components of the checklist and usability list. Angles are then measured on the saved static images from the US exam, and immediate feedback is provided to the learners
The method currently taught to distinguish hips with pathology from those without represents the evolution of the so-called “Dynamic standard minimum examination.”7 We currently teach this method due to its proven ease of learning and reliability.8
Simplified Three-Step Method
Step 1. Determine Whether the Hip is Located or Dislocated
The simplified method keeps the patient on a regular exam table, avoiding the need for any specialized equipment. The examined hip is held at 90 degrees of flexion with slight adduction. The view in this plane is the so-called “transverse” image (Figure 4). The transducer is placed parallel to the long axis of the femur, and the position of the femoral head in relation to the acetabulum is determined. If the femoral head is in contact with the acetabulum, whether it may be dysplastic or not, that femoral head is located.
Figure 4. Schematic and overlay of a transverse image showing the position of the femoral head in relation to the acetabulum.

Step 2. Determine Whether the Hip is Stable or Unstable9
To assess stability under sonographic evaluation, the hip should be stressed by adducting and applying posteriorly directed force, simulating a Barlow test. Figure 5 demonstrates an unstable hip during the simulated Barlow test (Figure 5).
Figure 5. Unstable hip during simulated Barlow test.

Displacement of the femoral head can be measured during this maneuver by measuring the distance between two set points, typically the femoral head and the triradiate cartilage, before and after applying the stress. Displacement greater than 4 mm between the acetabulum and femoral head signifies instability.
Another option for determining stability is to look for the so-called “bird-in-flight” sign, a line drawn along the acetabulum and the proximal femoral metaphysis (Figure 6). This virtual line is akin to a Shenton line on a radiograph and should be contiguous. A broken line signifies an unstable hip.
Figure 6. Bird in flight sign.

Step 3. Determine Whether the Socket is Deep or Shallow10
A coronal view is obtained by rotating the transducer 90 degrees, producing an image analogous to an AP of the pelvis (although it is rotated 90 degrees on its side). To accurately assess acetabular development, these coronal images should be captured with a perfectly flat ilium, from which measurements can be constructed. A line is drawn along the lateral border of the ilium, akin to the straight iliac line, which should intersect the femoral head with at least 50% of the head below the line, with smaller values suggesting a shallow socket. This line provides an objective measure of the coverage. A second line can be drawn along the bony acetabular roof to the edge of the acetabulum. The angle between the baseline and this line is the acetabular roof angle. This angle should always be greater than 60 degrees and should increase progressively with age.
The recently validated three-step method provides a straightforward classification method into four types. This provides an even greater interobserver reliability when performing the sonographic examination.8
- Normal
- Dysplastic
- Unstable
- Dislocated
Classification of the hip can even be further simplified to:
- Normal (no treatment needed)
- Abnormal (treatment needed)
Specifics of Simulation Training for Ultrasound Examination of the Infant Hip
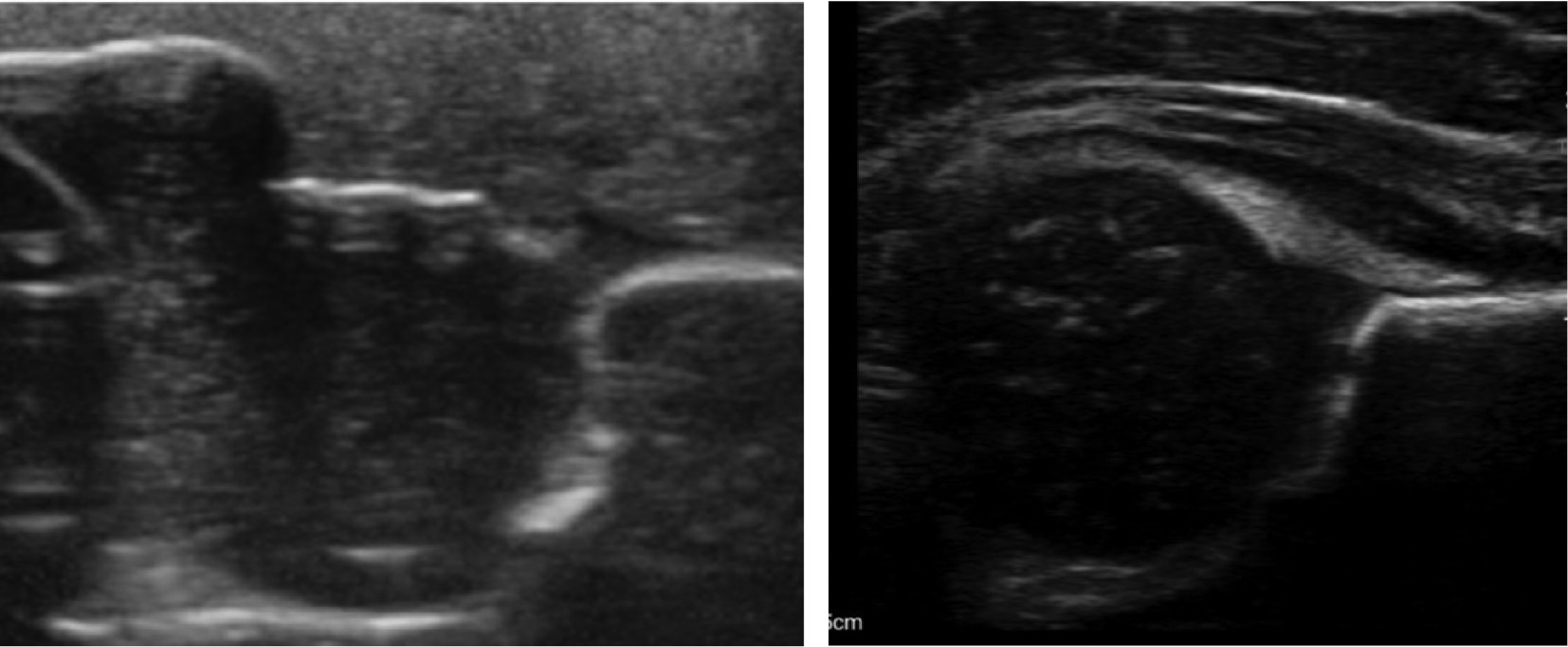
Using a Graf table (Figure 7) with a phantom baby (Figure 8), one can replicate all exam steps. By following all the steps listed above, on the simulation baby in the lateral decubitus position (Figure 9), one can acquire the skills to understand ultrasound evaluation of morphology. Limitations of using the phantom baby is that it does not allow for a dynamic exam and, although it allows understanding of normal anatomy, the phantom does not although the trainee to identify and measure pathologic findings (Figure 10). Once the trainee is comfortable and demonstrates proficiency with the phantom baby in the Graf table, we recommend practicing the exam with the phantom outside the positioner (Figure 9).
Figure 7. Graf Table.

Figure 8. Phantom baby.
Figure 9. Sample set up.
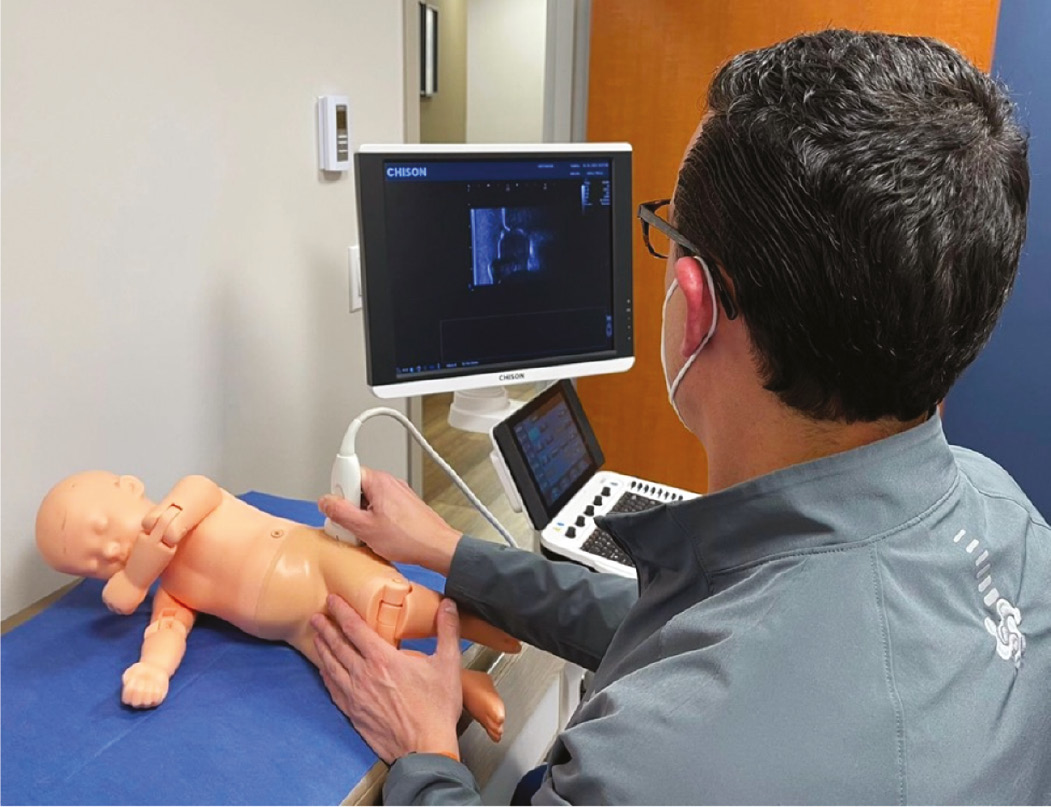
Figure 10. Phantom baby hip on left, real baby hip on right.
Rather than explicitly choosing and gaining confidence in one method or the other, it is more important to have a strong understanding of both to incorporate the principles effectively and evaluate hips consistently and efficiently. Following these established steps increases accuracy and produces high reproducibility rates.
Summary
The technique described by Graf was pioneering and has led the way to simplified examinations that enhance the clinician’s ability to detect hip dysplasia. Modern devices allow an immediate point-of-care access, which puts the information clinicians need during the visit, reducing costs and time.11 Within the time course of our training, we have evolved our method of teaching. Initially, the structure was lecture-based and the next step was to practice on live neonates. With incorporation of the first practicing POCUS on the phantom baby, we provide the learner with a low-fidelity model that allows better anatomic understanding. Only once the learner feels comfortable with this, can they progress to live patients.
Looking forward and strategizing how to improve current practice, a phantom baby with a dynamic component and incorporating VR with haptics to reproduce pathology are two projects that could expand and enhance the application of US to diagnosis and treatment of DDH.
Ultrasound is an effective tool for screening, diagnosing, intervention, and follow-up for DDH. It is a non-invasive, low-cost device that can enhance our early identification and treatment of DDH while decreasing the financial and medical sequelae that manifest throughout the patient’s life. By having the means to perform this during the clinical exam, it is now incorporated into the live examination, evaluation, and decision-making of an outpatient clinic visit and allows immediate intervention and initiation of treatment.
Disclaimer
There were no sources of funding for this paper. The authors have no conflicts of interest to report.
References
- Bialik V, Bialik GM, Blazer S, et al. Developmental dysplasia of the hip: a new approach to incidence. Pediatrics. 1999;103(1):93–99.
- Roovers EA, Boere-Boonekamp MM, Castelein RM, et al. Effectiveness of ultrasound screening for developmental dysplasia of the hip. Arch Dis Child Fetal Neonatal Ed. 2005;90(1):F25-F30.
- Litrenta J, Masrouha K, Wasterlain A, et al. Ultrasound evaluation of pediatric orthopaedic patients. J Am Acad Orthop Surg. 2020;28(16):e696-e705.
- Castaneda P. Pediatric hip dysplasia and evaluation with ultrasound. Pediatric Health. 2009;3(5):465–472.
- Stawicki SP, Bahner DP. Modern sonology and the bedside practitioner: evolution of ultrasound from curious novelty to essential clinical tool. Eur J Trauma Emerg Surg. 2015;41(5):457-460.
- Royall NA, Farrin E, Bahner DP, et al. Ultrasound-assisted musculoskeletal procedures: a practical overview of current literature. World J Orthop. 2011;2(7):57-66.
- Clarke NM, Castaneda P. Strategies to improve nonoperative childhood management. Orthop Clin North Am. 2012;43(3):281-289.
- Jejurikar N, Moscona-Mishy L, Rubio M, et al. What is the interobserver reliability of an ultrasound-enhanced physical examination of the hip in infants? a prospective study on the ease of acquiring skills to diagnose hip dysplasia. Clin Orthop Relat Res. 2021;479(9):1889-1896.
- Martus JE. Orthopaedic knowledge update. American Academy of Orthopaedic Surgeons; 2016.
- Castaneda P. Orthopaedic knowledge update. American Academy of Orthopaedic Surgeons; 2016: Chapter 20. Developmental Dysplasia of the Hip.
- Herrero C, Colon Y, Nagapurkar A, et al. Point-of-Care ultrasound reduces visit time and cost of care for infants with developmental dysplasia of the hip. Indian J Orthop. 2021;55:1-6.
Appendix
Supplies
- Graf table: $2030 U.S. (from 1800E), Mexican version $800 U.S.
- Phantom baby: $4000 U.S. (Kyoto Kagaku Phantom baby: see website for quote and manual of the evaluation specifics: https://www.kyotokagaku.com/en/products_data/us-13/).
- Transducer - linear transducer 5.2-5.7 MHz: $1,000–8,500 U.S.
- Total budget: $7000–$10000 U.S.