
Current Concept Review
Evidence-Based Management Strategies for Pediatric Pes Cavus
Division of Pediatric Orthopaedic Surgery, Columbia University, Vagelos College of Physician and Surgeons, New York, NY
Correspondence: Katherine A. Rosenwasser, MD, Morgan Stanley Children’s Hospital of New York, Floor 8N, 3959 Broadway, New York, NY 10032. E-mail: [email protected]
Received: March 15, 2022; Accepted: March 31, 2022; Published: May 1, 2022
DOI: 10.55275/JPOSNA-2022-0035
Volume 4, Number 2, May 2022
Abstract:
Pes cavus is defined as an abnormal elevation of the medial longitudinal arch of the foot. More than two-thirds of patients with pes cavus are found to have a neurologic diagnosis driving a muscle imbalance within the foot. Expedient clinical diagnosis of underlying pathology is paramount to facilitate proper neuraxial imaging studies and a referral to pediatric neurology. The goal of treatment in pes cavus is to obtain a painless, plantigrade, and supple foot. Nonoperative management is typically indicated in cases of mild nonprogressive deformity. Surgical management hinges heavily on physical and radiographic examination findings including the Coleman block test, which can help to determine the need for hind foot reconstruction.
Key Concepts:
- Pes cavus is frequently associated with underlying neurologic conditions such as Charcot-Marie-Tooth, cerebral palsy, Friedreich’s Ataxia, and spinal cord lesions.
- Non-operative management can provide symptomatic relief in static deformity that is relatively mild.
- Soft tissue reconstruction such as plantar fascia release and tendon transfers attempt to re-balance the foot but can be plagued with recurrence of deformity.
- Bony reconstruction for a rigid cavovarus foot may involve a first metatarsal or midfoot osteotomy to address a plantarflexed first ray. A lateral closing wedge can correct adductus, and a lateral calcaneal slide osteotomy can address fixed hindfoot varus.
- Triple arthrodesis may be indicated in the pediatric patient who has severe or recurrent deformity.
Introduction
Pes cavus in the pediatric patient is characterized by an elevation in the longitudinal arch of the foot (Figure 1).1 Isolated pes cavus may be an anterior deformity which is secondary to plantarflexion of the first ray (forefoot equinus) or less commonly, a posterior deformity due to dorsiflexion of the calcaneus (increased calcaneal pitch, also referred to as calcaneocavus) (Figure 2).2 “Global” pes cavus may also be seen, which is a combination of both anterior and posterior pes cavus.3 Additional foot deformities in other planes are also often encountered. Pes cavovarus, often associated with underlying neurologic conditions, is one such variant which is typically accompanied by hindfoot varus as well as pronation of the forefoot and clawing of the toes. Less commonly, pes cavovalgus with concomitant hindfoot valgus and a tight triceps surae muscle may be seen.
Figure 1. Plantarflexed first ray with increased inclination of metatarsals leads to weight-bearing on metatarsal heads.

Figure 2. This child has severe calcaneocavus foot deformity; radiographs will show elevated calcaneus pitch (Figure 11).

The key early deformity which usually drives the pes cavus is a plantarflexed first metatarsal.1 This can be initiated by an overactive peroneus longus which depresses the first metatarsal, elevates the medial longitudinal arch, and tightens the plantar fascia. Unfortunately, the vector of pull of the peroneus longus is increasingly optimized when the ankle is plantarflexed as is the case in some of these patients who also display equinus contractures.4 The plantarflexed first metatarsal head impacts the ground first during the gait cycle and hinders appropriate midfoot and subtalar eversion following heel strike. This increased inversion moment of the foot projects to the hindfoot. This is akin to a tripod where the first and fifth rays as well as the calcaneus form the three “legs”; a depressed first ray effectively places more pressure on the lateral border of the foot while also tilting the hindfoot segment into varus.1,4 In the advanced stages of deformity, the hindfoot varus may eventually become rigid and fixed, making it difficult to accommodate uneven terrain.
Pes cavus can be idiopathic, representing a variant of normal morphology in some patients that becomes symptomatic. This is often described as the “subtle” cavus foot or “under-pronator” and may be difficult to appreciate on physical examination as the obvious clinical signs of more profound pes cavus are typically absent.4 Attention must be paid while taking the patient’s history to screen for possible hereditary, developmental, or congenital pathology. Common neurologic conditions which may present with a cavus foot include Charcot-Marie-Tooth (CMT) disease, cerebral palsy, Friedreich’s ataxia, spinal cord lesions, poliomyelitis, and amniotic band syndrome. Other non-neurologic etiologies include prior posterior leg compartment syndrome (Figure 3), hindfoot trauma/malunion, or untreated/undertreated congenital idiopathic clubfoot.5
Figure 3. This 4-year-old boy has a cavovarus foot as a result of a compartment syndrome as an infant following femoral artery thrombosis.

Charcot-Marie-Tooth disease is a progressive peripheral motor neuron disease characterized by declining motor and sensory function in the extremities.6 There are several defined types of CMT, but the most common form (CMT Type I) is characterized by an abnormal myelin sheath, secondary to a lack of peripheral myelin protein 22 (PMP-22) encoded on chromosome 17.6 In CMT, distal motor weakness and imbalance often precedes the later development of sensory disturbances. Pes cavovarus is thought to develop as a result of selective denervation of the lateral and anterior muscle compartments.7 The relatively weaker peroneus brevis and anterior tibialis tendons are overcome by the antagonistic actions of the tibialis posterior and peroneus longus tendons. Increased recruitment of the peroneus longus plantarflexes the first ray and pronates the forefoot, and when combined with the inverting force of the posterior tibialis tendon, this creates compensatory hindfoot varus. Loss of strength of the intrinsic foot muscles, combined with increased firing of the hallux and lesser toe extensors, may also contribute to clawing of the toes.
Friedreich’s ataxia is an inherited disease in which lack of the frataxin mitochondrial protein causes degeneration of the posterior spinal column. As the disease progresses, patients can develop significant ataxia and lose the ability to ambulate. It has been estimated that 75% of individuals with Friedrich’s ataxia may manifest pes cavus.8 Sensorimotor imbalance in the extremities also frequently leads to foot deformity in multiple planes. Progressive equinovarus deformity and clawing of the toes may inhibit the ability to achieve a plantigrade foot and threaten ambulation potential, which is already difficult due to ataxia in these patients.9
The clinician must also be aware of other less common neurologic causes of pes cavus. When unilateral cavus is seen, this may suggest the presence of a syringomyelia or tethered spinal cord (Figure 4). Peripheral nerve injury affecting the peroneal nerve may produce pes cavus as a result of lateral and anterior compartment weakness. People with cerebral palsy also tend to develop various foot deformities, with the hemiplegic type more commonly manifesting pes cavovarus.10 Patients with sacral level myelomeningocele or poliomyelitis also often demonstrate a calcaneocavus foot which is characterized by a dorsiflexed calcaneus and relative weakness of the ankle plantarflexors.11
Figure 4. This boy with a syrinx has a unilateral cavovarus foot deformity (top) with claw toes (bottom).

Diagnosis
Clinical Evaluation
The symptomatic cavus foot presents with a constellation of historical features and physical exam findings. Patients that describe chronic and recurrent ankle sprains along with lateral ankle pain should be evaluated for pes cavus on radiographs. Excessive weight-bearing on the lateral border of the foot may manifest as callosities (Figure 5) foot pain or even stress fractures of the fifth metatarsal.12 Peroneal tendon pathology is another deleterious effect of the muscular imbalance and resultant lateral ankle instability and often presents on a spectrum ranging from tendonitis to subluxation or dislocation. Os peroneum syndrome may develop as an ossicle within the peroneus longus tendon that begins to fracture and fragment from repetitive activation of the tendon.13 Symptoms of plantar fasciitis may also be described due to elongation of the medial arch and forefoot pronation as well as a tight triceps surae. Developing painful plantar calluses under the first and fifth metatarsal head is often associated with the progression of a more rigid cavus deformity.
Figure 5. Lateral column overload can result in callosities over the 5th metatarsal base (top) and in extreme cases can result in stress fractures (bottom).

The “peek-a-boo” heel sign (Figure 6), in which the heel pad can be seen protruding medially when viewing the foot from the front, denotes varus hindfoot alignment.4 Other examination features common to many patients include prominence of the first metatarsal fat pads and a positive Silfverskiold test demonstrating tightness of the gastrocnemius.
Figure 6. The “peek-a-boo” heel sign seen in patients with hindfoot varus.

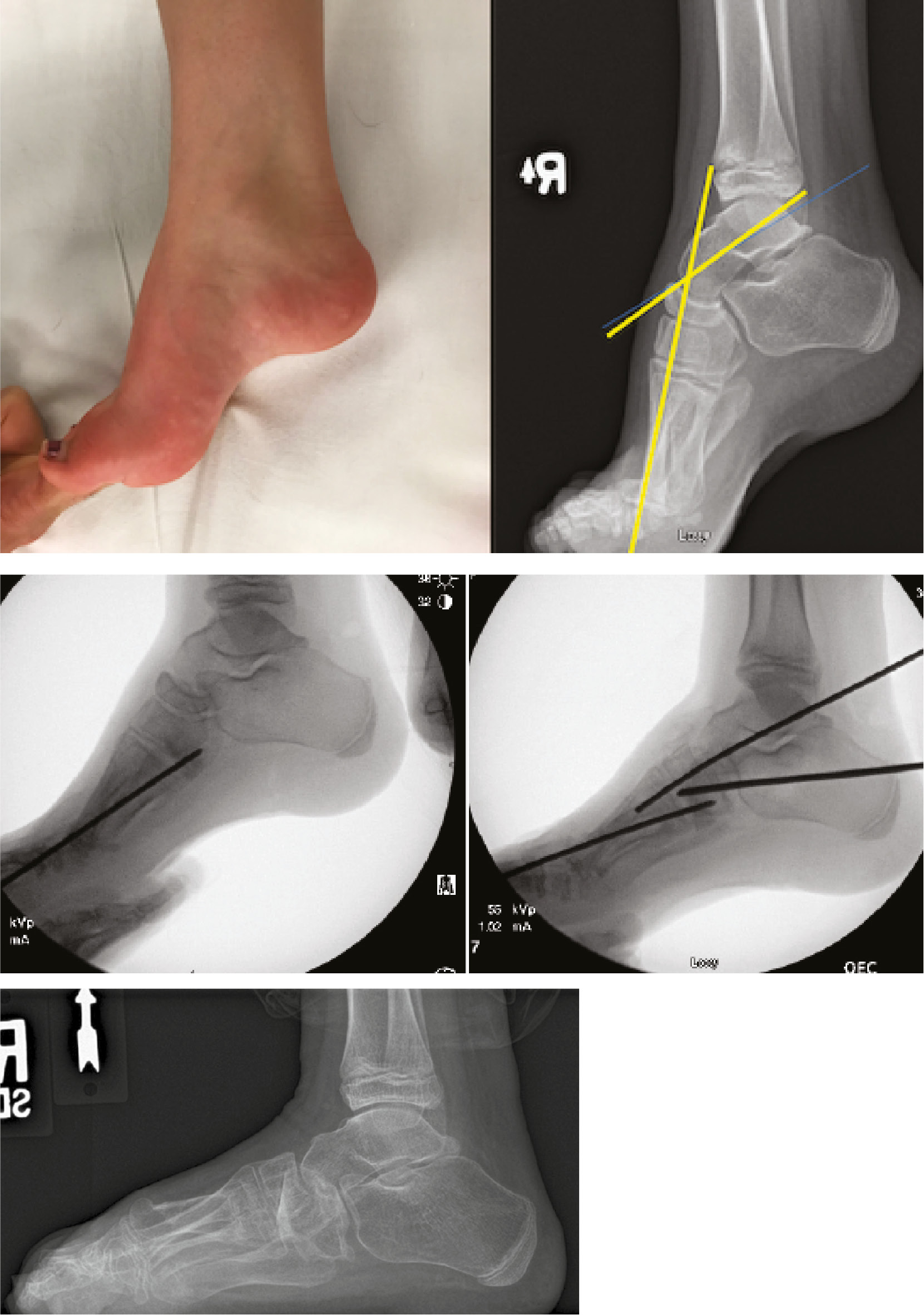
A critical physical examination maneuver to perform is the Coleman block test, which assesses the flexibility of the hindfoot in pes cavovarus.14 A block placed under the lateral foot neutralizes the elevated first ray and eliminates forefoot pronation, allowing the examiner to evaluate the hindfoot alone. A supple hindfoot will correct to a neutral or valgus position on the block (Figure 7), but a rigid hindfoot will remain fixed in a varus position (Figure 8). When a supple hindfoot is observed, this leads the examiner to assume that the plantarflexed first ray is the only pathologic deformity tilting the hindfoot into varus in the aforementioned “tripod” effect.4 Results of this test help dictate management strategies, since a flexible hindfoot will normalize once the forefoot deformity has been addressed, whereas a rigid hindfoot will typically require combined forefoot and hindfoot procedures to obtain deformity correction.
Figure 7. The Coleman block test on a patient with flexible hindfoot varus.

Figure 8. The Coleman block test on a patient with a rigid hindfoot.

Other physical examination findings may be variably present when underlying neurologic conditions exist. Clinical signs of spinal dysraphism or scoliosis necessitate that spinal cord lesions, Friedrich’s ataxia, or CMT be ruled out. Wasting of the first dorsal interosseous muscle of the hand is one such finding that is highly suggestive of CMT, and another early presenting manifestation of CMT may be hip pain with coexisting dysplasia.15 During assessment of gait, an unstable base of support or increased double limb stance suggests Friedreich’s ataxia. Additionally, sacral level spina bifida may be associated with plantar ulcers due to the tendency to develop calcaneocavus deformity (calcaneus dorsiflexion) and resultant pressure on the calcaneal tuberosity.11
Imaging
Radiographic evaluation of pes cavus is typically done with standing anteroposterior (AP) and lateral radiographs of the ankle as well as standing AP, lateral, and oblique radiographs of the foot. On the AP foot view, the talocalcaneal angle may be drawn to indicate the degree of hindfoot varus present. A talocalcaneal angle less than 20 to 25 degrees would be considered pathologic, with the normal range between 25 to 45 degrees (Figure 9). The talonavicular angle may additionally be drawn to assess the degree of forefoot adduction, with a value greater than 7 degrees indicating pathology. There may also be metatarsal overlap seen on this image that would indicate pronation of the forefoot. On the lateral foot view, Meary’s angle (lateral talo-first metatarsal angle) may be drawn. A break in this line is caused by plantarflexion of the first ray and a value more than 4 degrees apex dorsal indicates cavus (Figure 10). In the calcaneocavus foot with hindfoot dorsiflexion, the calcaneal pitch (or calcaneal inclination) is typically over 30 degrees (Figure 11).
Figure 9. An AP talocalcaneal angle less than 25 degrees is a sign of hind foot varus.

Figure 10. Cavus is noted radiographically if the talus-1st metatarsal angle is greater than 5 degrees.

Figure 11. Radiographs of a patient with calcaneocavus deformity (Figure 2) demonstrate a calcaneal pitch that is well over the normal 30 degrees.

Other findings on the lateral may include the sinus tarsi “see-through” sign (Figure 12) and “double talar dome” sign, a bell-shaped cuboid and increased distance between the base of the 5th metatarsal and medial cuneiform. The oblique radiograph may be useful for the diagnosis of metatarsal stress fractures (Figure 5) or calcaneonavicular coalitions.
Figure 12. Another radiographic characteristic for hind foot varus is the “see-through sign.”

While the cavus foot is best described using plain radiographs, other imaging modalities may be required in the work-up and diagnosis of associated neurologic conditions. This may include AP and lateral spine radiographs to assess for scoliosis, brain and spine magnetic resonance imaging (MRI) to evaluate for central neurologic processes and/or electrodiagnostic studies in the form of electromyography (EMG) or nerve conduction velocity (NCV) studies to assess for peripheral neurologic disease seen in CMT or other hereditary motor and sensory neuropathies.
Management
Conservative Management
Pediatric pes cavus is quite variable in severity and rate of progression since underlying neurologic conditions may create complex foot deformities. Severity and progression of disease is typically much higher in children than adults, so conservative treatment which is often more effective in the older population may not provide durable symptomatic relief in younger patients.5 Despite the difficulty in controlling the growing skeleton and soft tissues, the use of physical therapy and orthotics as well as night splints and serial casting have all been described as appropriate conservative modalities in children.
Physical therapy should be performed early in the course of treatment when flexible mild cavus is present and targeting soft tissue imbalance is more beneficial. Physical therapy should include lower extremity stretching and strengthening, with particular attention to heel cord and plantar fascia stretching. Improving strength in the relatively weaker anterior and lateral compartments may also provide some benefit, as the peroneus brevis and tibialis anterior tendons are specifically targeted. A study by Burns et al. demonstrated significant improvements in dorsiflexion and eversion strength as well as functional outcomes after a 12-week dedicated course of physical therapy in pes cavus.16 Botulinum toxin may provide some benefit in children with spastic cerebral palsy but has been shown to be ineffective in the progression of pes cavus during treatment of CMT.17
Insoles supporting the lateral border of the foot along with metatarsal bars may decrease foot pressure and minimize formation of ulcers and callouses. Although semirigid orthoses are frequently utilized in adults in order to decrease lateral foot and metatarsal head overload,18–20 it has been an anecdotal observation that the growing pediatric foot does not respond as well to insole wear.21 Three months of custom-molded insole wear in an adult population improved foot pain scores by 74% and decreased plantar foot pressures by 26% when compared to control subjects, but it is difficult to say if these results could be generalized to the pediatric population.22 Although physical therapy and orthotic wear may provide some degree of symptomatic relief, there is no literature to suggest that these modalities can alter the natural history of the progressive deformity.
In a flexible mild pes cavus, night splinting and casting have been used with variable results. This is best instituted to slow the progression of disease in early cavus or to prevent recurrence of deformity after operative correction. Serial casting for pes cavovarus provides derotational forces by inducing heel valgus and ankle dorsiflexion, abduction of the transverse tarsal and subtalar joints, and supination of the forefoot, all while stretching the tight structures.2 This is very similar to the final phases of the Ponseti casting method which is used to treat idiopathic clubfoot. Night splinting is also thought to prevent progression of disease since pes cavus and clawing of the toes becomes more pronounced while laying supine.2 Although there is a paucity of literature evaluating serial casting and splinting, a recent French study treated patients with a neurologic cavovarus foot with an untwisting walking cast followed by untwisting nocturnal splinting beginning at a mean age of 8.8 years. They were able to avoid surgery altogether through the end of growth in 10 of the 21 feet (48%), and they were able to delay surgery by an average of 4.5 years in the other 11 feet that progressed to needing surgical correction.23 Further high-powered studies are needed to elucidate the efficacy of serial casting and splinting, especially when pes cavus is more severe, since it can be challenging to enlist patient compliance during lengthy periods of immobilization.
Surgical Management
Soft tissue reconstruction
Most surgeons elect to begin with soft tissue reconstruction early in the course of disease while the deformities are supple. A flexible hindfoot as documented via the Coleman block test is crucial in pursuing soft tissue reconstruction on flexible deformities. It is easier to address soft tissue imbalance before progressive bony rigidity and malalignment prevent the opportunity to achieve a plantigrade, braceable foot. Azmaipairashvili et al. noted that soft tissue reconstruction should only be indicated when both forefoot and hindfoot flexibility is present.24 Using this criteria, they found that pain was significantly improved and no further procedures were necessary in a group of patients younger than the age of 8 to 12 years who underwent soft tissue procedures alone, despite minimal radiographic correction of calcaneal pitch and overall cavus deformity postoperatively.24
Lengthening of the heel cord, either through tendoachilles lengthening or gastrocnemius recession, may be indicated in the case of an equinocavus deformity. Patients must be selected to undergo heel cord lengthening carefully since cavus deformity (which can also be termed forefoot equinus) can give one the impression that hindfoot equinus is present (Figure 13) concomitant or future correctional osteotomies may alter the tension of the heel cord. For this reason, some authors advocate avoiding heel cord lengthening unless significant equinus remains after corrective osteotomies, while others recommend performing this prior to bony reconstruction so as not to compromise maintenance of fixation.21 Excessive lengthening of the heel cord can cause plantarflexion weakness and calcaneus positioning of the hindfoot.25
Figure 13. An initial examination of this foot may suggest that an Achilles or gastrocnemius fascial lengthening may be needed, yet when one ignores the forefoot equinus (Cavus) deformity, such a calf lengthening may not be needed after correction of the cavus.

Plantar fascia release directly addresses a tight structure which is a major component in driving flexible pes cavus, but this may not always produce durable results. Selective fasciotomy is usually done through a small plantar medial midfoot incision, but Steindler also recommended sectioning the intrinsic muscles of the foot (e.g., flexor hallucis brevis, abductor digiti minimi, and abductor hallucis) and the plantar calcaneocuboid ligament through a larger incision.26 However, some authors have noted27,28 that overcorrection is a risk of extensive plantar release as initially advocated by Steindler, so most surgeons now utilize a selective fasciotomy for better control of the soft tissues.29 Plantar fascia release is reported to have improved clinical outcomes with greater cavus correction when a first metatarsal osteotomy is performed at the same time.26 Plantar fascia release should also be performed judiciously when toe clawing is present, as this can potentially worsen such a deformity if the clawing is not addressed simultaneously.30
Peroneus longus to brevis transfer can decrease the plantarflexion forces on the first ray (which elevates the longitudinal arch) and is a good adjunct to first metatarsal or midfoot osteotomy and plantar fascia release. This is also considered when the peroneus longus tendon is visibly tense during active dorsiflexion of the ankle or the swing phase of gait.31 Given that a transferred tendon may lose some grading in strength, Leeuwesteijn et al. found that utilizing this particular transfer provided a tenodesis effect but they could not determine if there was increased eversion power. In a group of patients (27/52 feet or 52%) who underwent peroneus longus to brevis transfer, in combination with other procedures, no foot developed a recurrence of first ray plantarflexion postoperatively.31 Studies which report on the use of this tendon transfer manifest patient heterogeneity and often utilize concurrent procedures, so outcomes of an isolated peroneus longus tendon transfer are unclear. However, early use of this technique may avoid or delay the need for medial column osteotomies.32 Once the plantarflexed first ray has become more rigid, it appears to be beneficial to combine such a transfer with other techniques to address forefoot equinus, including first metatarsal or midfoot osteotomy (Figure 14) and plantar fascia release.
Figure 14. An 18-year-old female with residual cavus deformity undergoes plantar fascia release and 1st cuneiform osteotomy with allograft.

Posterior tibialis transfer to the dorsum of the foot (Figure 15) or to the dorsiflexors (tibialis anterior, peroneus tertius, or the extensor digitorum communis tendons) just proximal to the ankle as they pass under the extensor retinaculum also supplements dorsiflexion weakness of the tibialis anterior and removes a strong inverter.21,33–35
Figure 15. This 14-year-old girl with a paralyzed anterior tibialis undergoes posterior tibialis transfer through interosseus membrane. (A) The tibialis anterior is detached from its insertion, (B) a drill tunnel is created for interosseous transfer, (C) the tibialis anterior tendon is passed to the dorsum of the foot, and (D) ultimately sutured to the tibialis posterior to increase dorsiflexion power.
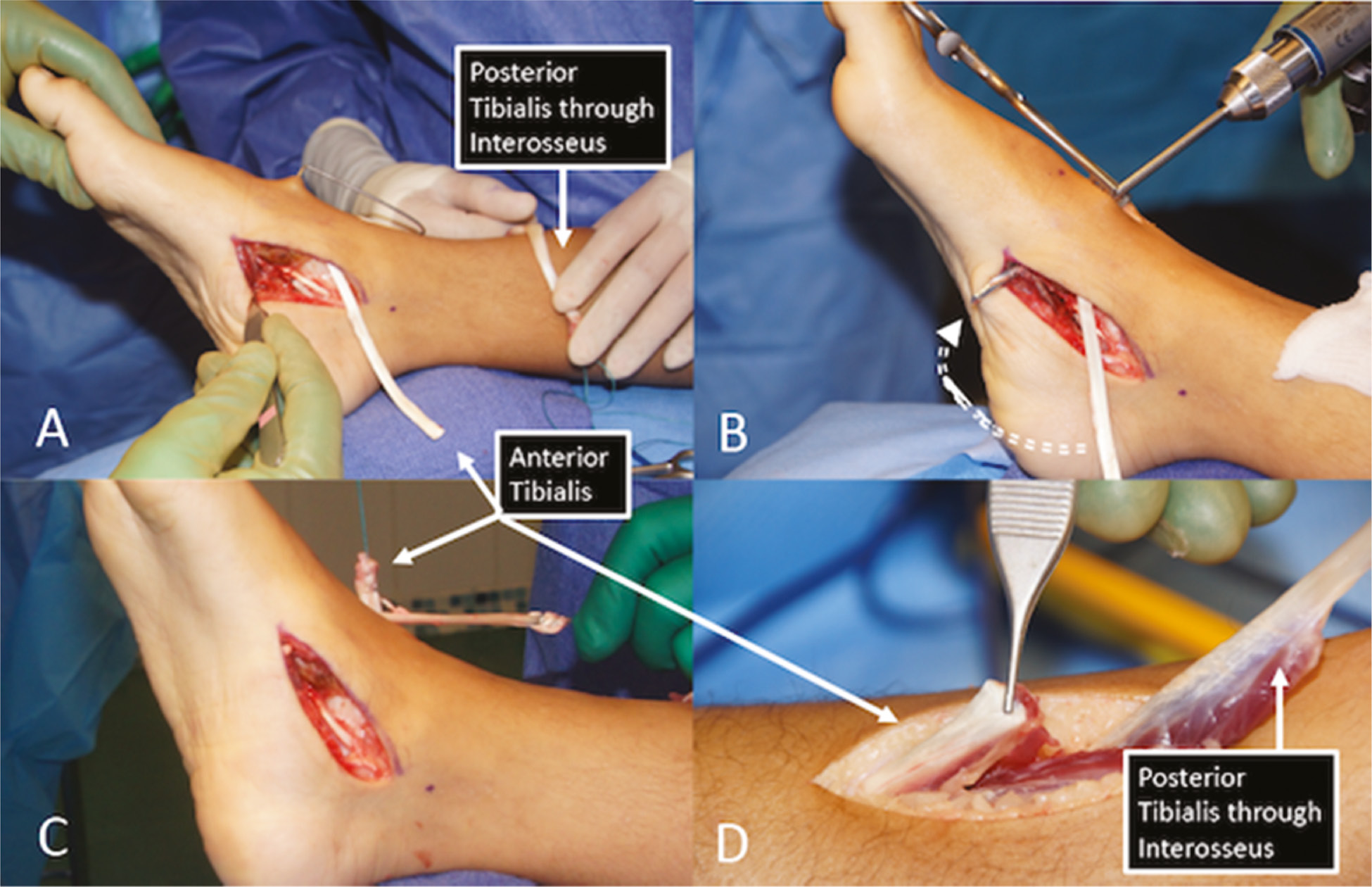
Dreher has utilized this technique combined with other necessary osteotomies and soft tissue procedures with good results in patients who manifest tibialis anterior weakness on the spectrum of a “drop foot.”34 Three-dimensional gait analysis in 14 patients (23 feet) following split posterior tibialis tendon transfer to the tibialis anterior and peroneus brevis/tertius demonstrated significant increases in ankle dorsiflexion during swing phase of gait with decreased peak plantar flexion of the ankle; patients also demonstrated preserved active and passive range of motion of the ankle on supine examination.34 Kaplan stated that transfer of the posterior tibialis tendon through the interosseous membrane, as opposed to a subcutaneous transfer maximizes its strength by providing an optimal vector of pull. They have utilized a transfer of the posterior tibialis tendon to the lateral cuneiform, which augments dorsiflexion strength, or to the cuboid, which augments both eversion and dorsiflexion strength.21 In some cases, posterior tibialis Z-lengthening is done at the distal tibia region near the musculotendinous junction or alternatively, near its distal insertion in concert with an extensive medial release of the talonavicular joint and plantar fascia. Release of the contracted plantar medial talonavicular capsule and soft tissues around the midfoot can be performed through the same incision.2
Other midfoot tendon transfers which have been described include tibialis anterior tendon transfer to the cuboid or lateral cuneiform, transfer of the long toe extensors to the cuboid or lateral cuneiform (modified Hibbs procedure),36 or a split tibialis anterior tendon transfer to the cuboid or peroneus tertius.37,38 When the tibialis anterior tendon is transferred closer to the lateral border of the foot, this not only provides an improved vector of pull for dorsiflexion strength but also can potentially augment eversion forces. In theory, this also eliminates the supination pull of the tendon, alleviating torsional forces which contribute to hindfoot varus and midfoot cavus. A split tendon transfer is another option in the care of children with neuromuscular deformities as this provides a balanced pull to both medial and lateral borders of the foot when significant spasticity is present. A tibialis anterior tendon transfer can also be strengthened by simultaneous transfer of the long toe extensors.39
Forefoot correction is especially helpful in those feet with underlying neurologic abnormalities where clawing of the toes is present, such as CMT and Friedrich’s ataxia. Weakness of the intrinsic muscles in these conditions leads to hyperextension at the MTP joints and compensatory flexion at the IP joints of the toes, which also secondarily tensions the plantar fascia and worsens longitudinal arch elevation and pronation of the forefoot. This is compounded by increased recruitment of the toe extensors for ankle dorsiflexion in order to compensate for progressive weakness of the tibialis anterior. Forefoot correction is frequently accomplished with transfer of the extensor hallucis longus through a drill hole or fixation with an interference screw in the first metatarsal neck as originally described by Jones.40,41 A concomitant tenodesis of the extensor hallucis longus to the extensor hallucis brevis may be used in children, instead of the typical hallux interphalangeal arthrodesis joint advocated by Jones, if a motion-preserving procedure is desired.41 This may be supplemented by extensor digitorum longus transfer to the lesser metatarsal necks when lesser toe clawing is present, as initially described by Hibbs.36 These transfers help to reorient the pull of the relatively stronger extrinsic tendons, converting a deforming force into a force which neutralizes elevation of the metatarsals and eliminates weight-bearing on the metatarsal heads.
Overall, studies which examine the outcomes of isolated soft tissue procedures in the absence of concomitant bony reconstruction are lacking. Dwyer has previously stated that soft tissue procedures more often provide temporary improvement and may not be long-lasting, but these procedures can slow the progression of rigid deformity over time.42 The relatively low rate of complications with these procedures makes them an attractive option to address early muscle imbalance in the flexible variants of pes cavus.
Bony reconstruction
Bony reconstruction, usually with realignment osteotomies, is necessary when the Coleman block test demonstrates a rigid hindfoot or when soft tissue procedures fail to resolve deformity. These osteotomies should be carried out in a methodical fashion to address the forefoot, midfoot, and hindfoot segments sequentially, taking into account coexisting foot abnormalities in all planes.
In the early stages of a flexible pes cavus, when the hindfoot varus is not fixed, soft tissue procedures may not always correct the primary forefoot equinus. In this scenario, authors have advocated for a first metatarsal dorsiflexion osteotomy11 or plantar opening wedge osteotomy of the medial cuneiform,29 either in combination43 or isolation. When a first metatarsal osteotomy is performed in isolation, it may also be necessary to perform second and third metatarsal osteotomies to enhance correction of forefoot pronation.33 Proponents of a cuneiform or midfoot osteotomy (Figure 16) point to the fact that the apex of the deformity in the sagittal plane is typically centered closer to the cuneiform region.2
Figure 16. This 14-year-old girl with Peter Syndrome has severe cavus with an apex of the deformity located at the navicular (top). The treating surgeon initially performed a 1st cuneiform osteotomy (middle left) without obtaining full correction. As a result, a naviculectomy and cuboid osteotomy was added (middle right). At 1-year follow-up, the patient had good correction (bottom).
Medial cuneiform plantar opening wedge osteotomy with an intact dorsal hinge allows for insertion of bone graft plantarly to neutralize at the apex of the cavus component and thus flatten the longitudinal arch (Figure 14). Wicart has also advocated for plantar opening wedge osteotomy of all three cuneiforms jointly in order to better correct forefoot pronation, as opposed to medial cuneiform osteotomy alone.2 Wicart demonstrated full or partial correction of cavus deformity in 75% of children at a follow-up of at least 5 years following this particular cuneiform osteotomy.29 It should be noted, however, that a cuneiform osteotomy may alter the flexibility and architecture of the hindfoot, so care must be taken to avoid inducing deformity in an adjacent segment of the foot.44
Other midfoot osteotomies have been used less frequently with good outcomes in a forefoot driven cavus, including the Japas osteotomy.45 The Japas osteotomy is a dorsal closing wedge osteotomy through the entire midfoot with the apex at the navicular and extending medially and laterally to end just proximal to the first and fifth tarsometatarsal joints. Meary also proposed a wedge tarsectomy which involved a closing wedge osteotomy through the navicular, cuboid and cuneiform bones, which is another variant of the multiple described midfoot osteotomies.46 Some authors choose to simply utilize a wedge osteotomy at the medial cuneiform and cuboid bones, addressing the medial and lateral borders of the foot while avoiding an osteotomy traversing the entire midfoot.47,48 This may not be as powerful in correcting forefoot pronation, but it may present less morbidity and postoperative stiffness when compared to osteotomies through the entire midfoot.24 Faldini reported good to excellent outcomes in 92% of patients (n=24 feet) with flexible hindfoot varus following a combination of plantar fasciotomy, osteotomy through the cuboid and naviculocuneiform joint, Jones extensor hallucis longus transfer, and dorsiflexion osteotomy of the first metatarsal.47 Mean calcaneal pitch improved by an average of 10 degrees, and the mean Meary angle improved substantially from 25 degrees to 2 degrees postoperatively. Even when performing separate wedge resections of the cuboid and naviculocuneiform joint, radiographic correction at the apex of the deformity in the midtarsal region was achieved while midfoot motion was preserved.47
With the myriad of osteotomies available, especially through the midfoot region, it is critical that the surgeon determine where the apex of the cavus deformity is centered in the sagittal plane (Figure 16). Each patient requires a personalized approach to address forefoot equinus. Tarsal osteotomies should be selected if the apex of the cavus deformity lies about the midfoot region. If the deformity is centered closer to the first metatarsal, then a dorsiflexion first metatarsal osteotomy, typically in combination with plantar fascia release and peroneus longus transfer, is indicated. Additionally, one study has suggested that dorsal hemiepiphysiodesis of the first metatarsal along with plantar fascia release in skeletally immature patients (n=24 feet, age 7-13 years) may be another option to address forefoot equinus centered at the first metatarsal. The authors demonstrated good clinical outcomes and correction of hindfoot varus as well as significant improvements in radiographic parameters including Meary’s angle, with full correction achieved in younger patients by skeletal maturity.49
When Coleman block testing demonstrates a rigid hindfoot, the surgeon should perform a calcaneal osteotomy. This can be done in several ways, with most surgeons utilizing a lateral calcaneal slide osteotomy or Dwyer lateral closing wedge osteotomy, which serves to shorten the lateral column.42,50 This induces hindfoot valgus and secondarily centralizes the pull of the ankle dorsiflexors and plantarflexors across the hindfoot. In a recent study utilizing three-dimensional printed models of the hindfoot, performing a Dwyer osteotomy significantly improved hindfoot valgus angle, coronal calcaneal tilt, and lateralization of the weight-bearing surface, as opposed to oblique slide osteotomy.51 These radiographic parameters were even further improved when the Dwyer osteotomy was utilized to internally rotate the posterior calcaneal tuberosity fragment. Mubarak reported on the sequential application of metatarsal osteotomy, plantar opening wedge of the medial cuneiform and cuboid osteotomy, and calcaneal osteotomy with soft tissue procedures added as needed to address rigid hindfoot varus. They found that this stepwise approach to segmental deformity provided good to excellent outcomes and adequate correction of Meary and Hibb angles in a group of 20 feet.43 Wicart utilized a similar approach, performing plantar opening wedge osteotomy of the three cuneiform bones with the addition of a plantar release and Dwyer osteotomy when rigid hindfoot varus was present, averaging a cavus correction of 74% in a group of 36 feet.29 Calcaneal osteotomy is a very effective procedure when combined with the other procedures which are indicated to treat segmental deformity. This is supported by an older study by Lariviere et al. which found a very high cavus recurrence rate approaching 71% when Dwyer osteotomy was performed in isolation without the addition of midfoot osteotomies.52 When extensive bony reconstruction is required, the major goal of surgery is to avoid stiffness and prevent degenerative changes over time while also providing adequate pain relief and functioning. By addressing deformity during growth in this manner, with a careful application of procedures as they are indicated, a plantigrade foot can be maintained following skeletal maturity.
Salvage options
Triple arthrodesis has been described as a salvage procedure in which the subtalar, talonavicular, and calcaneocuboid joints are fused in proper anatomic alignment (Figure 17). A major drawback of this procedure is the loss of subtalar and transverse tarsal motion as well as the fact that addressing the hindfoot does not always target the apex of the deformity which lies closer to the midfoot and cuneiforms. It is acknowledged that this can produce pain relief and provide satisfactory functioning in patients with severe, rigid deformity and concomitant peripheral neuropathy, but most studies demonstrate that adjacent tibiotalar instability and arthritis tends to develop at an early age. Saltzman reported on a group of 67 feet which required triple arthrodesis, finding that 95% of these patients continue to state that they were satisfied with the procedure, even though many of them developed radiographic arthritis at adjacent ankle and midfoot joints, along with foot pain in some.53 Another study also affirmed this finding, with 91% of patients stating they would undergo the procedure again despite the presence of radiographic signs of ankle arthritis.54 Salvage procedures are effective when pain control is the primary goal of the surgery, but patients must be counseled about the likelihood of early arthritis as well as loss of segmental foot motion and function.
Figure 17. This 19-year-old young man with ataxia telangiectasia had four previous procedures for cavovarus deformity. Triple arthrodesis was finally successful in maintaining a balanced foot. This case illustrates the difficulty in predicting outcome when deformity is a result of ataxia.

Complications and Outcomes
There are various sequelae which can develop in the child with untreated pes cavus. Over time, patients may suffer from symptoms of plantar fasciitis. The plantar fascia becomes significantly contracted, especially in the presence of forefoot pronation and gastrocnemius tightness which elevates the arch even more. Stress fracture of the fourth and fifth metatarsals may occur due to progressive lateral column overload (Figure 5). Peroneal tendon subluxation and tendinitis often develop and may predispose to tearing of the peroneal tendons as they become progressively stretched and attenuated. Hallux sesamoiditis is another consequence of increasing plantarflexion of the first ray which exerts significant pressures over the extended first metatarsophalangeal joint.
Chronic ankle instability may develop as a result of an attenuated lateral ankle ligamentous complex, especially in the subtle pes cavus with a delayed diagnosis. Untreated lateral ankle instability may lead to degenerative joint disease of the ankle with varus collapse in adulthood. There is a minimal role for lateral ankle reconstruction (Broström procedure) in children, but some surgeons have utilized this procedure in adolescents and adults after bony realignment has been performed.21 To date, there are no clear indications for when to include a lateral ankle ligament reconstruction during the course of treatment.
Summary
Treatment goals need to be considered fully prior to surgical intervention, and deformity should be addressed methodically from the forefoot to the hindfoot. Moreover, in patients who manifest underlying neurological pathology, proper timing of surgical intervention is controversial, as it is often difficult to predict the course of disease. Soft tissue procedures are often used to temporize the patient and delay more invasive bony reconstruction. However, combining osseous reconstruction with soft tissue balancing is typically more productive in the treatment of pes cavus, especially in an older child where rigid deformity is present.
Soft tissue releases and tendon transfers may allow for a more supple, plantigrade foot and reduce foot pain with activity. When more severe pes cavus is present, the Coleman block test can help the clinician to pursue midfoot and/or forefoot osteotomies if the hindfoot is flexible or to add a calcaneal osteotomy when a rigid hindfoot is recognized. We advocate for first metatarsal dorsiflexion osteotomy as well as medial cuneiform osteotomy and cuboid osteotomy to address a primarily forefoot-driven deformity. Achieving a neutral hindfoot position through calcaneal osteotomies may often unmask forefoot pronation, which can then be corrected with metatarsal osteotomies and the modified Jones procedure. Individualized treatment plans often require a variety of procedures which have been discussed, so the surgeon must be familiar with the various options which have been described to correct pes cavus and its secondary deformities.
Additional Links
- POSNAcademy: Plantar-Medial Release (PMR) for Cavovarus Foot Deformity, Vincent S. Mosca, MD—https://bit.ly/3NUbQc2
- POSNAcademy: Mid-tarsal Osteotomies: Tips of the Trade, Vincent S. Mosca, MD—https://bit.ly/3LOUcER
Disclaimer
The authors have no conflicts of interest to disclose.
References
- Mosca VS. The cavus foot. J Pediatr Orthop. 2001;21(4):423–424.
- Wicart P. Cavus foot, from neonates to adolescents. Orthop Traumatol Surg Res. 2012;98(7):813-828. doi:10.1016/j.otsr.2012.09.003
- Vogler HW. Surgical management of neuromuscular deformities of the foot and ankle in children and adolescents. Clin Podiatr Med Surg. 1987;4(1):175-206.
- Manoli A, Graham B. The subtle cavus foot, “the underpronator.” Foot Ankle Int. 2005;26(3):256-263. doi:10.1177/107110070502600313
- Seaman TJ, Ball TA. Pes cavus. In: StatPearls. StatPearls Publishing; 2022. Available at: http://www.ncbi.nlm.nih.gov/books/NBK556016/. Accessed March 13, 2022.
- Maranho DA, Volpon JB. Acquired pes cavus in charcot-marie-tooth disease. Rev Bras Ortop. 2009;44(6):479-486. doi:10.1016/S2255-4971(15)30144-0
- Sanpera I, Villafranca-Solano S, Muñoz-Lopez C, et al. How to manage pes cavus in children and adolescents? EFORT Open Rev. 2021;6(6): 510-517. doi:10.1302/2058-5241.6.210021
- Delatycki MB, Corben LA. Clinical features of friedreich ataxia. J Child Neurol. 2012;27(9):1133-1137. doi:10.1177/0883073812448230
- Delatycki MB, Holian A, Corben L, et al. Surgery for equinovarus deformity in Friedreich’s ataxia improves mobility and independence. Clin Orthop. 2005;(430):138-141. doi:10.1097/01.blo.0000150339.74041.0e
- Eilert RE. Cavus foot in cerebral palsy. Foot Ankle. 1984;4(4):185-187. doi:10.1177/107110078400400404
- Mosca. The foot. In: Weinstein SL and Flynn JM, eds. Lovell & Winter’s Pediatric Orthopaedics. Seventh edition. Lippincott Williams & Wilkins; 2014.
- Williams DS, McClay IS, Hamill J. Arch structure and injury patterns in runners. Clin Biomech Bristol Avon. 2001;16(4):341-347. doi:10.1016/s0268-0033(01)00005-5
- Chagas-Neto FA, de Souza BNC, Nogueira-Barbosa MH. Painful os peroneum syndrome: underdiagnosed condition in the lateral midfoot pain. Case Rep Radiol. 2016;2016:8739362. doi:10.1155/2016/8739362
- Coleman SS, Chesnut WJ. A simple test for hindfoot flexibility in the cavovarus foot. Clin Orthop Relat Res. 1977;(123):60-62. PMID: 852192
- Yagerman SE, Cross MB, Green DW, et al. Pediatric orthopedic conditions in Charcot-Marie-Tooth disease: a literature review. Curr Opin Pediatr. 2012;24(1):50-56. doi:10.1097/MOP.0b013e32834e9051
- Burns J, Raymond J, Ouvrier R. Feasibility of foot and ankle strength training in childhood Charcot-Marie-Tooth disease. Neuromuscul Disord NMD. 2009;19(12):818-821. doi:10.1016/j.nmd.2009.09.007
- Burns J, Scheinberg A, Ryan MM, et al. Randomized trial of botulinum toxin to prevent pes cavus progression in pediatric Charcot-Marie-Tooth disease type 1A. Muscle Nerve. 2010;42(2):262-267. doi:10.1002/mus.21685
- Mueller MJ, Lott DJ, Hastings MK, et al. Efficacy and mechanism of orthotic devices to unload metatarsal heads in people with diabetes and a history of plantar ulcers. Phys Ther. 2006;86(6):833-842.
- Chalmers AC, Busby C, Goyert J, et al. Metatarsalgia and rheumatoid arthritis--a randomized, single blind, sequential trial comparing 2 types of foot orthoses and supportive shoes. J Rheumatol. 2000;27(7):1643-1647.
- Crosbie J, Burns J. Are in-shoe pressure characteristics in symptomatic idiopathic pes cavus related to the location of foot pain? Gait Posture. 2008;27(1):16-22. doi:10.1016/j.gaitpost.2006.12.013
- Kaplan JRM, Aiyer A, Cerrato RA, et al. Operative treatment of the cavovarus foot. Foot Ankle Int. 2018;39(11):1370-1382. doi:10.1177/1071100718798817
- Burns J, Crosbie J, Ouvrier R, et al. Effective orthotic therapy for the painful cavus foot: a randomized controlled trial. J Am Podiatr Med Assoc. 2006;96(3):205-211. doi:10.7547/0960205
- d’Astorg H, Rampal V, Seringe R, et al. Is non-operative management of childhood neurologic cavovarus foot effective? Orthop Traumatol Surg Res. 2016;102(8):1087-1091. doi:10.1016/j.otsr.2016.09.006
- Azmaipairashvili Z, Riddle EC, Scavina M, et al. Correction of cavovarus foot deformity in Charcot-Marie-Tooth disease. J Pediatr Orthop. 2005;25(3):360-365. doi:10.1097/01.bpo.0000150807.90052.98
- Natarajan R, Ribbans WJ. Achilles tendon involvement in pediatric conditions. In: Maffulli N, Almekinders LC, eds. The Achilles Tendon. New York, NY: Springer; 2007:236-251.
- Steindler A. The treatment of pes cavus (hollow claw foot). Arch Surg. 1921;2(2):325-337. doi:10.1001/archsurg.1921.01110050143007
- Paulos L, Coleman SS, Samuelson KM. Pes cavovarus. Review of a surgical approach using selective soft-tissue procedures. J Bone Joint Surg Am. 1980;62(6):942-953.
- Sherman FC, Westin GW. Plantar release in the correction of deformities of the foot in childhood. J Bone Joint Surg Am. 1981;63(9):1382-1389.
- Wicart P, Seringe R. Plantar opening-wedge osteotomy of cuneiform bones combined with selective plantar release and dwyer osteotomy for pes cavovarus in children. J Pediatr Orthop. 2006;26(1):100-108. doi:10.1097/01.bpo.0000189005.78045.17
- Lin T, Gibbons P, Mudge AJ, et al. Surgical outcomes of cavovarus foot deformity in children with Charcot-Marie-Tooth disease. Neuromuscul Disord. 2019;29(6):427-436. doi:10.1016/j.nmd.2019.04.004
- Leeuwesteijn AEEPM, de Visser E, Louwerens JWK. Flexible cavovarus feet in Charcot-Marie-Tooth disease treated with first ray proximal dorsiflexion osteotomy combined with soft tissue surgery: a short-term to mid-term outcome study. Foot Ankle Surg. 2010;16(3):142-147. doi:10.1016/j.fas.2009.10.002
- Boffeli TJ, Tabatt JA. Minimally invasive early operative treatment of progressive foot and ankle deformity associated with charcot-marie-tooth disease. J Foot Ankle Surg. 2015;54(4):701-708. doi:10.1053/j.jfas.2014.03.019
- Louwerens JWK. Operative treatment algorithm for foot deformities in Charcot-Marie-Tooth disease. Oper Orthopadie Traumatol. 2018;30(2):130-146. doi:10.1007/s00064-018-0533-0
- Dreher T, Wolf SI, Heitzmann D, et al. Tibialis posterior tendon transfer corrects the foot drop component of cavovarus foot deformity in Charcot-Marie-Tooth disease. J Bone Joint Surg Am. 2014;96(6):456-462. doi:10.2106/JBJS.L.01749
- Hsu JD, Hoffer MM. Posterior tibial tendon transfer anteriorly through the interosseous membrane: a modification of the technique. Clin Orthop Relat Res. 1978;(131):202-204. PMID: 657623
- Hibbs RA. An operation for “claw foot.” J Am Med Assoc. 1919;73(21):1583-1585. doi:10.1001/jama.1919.02610470019007
- Lullo B, Nazareth A, Rethlefsen S, et al. Split tibialis anterior tendon transfer to the peroneus brevis or tertius for the treatment of varus foot deformities in children with static encephalopathy: a retrospective case series. J Am Acad Orthop Surg Glob Res Rev. 2020;4(5):e2000044. doi:10.5435/JAAOSGlobal-D-20-00044
- Ward CM, Dolan LA, Bennett DL, et al. Long-term results of reconstruction for treatment of a flexible cavovarus foot in Charcot-Marie-Tooth disease. J Bone Joint Surg Am. 2008;90(12):2631-2642. doi:10.2106/JBJS.G.01356
- Huber M. What is the role of tendon transfer in the cavus foot? Foot Ankle Clin. 2013;18(4):689-695. doi:10.1016/j.fcl.2013.08.002
- Jones R. III. The soldier’s foot and the treatment of common deformities of the foot. Br Med J. 1916;1(2891):749-753. doi:10.1136/bmj.1.2891.749
- de Palma L, Colonna E, Travasi M. The modified Jones procedure for pes cavovarus with claw hallux. J Foot Ankle Surg. 1997;36(4):279-283. doi:10.1016/s1067-2516(97)80073-7
- Dwyer FC. Osteotomy of the calcaneum for pes cavus. J Bone Joint Surg Br. 1959;41-B(1):80-86. doi:10.1302/0301-620X.41B1.80
- Mubarak SJ, van Valin SE. Osteotomies of the foot for cavus deformities in children. J Pediatr Orthop. 2009;29(3):294-299. doi:10.1097/BPO.0b013e31819aad20
- Viehweger E, Jacquemier M, Launay F, et al. First cuneiform osteotomy alters hindfoot architecture. Clin Orthop. 2005;441:356-365. doi:10.1097/01.blo.0000180605.535851.82
- Japas LM. Surgical treatment of pes cavus by tarsal V-osteotomy. Preliminary report. J Bone Joint Surg Am. 1968;50(5):927-944.
- Simon AL, Seringe R, Badina A, et al. Long term results of the revisited Meary closing wedge tarsectomy for the treatment of the fixed cavo-varus foot in adolescent with Charcot-Marie-Tooth disease. Foot Ankle Surg. 2019;25(6):834-841. doi:10.1016/j.fas.2018.11.005
- Faldini C, Traina F, Nanni M, et al. Surgical treatment of cavus foot in Charcot-Marie-tooth disease: a review of twenty-four cases: AAOS exhibit selection. J Bone Joint Surg Am. 2015;97(6):e30. doi:10.2106/JBJS.N.00794
- Chen ZY, Wu ZY, An YH, et al. Soft tissue release combined with joint-sparing osteotomy for treatment of cavovarus foot deformity in older children: Analysis of 21 cases. World J Clin Cases. 2019;7(20):3208-3216. doi:10.12998/wjcc.v7.i20.3208
- Sanpera I, Frontera-Juan G, Sanpera-Iglesias J, et al. Innovative treatment for pes cavovarus: a pilot study of 13 children. Acta Orthop. 2018;89(6):668-673. doi:10.1080/17453674.2018.1486525
- Barg A, Hörterer H, Jacxsens M, et al. [Dwyer osteotomy : Lateral sliding osteotomy of calcaneus]. Oper Orthop Traumatol. 2015;27(4):283-297. doi:10.1007/s00064-015-0409-5
- An TW, Michalski M, Jansson K, et al. Comparison of lateralizing calcaneal osteotomies for varus hindfoot correction. Foot Ankle Int. 2018;39(10):1229-1236. doi:10.1177/1071100718781572
- Larivière JY, Miladi L, Dubousset J, et al. Failure of Dwyer’s procedure in internal pes cavus in children. Physiopathological considerations and therapeutic deductions. Rev Chir Orthop Reparatrice Appar Mot. 1985;71(8):563-573. French. PMID: 3834543
- Saltzman CL, Fehrle MJ, Cooper RR, et al. Triple arthrodesis: twenty-five and forty-four-year average follow-up of the same patients. J Bone Joint Surg Am. 1999;81(10):1391-1402.
- Pell RF, Myerson MS, Schon LC. Clinical outcome after primary triple arthrodesis. J Bone Joint Surg Am. 2000;82(1):47-57. doi:10.2106/00004623-200001000-00006