
Don’t Do This Case Report
Over-Reaming the Humerus to Place an IM Lengthening Nail
The University of Alabama at Birmingham, Department of Orthopaedic Surgery, Birmingham, AL
Correspondence: Shawn R. Gilbert, MD, 1600 7th Ave. S., Lowder Bldg., Suite 316, Birmingham, AL 35233. E-mail: [email protected]
Received: February 16, 2022; Accepted: March 21, 2022; Published: May 1, 2022
DOI: 10.55275/JPOSNA-2022-0026
Volume 4, Number 2, May 2022
Abstract:
The fully implantable intramedullary (IM) nailing system is an elegant solution in limb lengthening that has become incredibly popular among both surgeons and patients. The system was initially used for lower extremity lengthening; however, it has also been used for humeral lengthening. In this case report, we describe a very difficult course of a humeral lengthening with an intramedullary device. This case illustrates the importance of appropriate patient and implant selection. Despite advances in the field of limb lengthening, the potential for major complications of these procedures should not be underestimated.
Key Concepts:
- It is critical to ensure proper implant size with adequate inner and outer diameter of the bone.
- Excessive reaming can potentially lead to bone necrosis which decreases bone formation and increases risk for infection.
- When considering an IM implant for humeral lengthening, one must ensure that all factors are optimized or consider use of an external fixator.
- In cases where bone is needed for reconstruction, one could consider a suction device for harvesting autograft bone from the tibia.
Introduction
Indications for limb lengthening include functional impairment and cosmetic concerns.1 The technique of gradual distraction osteogenesis using circular external fixators described by Gavriil Ilizarov, MD, has evolved and now can be accomplished with fully implantable intramedullary nailing systems such as the PRECICE nail (NuVasive, Inc., San Diego, CA).1,2 Originally, this implant was designed for use in the lower extremity but has been utilized for the humerus as well. Compared to leg lengthening, arm lengthening is less common.
Limb lengthening surgery risks serious complications when performed at any site, including joint subluxation, fracture, and poor regeneration that can lead to delayed union or nonunion.2 Delayed union may respond to nonoperative management, but nonunion typically requires surgical intervention.2,3 Nonunion is usually a result of at least one of the following mechanisms: infection, mechanical failure, bone necrosis, or altered biologic healing processes.4 The surgical procedure of choice for treatment of nonunion depends on both the location and type but frequently requires bone grafting.3,5–8
Herein, we report a case of humeral lengthening with an IM device that resulted in an infected nonunion. Retrospective review demonstrates errors in preoperative planning and execution that likely contributed to this difficult course.
Case
Our patient was a 15-year-old female with a history of Russell-Silver syndrome, and as a result of her underlying pathology, she had both upper and lower limb length differences. She had undergone uncomplicated limb length equalization using an intramedullary lengthening device (PRECICE nail) of the left femur. The patient requested humeral lengthening to address her upper limb discrepancy.
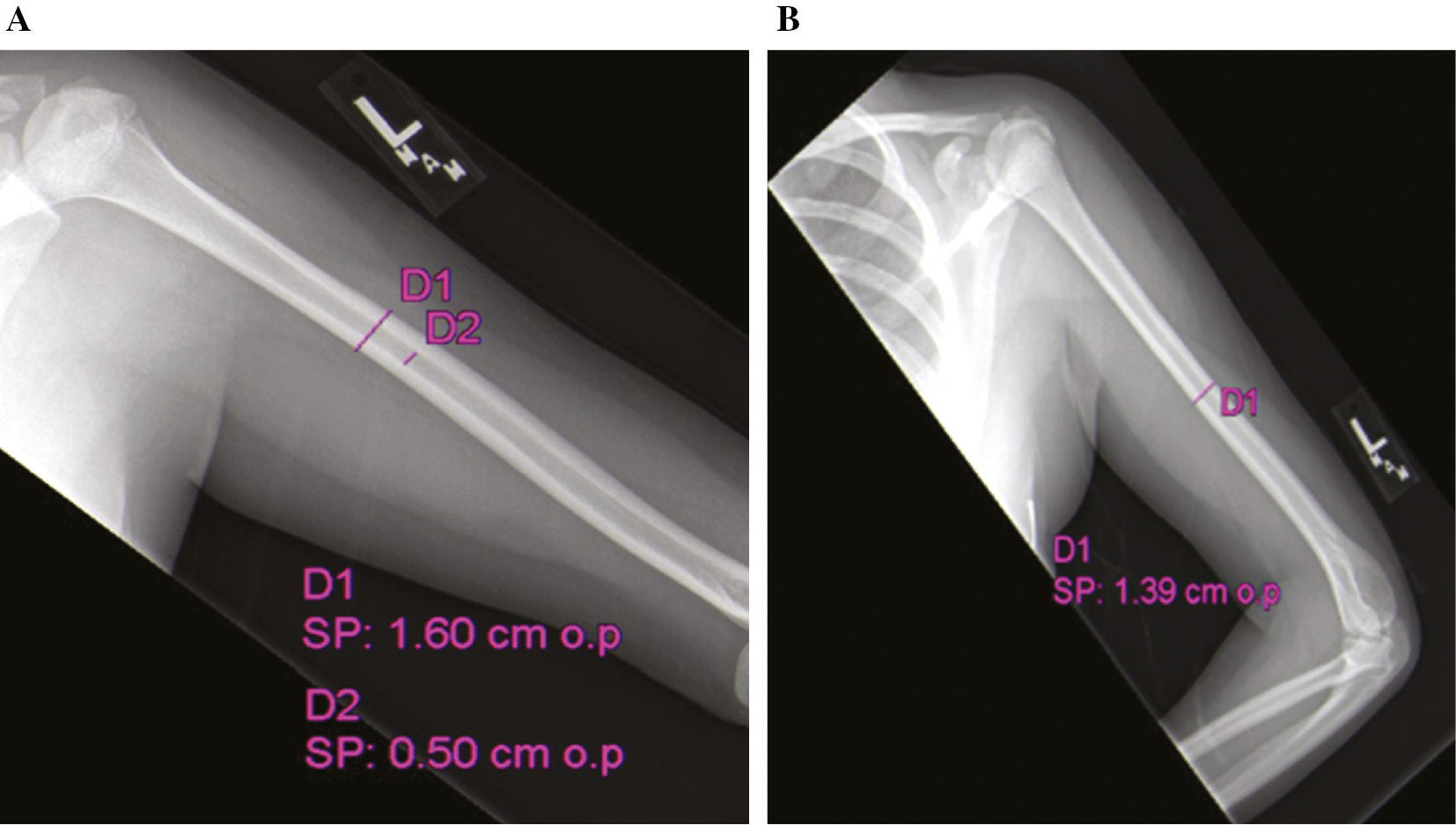
Radiographically, the patient’s intramedullary canal was 5 mm at the narrowest point (Figure 1A). The outside diameter of the humerus was 1.6 cm on the AP and 1.4 cm on the lateral (Figure 1A & B).
Figure 1. (A) AP and (B) lateral preoperative humeral canal measurements.
The humeral lengthening was planned with the anticipation of using an 8.5 mm diameter PRECICE tibial nail. After appropriate exposure and entry point was obtained, and ball tipped guide wire was passed, reaming was performed. A starting reamer was used and the bone was noted to be very difficult to ream. The osteotomy site was anticipated to be 12 cm proximal to the tip of the 180 mm nail. Multiple drill holes were made at the level of the planned osteotomy to vent reamings. We proceeded to ream up to 8.5 mm distally but noted a perforation in the cortex distally. The proximal segment was over-reamed to 11 mm. The osteotomy was completed using an osteotome to connect the drill holes, and the nail was advanced through the distal canal and seated in its final position. There was some difficulty advancing the nail to its final position due to lack of over-reaming. Proximal interlocks were placed using the guide and distal interlocks were placed using a freehand technique utilizing a small anterior incision to directly visualize the bone. The perforation was noted to be very close to the distal fixation and a decision was made to reinforce with a cerclage wire via the anterior incision (care was taken to ensure that no soft tissue was entrapped) (Figure 2). The postoperative course was complicated by partial radial nerve palsy, which resolved slowly over 10 months.
Figure 2. Postoperative Precice nail. Small medial fragment was noted at the osteotomy site which was slightly distracted.

Lengthening at 1 mm/day was initiated after 7 days of latency but was decreased to 0.66 mm/day after 7 days due to pain. At 4 weeks postoperatively, the patient developed mild erythema but no drainage and was felt to have a possible superficial infection that responded to a short course of clindamycin. She completed the desired 3 cm of lengthening. At 3 months postoperatively, she presented with erythema and induration. There was no significant bone regeneration noted in the distraction gap (Figure 3). She underwent debridement and irrigation and was found to have gross purulence as well as nonviable bone. She underwent removal of the implant and placement of an antibiotic nail. Cultures grew Staphylococcus capitis and Propionibacterium acnes. She subsequently underwent five additional debridements and prolonged IV antibiotic treatment. She had an attempt at reconstruction using allograft with some reconstitution of bone stock but incomplete healing resulting in an atrophic nonunion with an approximately 11 cm nonviable humeral segment (Figure 4A & B). A reconstructive procedure was planned to include use of bone autograft via a suction harvesting device.
Figure 3. AP radiograph at 3 months demonstrating minimal regenerate.

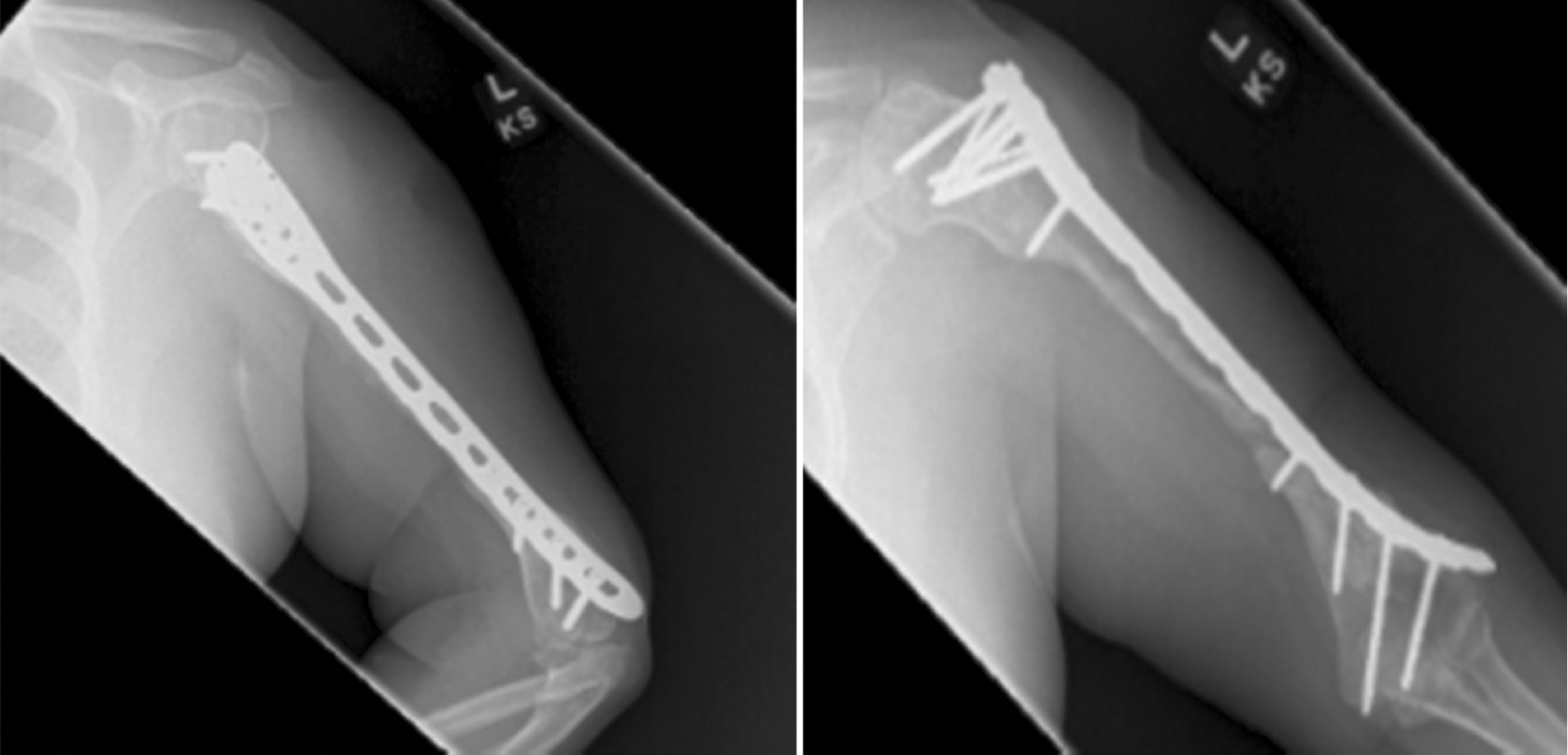
Figure 4. Atrophic nonunion with failure of proximal fixation, (A) AP, (B) lateral.

Brief Operative Description
After surgical exposure, fixation of the left humerus was achieved via a locking plate and screws. Following fixation, bone was harvested from the ipsilateral proximal tibial metaphysis (Figure 5) (Avitus® Bone Harvester, Avitus Orthopaedics, Inc., Farmington, CT). Via a 2 cm medial incision, an entry hole in the medial cortex was made to allow for manual suctioning and curettage. A total of 60 mL of cancellous bone was harvested by two suctioning rounds. The bone graft was mixed with 1 g of vancomycin powder and used to fill the humeral defect.
Figure 5. Autograft harvesting.

Postoperatively, the patient was allowed to bear weight as tolerated by her lower extremities and received instructions to limit weight bearing to her left humerus. One week after surgery, serous drainage was noted from her incision, which subsequently resolved after a 5-day course of doxycycline. She had regular follow-up and was thought to have bridging bone at 33 weeks (Figure 6).
Figure 6. Thirty-three weeks later there appeared to be bridging bone.
Implant removal was attempted 20 months post autograft, which resulted in re-fracture and subsequent re-plating (Figure 7).
Figure 7. Replating after fracture.

Follow up imaging 7 months after re-plating revealed a nonunion at the fracture site and broken distal screw. Treatment with a bone stimulator and high-dose vitamin D was attempted for 4 months but was unsuccessful. At 1-year follow-up, the patient complained of pain, limited range of motion with radiographic nonunion (Figure 8). There was no appreciable increase in lucency to cause concern for aggressive infection (Figure 8B).
Figure 8. (A) AP radiograph at 7 months after re-plating the defect was partially healed but construct failure was also noted. (B) Imaging at 12 months post re-plating demonstrating persistent nonunion and loose, broken distal screws.
Re-revision internal fixation and autologous bone grafting from the proximal ulna (we did not use prior graft technique as only a small amount was required) was subsequently performed (Figure 9A & B).
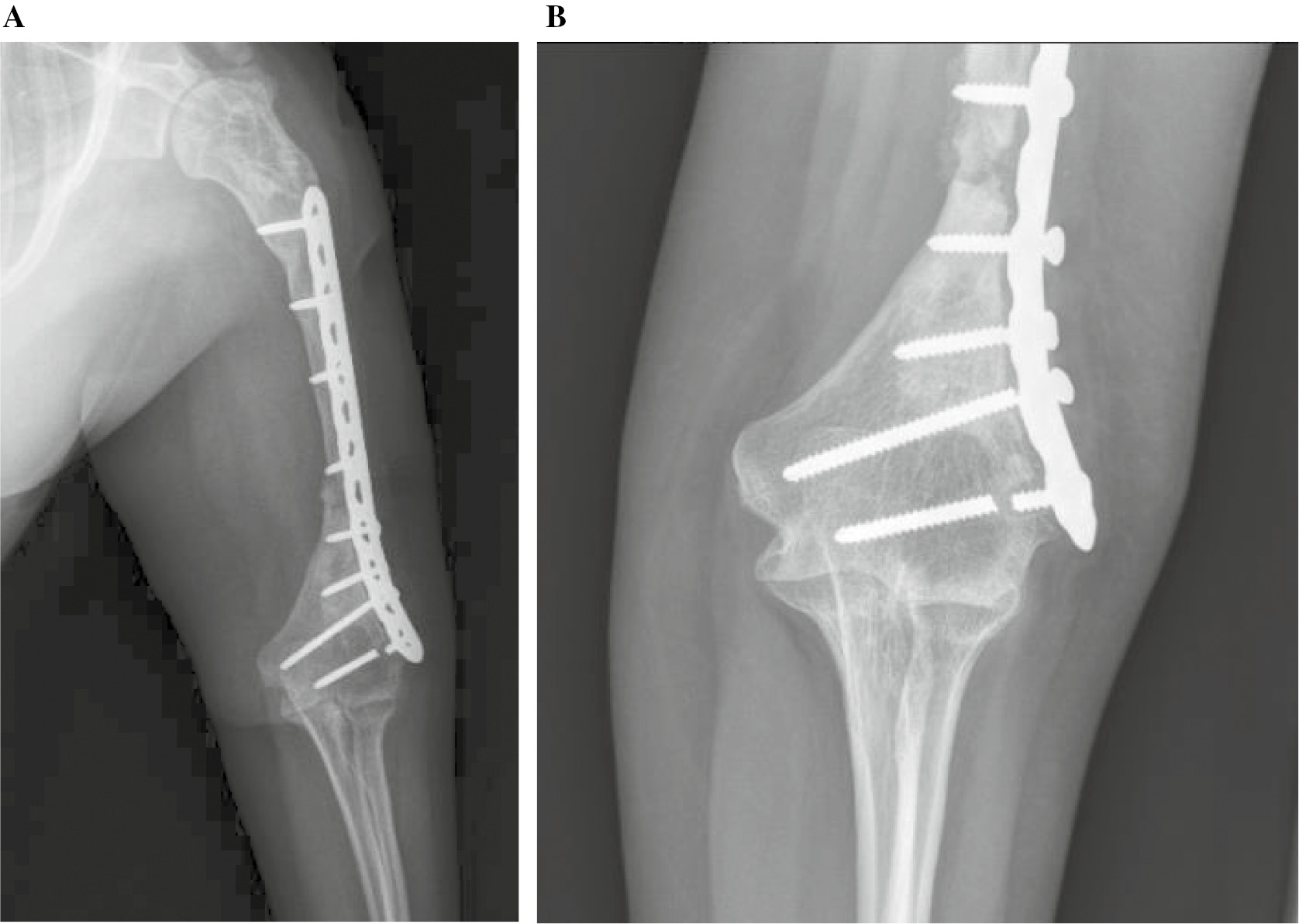
Figure 9. Most recent follow-up 1 month after re-revision for nonunion.

Discussion
We present a complex postsurgical course following an upper extremity limb lengthening procedure with an intramedullary implant. The case demonstrates poor initial bone formation that could have resulted from a variety of causes including thermal necrosis of the humerus when reaming, initial distraction at the osteotomy site, and low-grade infection. We wish to highlight 2 points from this difficult case.
With respect to the bone stock, the patient had a small humerus due to her underlying Russell-Silver syndrome.9 We failed to appreciate that her canal diameter was likely too narrow to accept the reaming required for nail insertion. The instructions for the PRECICE nail system indicate a need for 3 mm of cortical thickness surrounding the implant in addition to reaming 2 mm greater than the nail diameter.10 Therefore, for an 8.5 mm nail with 2 mm of reaming and 3 mm of cortex on both sides, the minimum outer diameter would need to be 16.5 mm. In our patient, the outer diameter was 16 mm on the AP but only 14 mm on the lateral. Additionally, the inner diameter was quite small (5 mm), necessitating extensive reaming. Excessive reaming disrupts the endosteal blood supply and may also lead to thermal injury.11 The inability to over ream the distal segment may have also led to distraction at the osteotomy site. The initial distraction in combination with extensive devitalization of the diaphysis of the humerus likely lead to nonunion and infection. While it is common and often necessary to perform “off label” use of implants in pediatric settings due to limited availability of appropriately sized implants, care must be taken to recognize limitations and respect biology.
Secondly, the presence of infection and extent of devitalization was incompletely appreciated. More prompt recognition of deep infection may have shortened the duration of interventions for this patient. In addition, more extensive initial debridements may have hastened eradication of infection. We were conservative in our debridement’s in order to avoid unnecessary bone loss, but ultimately the patient had a large segmental defect that was arrived at piecemeal over many procedures.
We wish to highlight the option of an additional method for obtaining autogenous cancellous bone using a vacuum-assisted system. The vacuum-assisted harvest method through a small incision over the tibia is an option that is relatively quick with limited blood loss. We harvested 60 mL of cancellous bone in 10 minutes with blood loss of 5 mL. Reamer-irrigator-aspirator (RIA) systems can be utilized, but yield may be lower in small femurs and complications like bleeding and fractures remain of significant concern.12–14 Merchand et al. compared blood loss with other methods of bone graft harvesting and found the average blood loss was 255 mL for iliac crest bone graft (ICBG) and 674 mL with RIA, and transfusions were required in 21% of the ICBG cohort and 44% of the RIA group.14 No fractures have been reported with the Avitus device to date.15–17
In conclusion, we present a difficult case that resulted from poor implant selection for the patient’s bone size and incomplete recognition and bony debridement of infection. We wish to highlight the need for careful consideration of reaming diameter to avoid thermal necrosis when utilizing intramedullary lengthening implants and to reiterate that the potential for complications in lengthening procedures should never be underestimated.
Additional Links
- POSNAcademy: Magnetic, Motorized Femoral Lengthening Nail: Antegrade Piriformis, John E. Herzenberg, MD, FRCSC—https://bit.ly/3ui60Iv
- POSNAcademy: How to Insert a Precice Tibial Nail, Christopher A. Iobst, MD—https://bit.ly/36FN9yT
Disclaimer
No funding was received. The authors have no conflicts of interest to disclose.
References
- Fürmetz J, Kold S, Schuster N, et al. Lengthening of the humerus with intramedullary lengthening nails-preliminary report. Strateg Trauma Limb Reconstr. 2017;12(2):99-106. doi: https://doi.org/10.1007/s11751-017-0286-6.
- Morrison S, Dahl M, Georgiadis A. Motorized internal limb lengthening: an updated review. JPOSNA. 2020;2(1). Available at: https://www.jposna.org/ojs/index.php/jposna/article/view/67.
- Kanakaris NK, Tosounidis TH, Giannoudis PV. Surgical management of infected non-unions: an update. Injury. 2015;46 Suppl 5:S25-S32. doi: https://doi.org/10.1016/j.injury.2015.08.009.
- Simpson A, Robiati L, Jalal MMK, et al. Non-union: indications for external fixation. Injury. 2019;50 Suppl 1:S73-S78. doi: https://doi.org/10.1016/j.injury.2019.03.053.
- Frölke JP, Patka P. Definition and classification of fracture non-unions. Injury. 2007;38 Suppl 2:S19-S22. doi: https://doi.org/10.1016/s0020-1383(07)80005-2.
- Rupp M, Biehl C, Budak M, et al. Diaphyseal long bone nonunions - types, aetiology, economics, and treatment recommendations. Int Orthop. 2018;42(2):247–258. doi: https://doi.org/10.1007/s00264-017-3734-5.
- Dekker TJ, White P, Adams SB. Efficacy of a cellular bone allograft for foot and ankle arthrodesis and revision nonunion procedures. Foot Ankle Int. 2017;38(3):277-282. doi: https://doi.org/10.1177/1071100716674977.
- Calori GM, Colombo M, Mazza EL, et al. Incidence of donor site morbidity following harvesting from iliac crest or RIA graft. Injury. 2014;45 Suppl 6:S116-S120. doi: https://doi.org/10.1016/j.injury.2014.10.034.
- Goldman V, McCoy TH, Harbison MD, et al. Limb lengthening in children with Russell-Silver syndrome: a comparison to other etiologies. J Child Orthop. 2013;7(2):151-156. doi: https://doi.org/10.1007/s11832-012-0474-3.
- NuVasive. Precice System Instructions for Use 2021. Available at: https://atlasapi.nuvasive.com/public/ifu/documents/retrieve?get&pVersion=0046&contRep=ZNUVEP1&docId=0050568677011EDB9CDF0046DC5EA12A&compId=LC0046-AD_ENGLISH.pdf.
- Bhandari M, Guyatt G, Tornetta P, 3rd, et al. Study to prospectively evaluate reamed intramedually nails in patients with tibial fractures (S.P.R.I.N.T.): study rationale and design. BMC Musculoskelet Disord. 2008;9:91. doi: https://doi.org/10.1186/1471-2474-9-91.
- Peters RM, Claessen FM, Doornberg JN, et al. Union rate after operative treatment of humeral shaft nonunion--a systematic review. Injury. 2015;46(12):2314-2324. doi: https://doi.org/10.1016/j.injury.2015.09.041.
- Madison RD, Nowotarski PJ. The reamer-irrigator-aspirator in nonunion surgery. Orthop Clin North Am. 2019;50(3):297-304. doi: https://doi.org/10.1016/j.ocl.2019.03.001.
- Marchand LS, Rothberg DL, Kubiak EN, et al. Is this autograft worth it?: The blood loss and transfusion rates associated with reamer irrigator aspirator bone graft harvest. J Orthop Trauma. 2017;31(4):205-209. doi: https://doi.org/10.1097/bot.0000000000000811.
- Lowe JA, Della Rocca GJ, Murtha Y, et al. Complications associated with negative pressure reaming for harvesting autologous bone graft: a case series. J Orthop Trauma. 2010;24(1):46-52. doi: https://doi.org/10.1097/BOT.0b013e31819c0ccb.
- Bagi P, Walls R. Novel, vacuum-assisted method for harvesting autogenous cancellous bone graft and bone marrow from the proximal tibial metaphysis. Foot Ankle Orthop. 2018;3(3):2473011418S2473000149. doi: https://doi.org/10.1177/2473011418S00149. Accessed November 04, 2021.
- Orthopaedics A. Avitus Orthopaedics Library. Available at: https://avitusortho.com/library. Accessed November, 2021.