
Original Research
Decreasing Rate of Operative Management of Proximal Humerus Fractures in Adolescents: A National Database Study
Department of Orthopaedic Surgery, University of California San Francisco, San Francisco, CA
Correspondence: Ishaan Swarup, MD, University of California, San Francisco, 747 52nd St., OPC First Floor, Oakland, CA 94609. E-mail: [email protected]
Received: February 13, 2022; Accepted: May 2, 2022; Published: August 1, 2022
DOI: 10.55275/JPOSNA-2022-0047
Volume 4, Number 3, August 2022
Abstract:
Background: There is no consensus on the operative treatment of adolescent proximal humerus fractures. The purpose of this study was to investigate the trends in treatment of proximal humerus fractures in adolescents and identify predictors of operative management.
Methods: The Pediatric Health Information System database was used to identify patients ages 10 to 18 diagnosed with proximal humerus fractures between 2004 to 2019. Open fractures were excluded from the analysis. Descriptive, univariate, and multivariate analyses were used to determine trends and predictors of operative management.
Results: A total of 17,515 proximal humerus fracture admissions were identified and 2081 (11.9%) were treated operatively. The mean age was 12.5 years and 37.5% of patients were female. The rate of operative management decreased from 15.1% to 8.9% during the study period (p<0.01). There was a higher rate of operative management in boys (13.4% vs. 9.4%, p< 0.01). The operative cohort was older (13.4 years vs. 12.4 years, p<0.01), and patients who lived in rural areas had twice the rate of operative management (20.7% vs. 10.8%, p<0.01). Operative patients had higher billed charges and longer hospital stay (p < 0.05), but there was no significant difference in mean estimated household income between operative and nonoperative groups (p > 0.05). A multivariate analysis showed increased odds of operative management with older age (OR 1.32, 1.29-1.36) and residence in the South (OR 1.19, 1.05-1.34). The odds of operative management were lower in more recent years (OR 0.94, 0.93-0.95) and in urban settings (OR 0.41, 0.35-0.47).
Conclusion: From 2004 to 2019, there has been a significant decrease in the rate of operative management of adolescent proximal humerus fractures at children’s hospitals. Patients who are older, male, or reside in rural areas or the South are more likely to be treated operatively.
Level of Evidence: Level IV
Key Concepts:
- There has been a decreasing rate of operative management of adolescent proximal humerus fractures at children’s hospitals.
- Younger (10 to 13 years) and older (14 to 18 years) adolescents are distinct surgical populations, with older adolescents having over twice the rate of operative management.
- Management of adolescent proximal humerus fractures is largely dependent on the practice setting, with patients in rural settings and the South more likely to receive operative treatment.
Introduction
Proximal humerus fractures account for 0.45-5.4% of all pediatric fractures.1–3 Nonoperative management of these injuries has generally yielded excellent radiographic and clinical outcomes as the majority (85%) of these fractures are non or minimally displaced.3–8 Furthermore, the proximal humerus epiphysis is responsible for 80% of humeral growth, and therefore, has considerable remodeling potential.1 Due to these reasons, the current orthopaedic literature has largely advocated for nonoperative management of these injuries in the pediatric population.5
However, the management of these injuries in adolescent patients is more controversial due to the decreased remodeling potential in this age group. It has been recommended to treat children under 10 and over 13 as distinct patient populations, as their prognosis is likely to be different due to the closure of the proximal humeral physis.5,9 There are significantly higher rates of operative management in adolescents compared to younger children10 and good outcomes have been reported with operative management in older children.6,11,12 In adults, there has been an increasing trend toward operative management of these fractures.13–14 There has also been an increase in the rates of operative fixation for other adolescent fractures such as tibia shaft and clavicle fractures.15–17 However, there are very few studies that have assessed trends in the rate of operative management of proximal humerus fractures specifically in adolescents. The purpose of this study was to investigate recent trends in the management of proximal humerus fractures in adolescents and to investigate predictors of operative management using a large national database.
Materials and Methods
We performed a retrospective study using the Pediatric Health Information System (PHIS). PHIS is a database that includes clinical and resource utilization data across inpatient, ambulatory, and emergency department encounters from 52 children’s hospitals in the United States. This study included patients between the ages of 10 to 18 who sustained a proximal humerus fracture between 2004 to 2019. International Classification of Disease, 9th and 10th Revisions (ICD-9 and ICD-10) codes were used to identify proximal humerus fractures. Patients with open fractures were excluded from the analysis. We specifically collected data on patient demographics and details relating to management of the injury. The primary outcome of interest was rate of operative management, and this rate was analyzed for each year as well as trended over time. Secondary outcomes of interest included factors associated with operative management of this injury.
Statistical Analysis
Descriptive statistics were used to summarize the data. Student t-test and Chi-square analyses were performed on continuous and categorical values, respectively. The rate of operative treatment was calculated by year of treatment and by patient age. Multivariable analysis was performed using a binary logistic regression model to identify factors associated with operative management. All statistical analyses were performed using R statistical software (Version 4.0.2).
Results
Cumulative Data
This study included 17,515 pediatric admissions with a primary diagnosis of proximal humerus fracture (Table 1). In this cohort, 2082 fractures were treated operatively (11.9%) and 15433 fractures (88.1%) were treated nonoperatively. The mean age of patients was 12.5 years and 37.5% of patients were female. Subgroup analyses was performed by age with younger adolescents ages 10 to 13 (12271 patients, 70.0%) and older adolescents ages 14 to 18 (5244 patients, 30.0%). Patients age 14 and under compromised 84.4% of the data. The majority (90.9%) of the study data was from institutions in urban settings as defined by the United States Census Bureau. There was insufficient data to study the effect of race, ethnicity, and insurance status on the rate of operative treatment.
Table 1. Demographic Data of Adolescent Proximal Humerus Admissions
| Total | Nonoperative | Operative | p | |
|---|---|---|---|---|
| N | 17515 | 15433 (88.1%) | 2082 (11.9%) | |
| Mean Age (SD) | 12.54 (1.87) | 12.42 (1.86) | 13.44 (1.72) | <0.001 |
| Female | 6574 (37.5%) | 5956 | 618 (9.4%) | <0.001 |
| Male | 10939 (62.5%) | 9475 | 1464 (13.4%) | |
| Urban | 15539 (90.9%) | 13856 | 1683 (10.8%) | <0.001 |
| Rural | 1559 (9.1%) | 1236 | 323 (20.7%) | |
| Midwest | 4528 | 4018 | 510 (88.7%) | - |
| Northeast | 3036 | 2668 | 368 (87.9%) | 0.27 |
| South | 5777 | 5038 | 739 (87.2%) | 0.01 |
| West | 4174 | 3709 | 465 (88.9%) | 0.88 |
| Mean Income (SD) | 49333 (20877) | 48517 (22260) | 0.11 | |
| Mean Estimated Cost (SD) | 654 (2550) | 7453 (7531) | <0.001 | |
| Mean Billed Charges (SD) | 1760 (5279) | 22046 (23175) | <0.001 | |
| Mean Length of Stay (SD) | 1.07 (1.19) | 1.42 (1.64) | <0.001 |
SD=standard deviation.
Of the operatively treated patients, there were 1596 admissions that could be clearly identified and either open or closed reduction based on coding. There were 693 (43.4%) open reductions, and this cohort was significantly older than the closed reduction cohort (13.7 years vs. 13.3 years, p< 0.01). There was no difference in urban hospitals or gender between the cohorts.
Rates of Operative Management
The rates of operative treatment were examined by patient age and treatment year (Figures 1 and 2). The rates of operative management decreased from 15.1% in 2004-2008 to 8.9% in 2015-2019 (p<0.01). There was a higher rate of operative management in boys compared to girls (13.4% vs. 9.4%, p< 0.01). Additionally, the operative cohort was older than the nonoperative cohort (13.4 years vs. 12.4 years, p< 0.01), and the rate of operative management in patients who were treated in rural areas was twice as high as patients who were treated at urban hospitals (20.7% vs. 10.8%, p< 0.01). Older adolescents had twice the rate of operative management compared to younger adolescents (19.8% vs. 8.5%, p<0.01).
Figure 1. Operative vs. Nonoperative Treatment by Age.
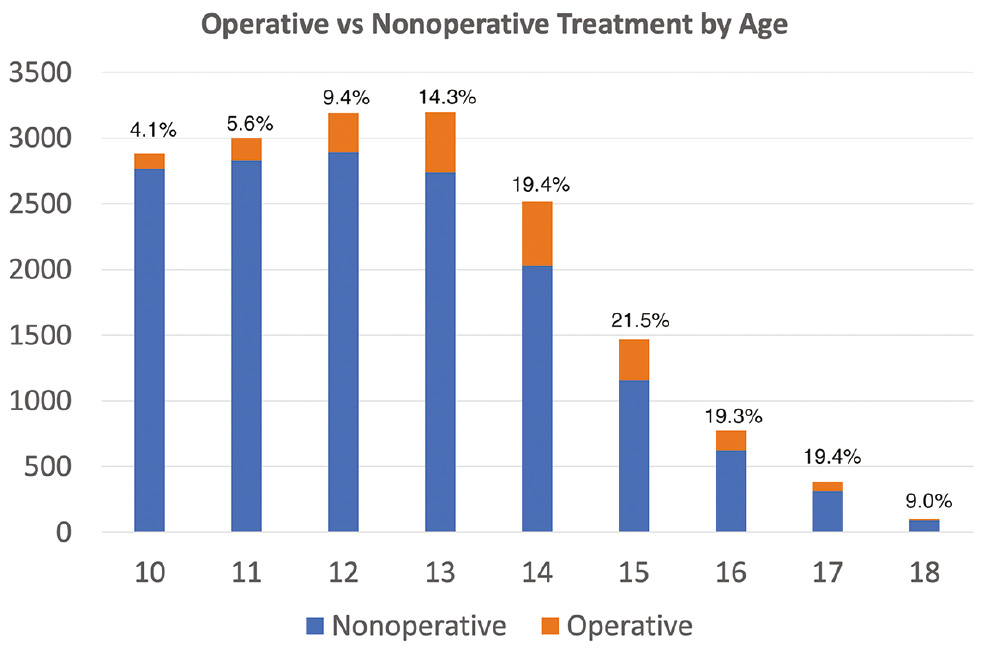
Figure 2. Rate of Operative Treatment by Year.

Operative patients had higher billed charges ($22046.33 vs. $1760.12, p< 0.01) and longer hospital length of stay (1.42 days vs. 1.07 days, p < 0.01), but there was no significant difference between the two groups in mean estimated household income, which was estimated by zip code of residence (p> 0.05).
Predictors of Operative Management
A multivariate analysis showed increased odds of operative management with older age (OR 1.32, p<0.01) and treatment in the South as defined by the United States Census Bureau (OR 1.19, p=0.01) (Table 2). Male gender was not identified as an independent predictor of operative management in the multivariate analysis (OR 1.08, p> 0.05). The odds of operative management were lower in more recent years (OR 0.94, p< 0.01) and in urban hospitals (OR 0.41, p< 0.01). There was a statistically significant effect of higher estimated household income on the likelihood of operative management, but the effect size was very small (OR 1.003, p< 0.01).
Table 2. Predictive Factors of Operative Management
| Odds Ratio | 95% CI | p | |
|---|---|---|---|
| Age | 1.32 | 1.29-1.36 | <0.001 |
| Male | 1.08 | 0.97-1.20 | |
| Year | 0.94 | 0.93-0.95 | <0.001 |
| Region | 0.01 | ||
| Midwest | 1 | ||
| Northeast | 1.09 | 0.94-1.26 | |
| South | 1.19 | 1.05-1.34 | |
| West | 1.02 | 0.89-1.18 | |
| Urban | 0.41 | 0.35-0.47 | <0.001 |
| Income | 1.00 | 1.00-1.00 | <0.001 |
Discussion
The purpose of this study was to investigate recent trends in the management of proximal humerus fractures in adolescents as well as to identify predictors of operative management. Trends in the treatment of pediatric proximal humerus fractures have varied greatly over time. The orthopaedic literature from 1965 to 1990 uniformly recommended nonoperative management, whereas studies in the 2000s recommended surgery for displaced fractures, particularly in older children.5 This study showed that from 2004 to 2019, the overall rate of surgical management was 11.9%. This rate is comparable to studies that cite 8-17.3% for all pediatric proximal humerus fractures, though lower than reported rates of 20% in adolescents.1,8,10 Subgroup analyses demonstrated that younger (10 to 13) and older (14 to 18) adolescents were indeed distinct surgical populations, with older adolescents having over twice the rate of operative management (19.4%). Although in our data set, the oldest cohort (age 18) had the lowest rate of operative management (9.0%), this is likely an outlier as only 100 patients were included in this age group. We anticipate that 18-year-olds are likely treated, and operated on, at adult hospitals with higher frequency.
A recent database study by Cruz et al. showed that 43.2% of pediatric humerus fractures were treated operatively.18 However, admission to a children’s hospital was associated with lower rates of operative management. Our study included data exclusively from children’s hospitals as well as more recent data, and these important differences may help to explain the lower operative rates observed in this study. Overall, additional research is needed to understand variations in management and ensure appropriate management of proximal humerus fractures in adolescents.
In this study, we also noted a decreasing trend in operative management over time. For instance, the rate of operative management of proximal humerus fractures in adolescents decreased from 15.1% in 2004-2008 to 8.9% in 2015-2019. In comparison, Cruz et al. showed an increasing trend in operative management from 39.4% in 2000 to 46.3% in 2012. However, their data included all hospitals in the United States and did not include any data beyond 2012. It is unclear why operative rates have decreased over time, but it may be related to changes in practice. Specifically, there have been a number of recent publications since Cruz’s study showing excellent nonoperative results that may have shifted practice in children’s hospitals. For example, Binder et al. showed that 96.9% of patients treated nonoperatively had excellent results with significantly poorer results in the surgical group.1 Chaus et al. showed that there was no difference in complications, rate of return to activity, or cosmetic satisfaction in operative and nonoperative matched cohorts and that functional outcomes tended to be higher in the nonoperative cohort.19 While older age has been cited as a reason for operative treatment, Wei et al. compared patients under 11 to patients 11 and older with displaced proximal humerus fractures treated with conservative management. They showed no significant difference in malreduction or Constant scores at 2 years in both, suggesting that nonoperative management may be appropriate in adolescent patients.20 Lastly, another consideration is the cost of operative treatment. Our study showed that operative treatment had a 12.5 times higher billed cost ($22046) compared to nonoperative treatment ($1760), and this information should be offered during shared decision-making.
Perhaps the most critical decision for a surgeon is when to operate. There is no accepted absolute indication for surgery, but Neer-Horwitz Grade III or IV displacement and greater than 30 degrees angulation in children 10 or older have been suggested as general guidelines.9,18 In girls under 13 and boys under 15, 50% of bayonet apposition and up to 20 degrees of angulation in any plane were noted to remodel.21 There are variable indications for operative management in the literature based on degree of translation, angulation, and by age, which is confusing to clinicians.22 Shoulder fracture-dislocations are rare in pediatric patients but may be an absolute indication to surgical management.23 Moreover, surgical management is usually recommended when closed reduction is unsatisfactory due to interposed long head of the biceps tendon, deltoid muscle, comminution, periosteum, or capsule,6,10,21 and recently, there has been renewed interest in describing surgical techniques.24 Displaced fractures treated operatively have shown good functional and radiographic outcomes in smaller retrospective studies.11,12,25 Wang et al. studied a cohort of 37 children treated surgically for severely displaced proximal humerus fractures. There were no complications and all patients were satisfied or very satisfied.26 In general, studies on operative treatment of pediatric or adolescent proximal humerus fractures have been retrospective and smaller in nature and thus do not provide robust data on operative outcomes.
Proximal humerus fractures are more common in male adolescents who are more likely to be treated operatively, although gender was not identified as an independent predictor of surgery. Our analysis identified older age, income, and residence in rural settings or the South as predictive factors of operative management. Interestingly, where the patient is treated seems to affect whether the patient is treated operatively, and geographic differences have been noted in the management of other medical and surgical conditions.27–29 Similarly, Cruz et al. demonstrated admission to a non-children’s hospital was associated with increased operative rates (45% compared to 29%) which underscores variations in practice and experience with management of pediatric proximal humerus fracture.18 Overall, the results from this study and previous studies show that the treatment algorithm for adolescent proximal humerus fractures is not uniform across practice settings, and additional research is needed to explore variations in practice and further define indications. Ultimately, prospective studies and evidence-based guidelines are needed to guide clinical decision-making.
Strengths of this study include its large sample size and data from multiple hospitals across all regions of the United States. Our study builds upon prior meta-analyses and database studies to describe updated trends in the management of proximal humerus fractures. Our study also focuses on adolescent patients, which is a population that has not been extensively studied. However, this study has several limitations including the fact that the majority of our data comes from urban children’s hospitals and may not represent practice in rural areas. Our sample is also skewed towards younger adolescents with 84.4% of the data coming from patients 14 and under. Therefore, the age difference between operative and nonoperative patients is smaller than expected, and thus our subgroup analyses is a more useful illustration of the age-dependent nature of the operative indication in proximal humerus fractures. Furthermore, as a database study, our data is limited by coding misclassification and inability to extract further clinical information such as fracture displacement and morphology. The study is also limited by lack of outcome data and we are unable to describe the effect of operative trends on patient outcomes. Future studies are needed to validate these results as well as provide additional insight on the effect of clinical factors on management and outcomes after surgical and nonsurgical management.
In conclusion, approximately 10% of proximal humerus fractures in adolescents are treated operatively, but younger and older adolescents are distinct populations with children 14 and older having twice the rate of operative management. More recently, there has been a trend toward nonoperative management of these injuries at children’s hospitals. Patients who are older, male, or who are treated in rural areas are significantly more likely to receive operative treatment. Further study is needed to investigate temporal trends and geographic differences in practice, as well as identify differences in patient outcomes between operative and nonoperative management of adolescent proximal humerus fractures.
Additional Links
- POSNAcademy: Proximal Humerus Fractures: Should We Operate or Not?, Donald S. Bae, MD, Boston Children’s Hospital
- POSNAcademy: Reduction & Fixation of Proximal Humerus Fracture, Donald S. Bae, MD, Boston Children’s Hospital
Disclaimer
No funding was received for this study. The authors have no conflicts of interest to report.
References
- Binder H, Tiefenboeck TM, Payr S, et al. Treatment of proximal humerus fractures in children and young adolescents. Wien Klin Wochenschr. 2016;128:120–124.
- Jin S, Cai H, Xu Y. Shoulder dislocation combined with proximal humerus fracture in children. Medicine. 2017;96(48):e8977.
- Shrader MW. Proximal humerus and humeral shaft fractures in children. Hand Clin. 2007;23(4):431-435.
- Fernandez FF, Eberhardt O, Langendörfer M, et al. Treatment of severely displaced proximal humeral fractures in children with retrograde elastic stable intramedullary nailing. Injury. 2008;39:1453-1459.
- Pahlavan S, Baldwin KD, Pandya NK, et al. Proximal humerus fractures in the pediatric population: a systematic review. J Child Orthop. 2011;5:187-194.
- Bahrs C, Zipplies S, Ochs BG, et al. Proximal humeral fractures in children and adolescents. J Pediatr Orthop. 2009;29(3):238-242.
- David S, Kuhn C, Ekkernkamp A. Fracture of the proximal humerus in children and adolescents. The most overtreated fracture. Der Chirug. 2006;77:827-834.
- Di Gennaro GL, Spina M, Lampasi M, et al. Fractures of the proximal humerus in children. Chir Organi Mov. 2008;92(2):89-95.
- Popkin CA, Levine WN, Ahmad CS. Evaluation and management of pediatric proximal humerus fractures. J Am Acad Orthop Surg. 2015;23:77-86.
- Hannonen J, Hyvönen H, Korhonen L, et al. The incidence and treatment trends of pediatric proximal humerus fractures. BMC Musculoskelet Disord. 2019;20(1):571.
- Khan A, Athlani L, Rousset M, et al. Functional results of displaced proximal humerus fractures in children treated by elastic stable intramedullary nail. Eur J Orthop Surg Traumatol. 2014;24(2):165-172.
- Canavese F, Athlani L, Marengo L, et al. Evaluation of upper-extremity function following surgical treatment of displaced proximal humerus fractures in children. J Pediatr Orthop B. 2014;23(2):144-149.
- Sabesan VJ, Lombardo D, Petersen-Fitts G, et al. National trends in proximal humerus fracture treatment patterns. Aging Clin Exp Res. 2017;29(6):1277-1283.
- Schairer WW, Nwachukwu BU, Lyman S, et al. Arthroplasty treatment of proximal humerus fractures: 14-year trends in the United States. Phys Sportsmed. 2017;45(2):92-96.
- Essilfie A, Sabour A, Hatch GF, et al. An increasing rate of surgical management of closed tibia fractures in an adolescent population: a national database study. J Am Acad Orthop Surg. 2019;27(21):816-822.
- Raducha JE, Swarup I, Schachne J, et al. Tibial shaft fractures in children and adolescents. JBJS Rev. 2019;7(2):e4.
- Yang S, Werner BC, Gwathmey FW. Treatment trends in adolescent clavicle fractures. J Pediatr Orthop. 2015;35(3):229-233.
- Cruz AI, Kleiner JE, Gil JA, et al. Inpatient surgical treatment of paediatric proximal humerus fractures between 2000 and 2012. J Child Orthop. 2018;12:1111-116.
- Chaus GW, Carry PM, Pishkenari AK, et al. Operative versus nonoperative treatment of displaced proximal humeral physeal fractures: a matched cohort. J Pediatr Orthop. 2015;35(3):234-9.
- Wei SW, Shi ZY, Zhao YM, et al. Comparison of conservative treatment outcomes for proximal humeral epiphyseal fractures in patients of different ages. Orthopade. 2019;48(2):119-124.
- Pandya NK, Behrends D, Hosalkar HS. Open reduction of proximal humerus fractures in the adolescent population. J Child Orthop. 2012;6:111-118.
- Kim AE, Chi H, Swarup I. Proximal humerus fractures in the pediatric population. Curr Rev Musculoskelet Med. 2021;14:413-420.
- Nelson G, Brown C, Liu RW. No incidence of glenohumeral joint dislocation in a review of 220 paediatric proximal humerus fractures. J Child Orthop. 2018;12:493-496.
- Swarup I, Hughes MS, Bram JT, et al. Percutaneous pinning of pediatric proximal humeral fractures. JBJS Essent Surg Tech. 2019;9(4):e33.1-6.
- Schwendenwein E, Hajdu S, Gaebler C, et al. Displaced fractures of the proximal humerus in children require open/closed reduction and internal fixation. Eur J Pediatr Surg. 2004;14(1):51-55.
- Wang X, Shao J, Yang X. Closed/open reduction and titanium elastic nails for severely displaced proximal humeral fractures in children. Int Orthop. 2014;38(1):107-110.
- Anders M, Mutty C, Cornwall A. Geographic variation in fasciotomy during operative management of tibia fractures. J Orthop. 2015;13(3):225-229.
- Azad TD, Vail D, O’Connell CO, et al. Geographic variation in the surgical management of lumbar spondylolisthesis: characterizing practice patterns and outcomes. Spine J. 2018;18(12):2232-2238.
- Floyd SB, Campbell J, Chapman CG, et al. Geographic variation in the treatment of proximal humerus fracture: an update on surgery rates and treatment consensus. J Orthop Surg Res. 2019;14(1):22.