
Original Research
Navicular Stress Fractures in Adolescent Athletes: Injury Characteristics and Outcomes of Surgical Fixation
Children’s Healthcare of Atlanta, Atlanta, GA
Correspondence: Crystal A. Perkins, MD, Children’s Healthcare of Atlanta, 5445 Meridian Mark Road, Suite 250, Atlanta, GA 30342. E-mail: [email protected]
Received: January 6, 2022; Accepted: February 21, 2022; Published: May 1, 2022
DOI: 10.55275/JPOSNA-2022-0022
Volume 4, Number 2, May 2022
Abstract:
Background: Surgical treatment of navicular stress fractures (NSF) in athletes has been recommended secondary to the poor blood supply of the navicular and frequency of delayed union and refracture. Regardless of treatment, nonunion and persistent pain are complications described in adults. The purpose of this study was to describe patient and fracture characteristics and outcomes of surgical treatment of NSF in adolescents.
Methods: An IRB approved retrospective review was performed of patients less than 18 years of age treated with surgical screw fixation of NSF from 2014-2019. All patients were contacted for collection of patient-reported outcome measures (PROMs).
Results: Five patients with a median age of 15.8 years (range 14–17 years) were included. Three patients, all baseball catchers, had a dorsal navicular osteophyte. All fractures were in the lateral third of the navicular. There were three type II fractures and two type III fractures. Median clinical follow-up was 7.1 months (range 5-14 months). No patient developed avascular necrosis. PROMs at a median of 61 months following surgery demonstrated that all patients returned to their primary sport at the same level and no patients reported refracture or subsequent surgeries.
Conclusions: In a cohort of adolescent patients, operative fixation of type II and III NSF results in reliable healing, no evidence of avascular necrosis (AVN), and excellent mid-term outcomes with full return to pre-injury level of sports. These outcomes are in contrast to higher rates of non-union and inability to return to sports reported in the adult literature.
Level of Evidence: IV
Key Concepts:
- A high index of suspicion for navicular stress fractures is required for prompt diagnosis and treatment.
- Advanced axial imaging, including CT and/or MRI, can be diagnostic of navicular stress fractures despite normal radiographs.
- Operative treatment of type II and III navicular stress fractures in adolescent athletes results in excellent mid-term outcomes.
Background
The tarsal navicular is a critical structure in the midfoot and has been described as an anatomical keystone in the formation of the medial longitudinal arch of the foot.1 The interplay of the tarsonavicular and talocalcaneonavicular joints are vital to the efficiency of gait, and thus injuries to the navicular, while rare, can have significant short- and long-term consequences.2 Navicular fractures occur most commonly as acute traumatic injuries or as a result of overuse. Sangerozan et al. classified navicular fractures into four categories based on anatomic location: tuberosity, body, capsular avulsion, and stress fractures.3
Navicular stress fractures (NSF) occur due to overuse and can present diagnostic and treatment challenges.4 Anatomic factors, including an elongated second metatarsal, metatarsal adduction, pes cavus, and equinus contractures, can all increase the load through the midfoot and make patients more susceptible to these injuries.5 The diagnosis of a navicular stress fracture can be difficult and is often delayed due to the insidious onset and non-specific symptomatology. Patients can report tenderness over the dorsal navicular prominence and have pain while standing, running, or jumping on the affected foot.6 Foot radiographs are often normal and confirmation of a stress fracture may require advanced imaging with computed tomography (CT) or magnetic resonance imaging (MRI).7
The management of navicular stress fractures remains controversial. Both nonoperative and operative interventions have been employed without well-defined guidelines to dictate treatment. In an attempt to decrease time to return to sport, early surgical intervention with screw fixation has been proposed with mixed results.8–11 Individual studies have reported quicker return to sport, but no significant differences are noted in meta-analyses.8,9 In addition, operative intervention inherently carries risks and can even cause delayed return to activity if hardware is removed.10 Regardless of treatment, fracture nonunion, persistent pain, and the development of talonavicular arthritis are described complications in the adult literature.11
The purpose of this study was to describe patient and fracture characteristics and outcomes of surgical treatment of NSF in adolescents. We hypothesized that in the active adolescent population, NSFs could be treated surgically with screw fixation with good functional results and minimal complications.
Methods
Patients between the ages of 12-18 who underwent operative fixation of a tarsal navicular stress fracture between January 1, 2010, through March 1, 2020, were identified by search of billing records for CPT code 28465 (open treatment of tarsal bone fracture). After Institutional Review Board approval, the study consisted of both a retrospective review and a follow-up survey of patients from a single pediatric hospital in a large urban area. Demographic information, including age at the time of surgery, sex, height, weight, race, sport participation, imaging, and treatment were collected. Patients undergoing fixation for acute traumatic navicular or other midfoot fractures were excluded.
Preoperative and postoperative imaging was reviewed for all patients by three independent observers. Any differences in radiographic assessments were discussed and agreed upon as a group. Preoperative fracture classification was based on the description by Saxena et al.8 Type I fractures involved only the dorsal cortex. Type II fractures extended from the dorsal cortex into the navicular body. Type III fractures extended completely from the dorsal cortex through a second cortex (plantar, medial, or lateral).
Fracture location in the axial plane was described as lateral, central, or medial third. Postoperative imaging, including radiographs and CT, was reviewed to assess for fracture union and avascular necrosis. CT was routinely obtained prior to advancement of weight-bearing, at or around 12 weeks postoperatively. Patients were then contacted prospectively, consent was obtained, and patients completed outcome surveys, including pre-injury primary sport participation, post-surgery and current sports participation, pain, navicular refracture, and additional surgeries.
Surgical Technique
The surgeries were performed by one of two surgeons with the same surgical technique. A small incision was made over the lateral aspect of the navicular to facilitate percutaneous fixation of the stress fracture. The fracture site itself was not formally opened, except for one patient whose imaging was concerning for AVN. In this case, bone grafting with calcaneal autograft was performed in addition to fixation. Guide pins were placed from dorsal lateral to plantar medial using multiple fluoroscopic views to ensure correct guide pin trajectory. Guide pins were placed as perpendicular to the fracture as possible. The guide pins were drilled, and then two partially threaded screws were placed to compress the fracture. Patients were treated with solid titanium screws ranging from 2.5–4.0 mm in diameter.
Results
Patient Demographics
Five patients, four males and one female, with a median age of 15.8 years (range 14-17 years) were included. All were athletes at the time of their injuries, with primary sports including baseball (three patients), soccer (one patient), and basketball (one patient). Median duration of symptoms prior to presentation was 47 days (range 1-92 days). One patient, a 15-year-old male who had recently returned to sports following a 4th metatarsal stress fracture, had a sudden onset of pain 1 day prior to presentation. This patient’s stress fracture was felt to result from his rapid return to sports following recent immobilization and protected weight-bearing for his metatarsal stress fracture. The other four patients all had greater than 30 days of pain prior to diagnosis. Patient demographics and fracture characteristics are listed in Table 1.
Table 1. Patient Demographics and Fracture Characteristics
| Age | Sex | Sport | Duration of Symptoms (days) | Saxena Classification | Initial Nonoperative Management | |
|---|---|---|---|---|---|---|
| 1 | 14 | M | Baseball | 62 | III | No |
| 2 | 16 | M | Baseball | 47 | II | NWB, boot x 6 weeks |
| 3 | 15 | M | Baseball, Football | 1 | III | No |
| 4 | 15 | F | Soccer | 92 | III | No |
| 5 | 17 | M | Basketball | 35 | II | NWB, boot x 6 weeks |
NWB = non-weight-bearing.
Imaging Results
All patients had plain radiographs at the time of initial presentation. The navicular stress fracture was visible on plain radiographs in only one patient. Three patients were noted to have a dorsal navicular osteophyte on radiographs. Advanced imaging was obtained in all patients, including MRI and CT in three patients, MRI in one patient, and CT in one patient. All fractures were in the lateral third of the navicular. There were two type II fractures and three type III fractures. Figures 1 and 2 highlight the pertinent preoperative and postoperative imaging of two individual cases.
Figure 1. Patient 2, a 16-year-old male baseball catcher with 7 weeks of midfoot pain. A. AP and Lateral radiographs of the foot with dorsal navicular osteophyte but no apparent fracture. B. MRI with a lateral third type II NSF. C. CT at 10 weeks postop with healed fracture. D. Radiographs at 3 months postop with healed fracture.
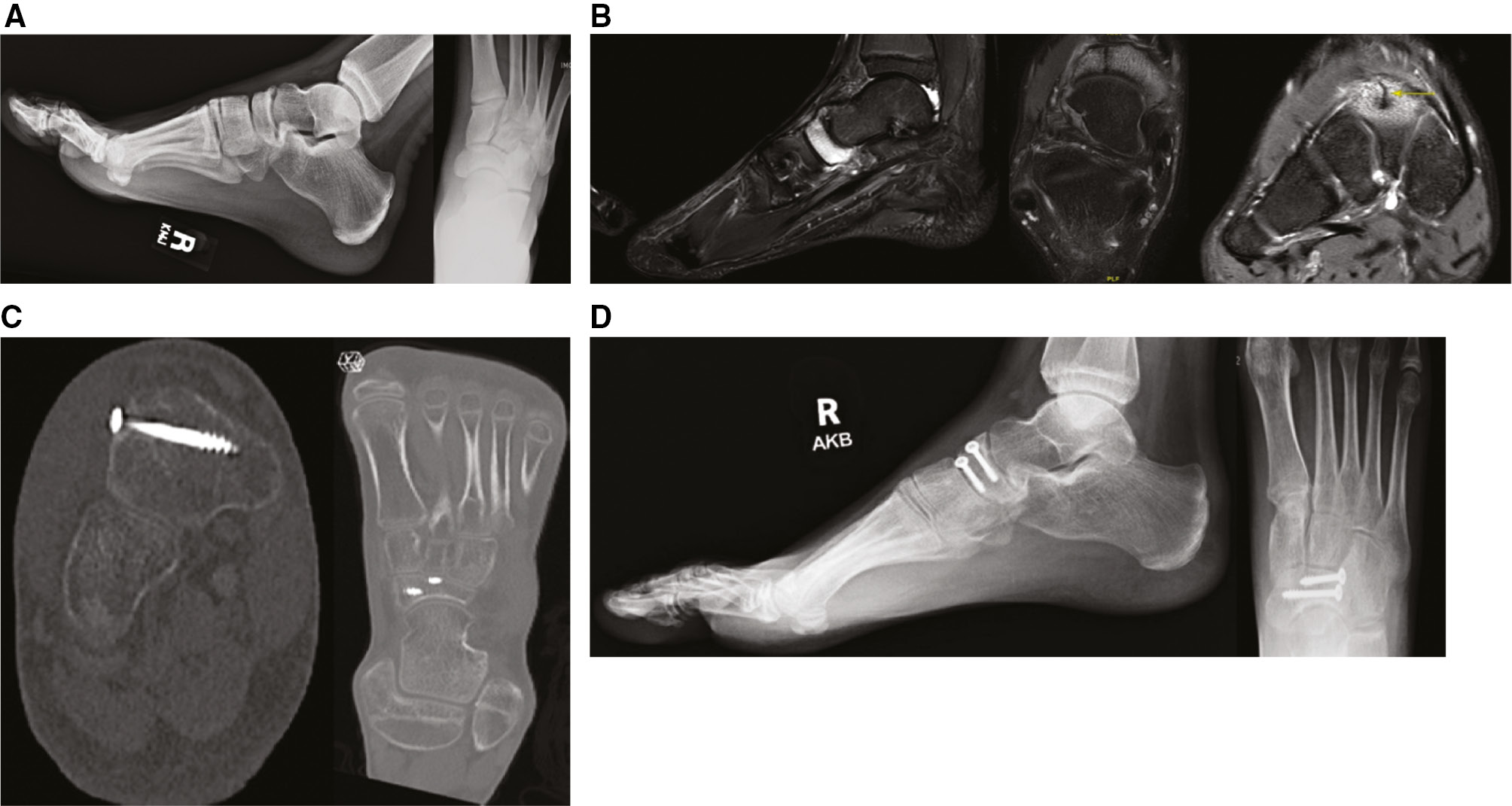
Figure 2. Patient 3, a 15-year-old male baseball catcher with acute onset of pain after returning to baseball and football following a period of immobilization and protected weight-bearing for a 4th metatarsal stress fracture. A. Radiographs demonstrating complete navicular stress fracture. B. CT with lateral third type III NSF. C. CT at 12 weeks postoperative with incomplete healing of the dorsal cortex. D. Radiographs at 7 months postop with healed stress fracture.

Treatment Details
The two patients with type II fractures were initially treated nonoperatively with strict non-weight-bearing restrictions and cast immobilization. Follow-up imaging at 6 weeks demonstrated no evidence of healing and surgical treatment was indicated. These patients underwent ORIF at a median of 45 days following presentation. Three patients with type III fractures were indicated for surgery at the time of presentation and underwent ORIF at 12- and 14-days following presentation. The fracture site was opened in only one patient (Case 3), a 14-year-old male with fragmentation at the fracture site in CT and concern for early AVN. After debridement, the fracture was bone grafted with calcaneal autograft and then fixation was placed. Dorsal navicular osteophyte excision was performed in all three patients where this was present. All patients were casted postoperatively for 6 weeks and non-weight-bearing (NWB) restrictions were maintained for a median of 12 weeks (range 10-16 weeks). Four patients utilized a bone stimulator postoperatively.
Clinical Outcomes
A CT scan was routinely obtained 8-12 weeks postoperatively to assess fracture healing prior to advancement of weight-bearing and this was completed in four patients. Complete fracture healing was noted in three patients while two had near complete healing with the exception of the dorsal cortex (Case 2 and 3). No patient developed avascular necrosis. Patients were released to full activities at a median of 24 weeks (range 19-30 weeks) following surgery. Median follow-up was 30 weeks (range 21-61 weeks) Hardware was not removed. There were no refractures or hardware failure during clinical follow-up.
Patient Reported Outcomes
All five patients were contacted via phone and completed patient reported outcome measures at a median of 61 months (range 18-76 months) following surgery. All patients returned to their primary sport at the same or a higher level. Four patients reported that they experienced no pain in their foot. One patient (Case 5), a high school soccer and cross-country athlete, was a current collegiate cross-country runner and noted an occasional ache in her foot with running. Of the two patients with incomplete healing on postoperative CT, neither had any pain or limitations in activities. No patients reported any refractures or subsequent surgeries.
Discussion
This study serves as the first to evaluate the fracture characteristics and outcomes of surgical management of a small series of operatively treated navicular stress fractures in adolescent athletes. Our series of adolescent patients with type II and III NSF were successfully treated with ORIF, returned to their primary sport, and had no complications.
The diagnosis of navicular stress fracture is frequently delayed, and patients may present with symptoms for weeks to months. Adult patients present at an average of 6-7 months after symptom onset.11,12 Our cohort, however, presented with an average of 6 weeks of symptoms, which may be attributable to the adolescent athlete population and the demands of their sports. As symptomatology can be vague, it has been recommended to palpate the “N-spot,” the high point of the navicular where it articulates with the talus for tenderness.6,12 Along with tenderness, all three baseball catchers in our study were found to have a dorsal navicular osteophyte. In the appropriate clinical setting with pain in the area of the navicular, the presence of a dorsal navicular osteophyte should heighten concern for a navicular stress fracture. We have theorized that a catcher’s frequent squatting and rising from a crouched position may result in frequent loading and altered joint mechanics in the talonavicular joint, prompting osteophyte formation. Talonavicular arthritis was noted to be present among 75% of NFL players diagnosed with a navicular stress fracture,13 again highlighting the altered mechanics in this area which likely contribute to the stress fracture.
In the adult population, both operative and nonoperative management of NSF has been described. In an early study evaluating treatment of NSF, Torg et al. showed success with nonoperative management consisting of NWB cast immobilization for 6-8 weeks followed by gradual weight-bearing in a boot until pain free.12 All 10 patients treated in this manner went on to healing without complication. Similar positive results were seen by Khan et al., with 86% of patients following this protocol returning to full activity at a mean of 5.6 months.7 However, compliance to strict and prolonged non-weight-bearing is vital in order to minimize the risk of a poor outcome. In the same study, Khan et al. showed only 26% of patients treated with walking casts returned to full activity. A more recent meta-analysis noted that 96% of NSFs initially treated with 6 weeks of NWB in a cast had a successful outcome, compared to only 47% treated with activity limitation but continued weight-bearing.9
Indications for surgical treatment of NSF are varied and have mixed results. In 1989, Fitch et al. reported on surgical treatment including en bloc resection of the fracture ends and autogenous bone grafting without internal fixation.13 Despite this aggressive surgical approach, only 12 of 15 patients with adequate follow-up were able to return to pre-injury level of play at a mean of 8 months postoperatively. Kahn et al. reported on successful outcomes for only 12 of 20 patients treated with surgery.7 However, this study includes adults and did not distinguish between fracture patterns or severity in relation to treatment.
Recognizing the need for a more algorithmic approach to NSF, Saxena et al. developed a fracture classification to guide treatment based on the amount of fracture propagation as seen on CT imaging.8 The authors recommended NWB casting for type I (fracture just through dorsal cortex) and ORIF for type II (fracture extending into navicular body) and type III (fracture completely propagating to a second cortex) fractures. When evaluating the results of ORIF for type II and III fractures, >90% of patients were able to return to activity, including all 21 elite level athletes in their most recent study.6,10 All athletes in our study successfully returned to their sport, including two at the collegiate level.
Large prospective comparison studies are required to make meaningful comparisons and distinctive conclusions between operative and nonoperative management, yet given the rarity of NSF, these data are lacking. In a comparative study with a total of 26 adult patients, Potter et al. showed minimal difference in functional outcomes or pain scores between nonoperative treatment at an average of 10-year follow-up.14 In a meta-analysis reviewing 200 NSF (median age mid-20s), Mallee et al. noted an earlier return to sport for surgical management as compared to nonoperative management (mean time of 16 weeks in the surgically treated patients and 22 weeks in patients treated with non-weight-bearing casts).15 Gross et al. recommend treatment based on CT findings, athletic participation level, and patient’s functional status, with surgical management recommended for type II and III fractures and athletes wishing to return to sports more quickly.16
Both operative and nonoperative treatment have potential complications. One concern with nonoperative management is the risk of refracture, especially in an active adolescent population. In their cohort, Saxena et al. noted 8/62 (13%) NSF were refractures in patients previously treated nonoperatively.10 The majority of refractures occurred in patients under 21 years of age and refracture was significantly associated with an inability to return to the desired level of sport.
Delayed union and nonunion can occur with either operative or nonoperative treatment. Nonunion is more common in patients treated without prolonged weight-bearing restrictions.7,12 As clinical and radiographic assessment of healing can be difficult, postoperative advanced imaging is recommended and is our standard practice at an average of 3 months postoperatively.17 While the authors acknowledge that only 50% of the patients had evidence of complete fracture healing at a mean of 3 months, the main use of the CT scan is to establish if enough healing has occurred to advance weight-bearing. As was seen in our cohort, a lack of complete healing at these early timepoints is not an uncommon occurrence. In a review of 55 CT scans for NSF, only 32% of fractures showed firm cortical union at 4 months of treatment.18 Potter et al. also noted some CT scans to show a persistent cleft at the dorsal fracture site even on 10-year follow-up imaging without clinical significance.14 Given these previously published findings, combined with the desire to avoid unnecessary radiation exposure in the adolescent population, additional CT scans were not pursued to document 100% union.
The main limitation of the study is the small cohort size. Ideally, a prospective study with a large number of patients, including a comparison group of patients treated nonoperatively, would be available for study. However, given the low incidence of NSF, this is not possible in a single center study. Although a multicenter case series would increase the total number of patients, in a retrospective fashion this is significantly limited by heterogeneity of surgeons, technique, postoperative rehabilitation, and return to sport protocols. Despite this limitation, the authors feel that the current study has value for the orthopaedic surgeon treating adolescent NSF, as no other similar study in this age-group is available provide insight into treatment outcomes.
Conclusion
A high index of suspicion for NSF is required for prompt diagnosis and treatment. The extent of fracture propagation on advanced imaging guides nonoperative vs. operative treatment. Among our cohort of adolescent athletes with type II and III navicular stress fractures, for which operative treatment is historically recommended, operative treatment results in full return to sports, excellent midterm outcomes, and no evidence for refracture.
Disclaimer
S. C. Willimon: Consultant for Smith & Nephew and Vericel. The remaining authors have no conflicts of interest to disclose.
References
- Marshall D, MacFarlane RJ, Molloy A, et al. A review of the management and outcomes of tarsal navicular fracture. Foot Ankle Surg. 2020;26:480–486.
- Sammarco VJ. The talonavicular and calcaneocuboid joints: anatomy, biomechanics, and clinical management of the transverse tarsal joint. Foot Ankle Clin. 2004;9:127-145.
- Sangeorzan BJ, Benirschke SK, Mosca V, et al. Displaced intra-articular fractures of the tarsal navicular. J Bone Joint Surg Am. 1989;71:1504-1510.
- Ramadorai MU, Beuchel MW, Sangeorzan BJ. Fractures and dislocations of the tarsal navicular. J Am Acad Orthop Surg. 2016;24:379-389.
- Kitaoka HB, Luo ZP, An KN. Contact features of the talonavicular joint of the foot. Clin Orthop Relat Res. 1996:290-295.
- Saxena A, Fullem B. Navicular stress fractures: a prospective study on athletes. Foot Ankle Int. 2006;27:917-921.
- Khan KM, Fuller PJ, Brukner PD, et al. Outcome of conservative and surgical management of navicular stress fracture in athletes. Eighty-six cases proven with computerized tomography. Am J Sports Med. 1992;20:657-666.
- Saxena A, Fullem B, Hannaford D. Results of treatment of 22 navicular stress fractures and a new proposed radiographic classification system. J Foot Ankle Surg. 2000;39:96-103.
- Torg JS, Moyer J, Gaughan JP, et al. Management of tarsal navicular stress fractures: conservative versus surgical treatment: a meta-analysis. Am J Sports Med. 2010;38:1048-1053.
- Saxena A, Behan SA, Valerio DL, et al. Navicular stress fracture outcomes in athletes: analysis of 62 injuries. J Foot Ankle Surg. 2017;56:943-948.
- Mann JA, Pedowitz DI. Evaluation and treatment of navicular stress fractures, including nonunions, revision surgery, and persistent pain after treatment. Foot Ankle Clin. 2009;14:187-204.
- Torg JS, Pavlov H, Cooley LH, et al. Stress fractures of the tarsal navicular. A retrospective review of twenty-one cases. J Bone Joint Surg Am. 1982;64:700-712.
- Fitch KD, Blackwell JB, Gilmour WN. Operation for non-union of stress fracture of the tarsal navicular. J Bone Joint Surg Br. 1989;71:105-110.
- Potter NJ, Brukner PD, Makdissi M, et al. Navicular stress fractures: outcomes of surgical and conservative management. Br J Sports Med. 2006;40:692-695; discussion 5.
- Mallee WH, Weel H, van Dijk CN, et al. Surgical versus conservative treatment for high-risk stress fractures of the lower leg (anterior tibial cortex, navicular and fifth metatarsal base): a systematic review. Br J Sports Med. 2015;49:370-376.
- Gross CE, Nunley JA, 2nd. Navicular stress fractures. Foot Ankle Int. 2015;36:1117-1122.
- Pavlov H, Torg JS, Freiberger RH. Tarsal navicular stress fractures: radiographic evaluation. Radiology. 1983;148:641-645.
- Kiss ZS, Khan KM, Fuller PJ. Stress fractures of the tarsal navicular bone: CT findings in 55 cases. AJR Am J Roentgenol. 1993;160:111-115.